

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rhinitis is classified as allergic rhinitis or nonallergic rhinitis based on systemic atopy to aeroallergens. Recently, the concept of local allergic rhinitis has been raised, and interest in this concept is increasing. Local allergic rhinitis is defined as a localized nasal allergic response and absence of systemic atopy. For diagnosis, nasal-specific immunoglobulin E (IgE) should be detected or nasal allergen provocation test proved positive.
Currently used methods for detecting nasal-specific IgE required administration of large amounts of isotonic saline into the nostrils, which is difficult in children.
We designed two methods that are easy to use in children: a spray method and a swab method. Using these methods, we measured nasal-specific IgE and evaluated the clinical characteristics of nasal-specific IgE in pediatric rhinitis.
MATERIALS AND METHODS
This study included 82 patients who visited Kyungpook National University Children's Hospital from December 2014 to July 2016. They visited with rhinitis symptoms (rhinorrhea, nasal obstruction, nasal itching, and sneezing) and were diagnosed with allergic rhinitis or nonallergic rhinitis. We defined patients with positive skin prick test as having allergic rhinitis. We used the methods described below for collecting nasal secretions with them. Thirty patients used the spray method (spray group), and 52 patients used the swab method (swab group). We used the swab method from December 2014 to December 2015 and the spray method from January to July 2016.
Measuring nasal sample
Measuring nasal sample came from methods of measuring virus-specific IgA (1). The spray method involves slowly spraying 5 mL of isotonic saline as a fine mist into each nostril using an electronic nasal spray device named New Coclean (WelbuTech, Incheon, Korea) and collecting the diluted nasal secretions. The swab method involves inserting a cotton swab until resistance is met at turbinates and rotating the swab several times against nasal wall and then washing the cotton swab tip with 1.25 mL of isotonic saline in a tube. We then examined the fluid for the presence of nasal-specific IgE to Dermatophagoides farinae, Dermatophagoides pteronyssinus, Alternaria, birch, and weed mix via an ImmunoCAP radioallergosorbent technique (UniCAP; Pharmacia, Uppsala, Sweden). We also examined the fluid for nasal total IgE.
Serum total IgE, specific IgE, and eosinophil count
We measured serum-specific IgE for aeroallergens (D. farinae, D. pteronyssinus, Alternaria, Aspergillus, cat dander, and dog dander) and serum total IgE using the ImmunoCAP. Serum-specific IgE concentrations ≥ 0.35 kIU/L were considered positive. Peripheral blood total eosinophil counts were checked using an automated system.
Skin prick test
Skin prick tests for allergen were performed using 17 allergen extracts. Histamine was used as the positive control, and isotonic saline was used as the negative control. After 15 minutes, a wheal and flare reaction equal to the negative control was considered negative. A wheal reaction of more than 3 mm was considered positive.
Statistical analysis
Qualitative variables are expressed as percentages. Quantitative variables are expressed as means and standard deviations or as median from minimum to maximum. Ages are expressed as means. Serum total IgE, specific IgE, eosinophils and eosinophil cationic protein (ECP) are expressed as median. The relationships between serum specific IgE and nasal-specific IgE were examined using Pearson correlation analysis. Receiver operating characteristic (ROC) curve analysis was used to determine the nasal-specific IgE cutoff point with optimal sensitivity and specificity. All statistical analysis was performed using PASW Statistics version 18.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
RESULTS
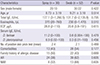
The average age of all 82 patients was 9.04 ± 3.17 years. Twenty of the spray group were boys, and ten were girls, with an average age of 8.73 ± 3.19 years. Twenty-four patients in the spray group were allergic rhinitis patients, and six were nonallergic rhinitis patients. Thirty of the swab group were boys, and twenty-two were girls, with an average age of 9.21 ± 3.18 years. Thirty-nine patients of the swab group were allergic rhinitis patients, and thirteen were nonallergic rhinitis patients. There were no significant differences in serum total IgE, serum specific IgE, serum eosinophil counts, ECP, the numbers of positive skin prick test results, the numbers of comorbidities and the numbers of family history of allergic disease between the spray and the swab groups (Table 1).
Table 1
Demographics of subjects
Thirty of all patients, all of whom had allergic rhinitis, had nasal-specific IgE concentrations of ≥ 0.35 kIU/L. Twenty-one of these patients were boys, and nine were girls, with an average age of 9.17 ± 2.83 years.
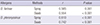
There was a positive correlation between nasal-specific IgE and serum-specific IgE to D. farinae in all patients (r = 0.548, P < 0.001). Dividing two groups, there was a positive correlation between nasal-specific IgE and serum-specific IgE to D. farinae in the spray group (r = 0.585, P = 0.001) and there was a positive correlation in the swab group (r = 0.554, P < 0.001) (Table 2). There was also a positive correlation between nasal-specific IgE and serum-specific IgE to D. pteronyssinus in all patients (r = 0.656, P < 0.001). There was a positive correlation between nasal-specific IgE and serum-specific IgE to D. pteronyssinus in the spray group (r = 0.610, P < 0.001) and there was a positive correlation in the swab group (r = 0.742, P < 0.001) (Table 2).
Table 2
Correlation of nasal-specific IgE and serum-specific IgE to D. farinae and D. pteronyssinus in the spray and the swab group
| Allergens | Methods | r | P value |
|---|---|---|---|
| D. farinae | Spray | 0.585 | 0.001 |
| Swab | 0.554 | < 0.001 | |
| D. pteronyssinus | Spray | 0.610 | < 0.001 |
| Swab | 0.742 | < 0.001 |
The proportion of patients with nasal-specific concentrations of IgE to D. farinae ≥ 0.35 kIU/L in the serum-specific IgE-positive group was 66.7% as measured using the spray method and 46.7% using the swab method. The proportion of patients with nasal-specific concentrations of IgE to D. pteronyssinus ≥ 0.35 kIU/L in the serum-specific IgE-positive group was 38.1% using the spray method and 31.6% using the swab method. There was no statistically significant difference between the groups.
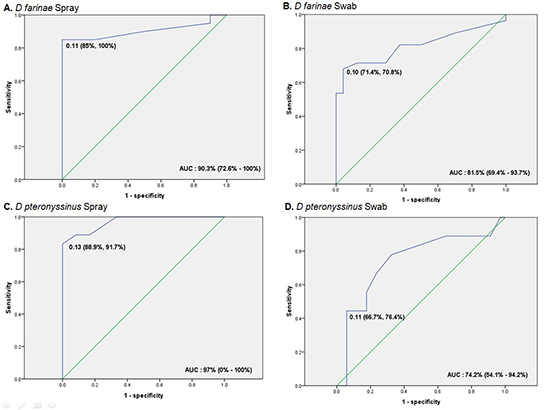
If we regard positivity of skin prick test as the standard, the cutoff point of nasal-specific IgE to D. farinae was 0.11 kIU/L using the spray method and 0.10 kIU/L using the swab method. The sensitivity of the spray method for D. farinae was 85.0%, and the specificity was 100%. The sensitivity of the swab method for D. farinae was 71.4%, and specificity was 70.8% (Table 3).
Table 3
Cutoff points and AUCs for spray and swab methods

The cutoff point of nasal-specific IgE to D. pteronyssinus was 0.13 kIU/L using the spray method and 0.11 kIU/L using the swab method. The sensitivity of the spray method for D. pteronyssinus was 88.9%, and the specificity was 91.7%. The sensitivity of the swab method for D. pteronyssinus was 66.7%, and the specificity was 76.4% (Table 3).
Based on these cutoff points, five of our patients would be regarded as having local allergic rhinitis. These patients were negative for serum specific IgE and skin prick test result and their nasal specific IgE concentrations were higher than our cutoff point in more than one allergen.
DISCUSSION
Local allergic rhinitis is characterized by local production of nasal-specific IgE without systemic atopy. The prevalence of local allergic rhinitis is unknown. Previous studies have reported the prevalence of local allergic rhinitis to be 47%–62.5% in patients with nonallergic rhinitis (234). In some studies reporting local allergic rhinitis in children and adolescents, 11% of the patients were aged < 14 years at clinical evaluation and 14% first reported symptoms in childhood (567). In our study, the prevalence of local allergic rhinitis based on our cutoff points was 6.1%.
Previous studies reported clinical characteristics of local allergic rhinitis (4689). Local allergic rhinitis patients are younger than nonallergic rhinitis patients and are predominantly women (6). Patients with local allergic rhinitis had a family history of atopy and more frequent conjunctivitis and asthma among allergic diseases (468). The most common symptoms are rhinorrhea, sneezing, and itching (48). A study of allergic rhinitis patients reported no significant difference in age or sex between the nasal provocation test-positive group and nasal provocation test-negative group (9).
Many tests have been used to measure nasal-specific IgE and diagnose local allergic rhinitis (891011). The nasal provocation test is considered the gold standard for diagnosing local allergic rhinitis (89). However, nasal provocation tests are time consuming and require a free interval between two allergens. Furthermore, there is a risk of anaphylactic shock (89). Nasal lavage for measuring nasal-specific IgE is another method for diagnosing local allergic rhinitis (810). This method is noninvasive, but the sensitivity is relatively low (810). One study reported that nasal IgE had a correlation rate of 90% with the nasal provocation test (11). However, the serum IgE and skin prick tests had correlation rates of 72.5% and 67.5% with the provocation test (11). This study suggested that the high correlation rate of nasal IgE with the nasal provocation test indicates that the nasal test is a safe and practical alternative to the nasal provocation test (11).
Our study presents two methods to evaluate nasal-specific IgE that are neither time consuming nor expensive. These methods came from methods of measuring virus-specific IgA (1). Previous study reported that nasal washing method was good to collect nasal secretions and determine ECP (12). The spray and swab methods can be conducted easily in children and had relatively high positivity. Furthermore, the nasal-specific IgE collected using these methods reflected the serum-specific IgE relatively well.
Although we measured nasal total IgE and nasal-specific IgE to prevalent inhalant allergens including D. farinae, D. pteronyssinus, Alternaria, birch and weed mix, only nasal-specific IgE to D. farinae and D. pteronyssinus were measured in all patients and other allergens showed very low positivity, so we only described about nasal-specific IgE to D. farinae and D. pteronyssinus.
A nasal-specific IgE-positive standard value has not yet been established. A study performed in Spain determined that the optimal cutoff point to discriminate local allergic rhinitis subjects from controls was 0.085 kIU/L (13). This study used the ImmunoCAP solid phase applied directly in the lower turbinate of each nostril (13). Our study examined the optimal cutoff point of the nasal-specific IgE value using the ROC curve. In our study, the cutoff point of nasal-specific IgE value for D. farinae was 0.11 kIU/L and D. pteronyssinus was 0.12 kIU/L. The previously mentioned study evaluated nasal-specific IgE in patients with allergic rhinitis, local allergic rhinitis, and healthy controls and identified a cutoff point to discriminate local allergic rhinitis from controls (13). However, our study evaluated nasal-specific IgE in patients with allergic rhinitis and nonallergic rhinitis and determined the cutoff point based on positivity of skin prick test.
The limitations of our study are as follows. First, we evaluated nasal-specific IgE only in nasal fluid and diagnosed local allergic rhinitis according to the results for the nasal-specific IgE. To establish an exact cutoff value for diagnosing local allergic rhinitis, a nasal provocation test is needed. Second, we used only one of the two methods in each patient. If both of the methods could be conducted in the same patient, we could compare the results of the two methods and choose the better one. Third, we used each method during different periods. Although different periods may affect the results of the study, the results may be little affected because this study focused on the perennial allergens. Fourth, our study is a small-scale retrospective study. For exact evaluation of the prevalence of local allergic rhinitis in children and accuracy of the optimal cutoff value of nasal-specific IgE, a large-scale prospective study is needed.
In summary, our study presents two methods to evaluate nasal-specific IgE. If we establish a positivity standard, these methods can be used to diagnose local allergic rhinitis in children. Further large-scale studies combined with nasal allergen provocation tests are needed.
 XML Download
XML Download