

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic infection of auditory tube diverticula, and subsequent empyema and chondroid formation, is well described in the horse [910]. Variable success has been reported with medical therapy [11319]. Treatment failures have been attributed to chronic inflammation and inadequate drainage from the nasopharyngeal ostium of the auditory tube [7]. Surgical fenestration into the auditory tube diverticulum has been applied to facilitate lavage, allow direct removal of chondroids, and encourage continuous drainage. Transcutaneous approaches to an auditory tube diverticulum have been criticized because of the proximity of multiple nerves and risk of inadvertent nerve injury [45]. Minimally invasive transpharyngeal surgical approaches have been advocated for treatment of diseases of auditory tube diverticula to decrease the risk of collateral injury and simplify wound management by owners in the post-operative period [6711121617].
Despite its common application, transpharyngeal endoscopic auditory tube diverticulotomy has not been fully described. Therefore, the aim of the present study was to compare two transpharyngeal endoscopic auditory tube diverticulotomy locations and describe the relative anatomy, duration, and incision properties for each surgical approach.
Materials and Methods
Ten horses enrolled in a separate research protocol approved by the Colorado State University Institutional Animal Care and Use Committee (IACUC 15-5769A) in compliance with the US National Institutes of Health Guide for the Care and Use of Laboratory Animals, the Animal Welfare Act, and the Federation of Animal Science Societies Guide for the Care and Use of Agricultural Animals in Research and Teaching were studied. Horses were humanely euthanized with an overdose of intravenous sodium pentobarbital (86 mg/kg) and heads were immediately collected by sharp dissection between the second and third cervical vertebrae. Specimens were stored at 5℃ until surgery, which was performed within 6 h of euthanasia.
Heads were positioned in a manner similar to that in standing transendoscopic surgery and were randomly assigned to a surgical technique. Distances between the left and right medial canthus and from the medial canthus to the ipsilateral nostril were measured. A one-meter flexible videoendoscope (Olympus, USA) was passed via the ventral nasal meatus into the nasopharynx and a flexible surgical ruler (Aspen Surgical, USA) attached with clear adhesive tape to the end of an equine uterine infusion pipette (Jorgensen Labs, USA) was introduced to obtain measurements of the dorsal pharyngeal recess (DR). The ruler was placed within the recess by allowing it to flex; measurements were made to the nearest millimeter.
Surgical procedure
Horses were grouped to undergo right and left transpharyngeal endoscopic auditory tube diverticulotomy either at a single DR (n = 5) location, or bilaterally caudal to the nasopharyngeal ostium (CNO; n = 5). All incisions were created with a surgical diode laser and a single surgeon created all laser fenestrations. A 600 µm quartz fiber attached to a 980 nm wavelength surgical diode laser (Ceralas D 50; Biolitec, Germany) was passed within the working channel of the endoscope and activated in a position approximately 2 to 3 cm from the endoscope tip. For all surgeries, a laser setting of 25 W was used, and the laser was applied in contact mode. An initial cut created at the border of the diverticulotomy was deepened with repetitive, linear motions until incisions were complete. Laser energy, laser activation time, and procedure duration were recorded. Entrance into both right and left auditory tube diverticula was visually confirmed endoscopically in each horse specimen. Each procedure was performed by a right-hand dominant surgical resident and video recorded. Distance of insertion of the endoscope for each procedure, defined as the length between the endoscope tip and the point that the endoscope exited the nares, was recorded.
For specimens assigned to auditory tube diverticulotomy at the DR location, the endoscope was placed via the ventral nasal meatus through a nostril selected at random (right, n = 2; left, n = 3), and a rectangular incision was created starting at the dorsal border of the recess and continuing around its borders, crossing the median septum at the dorsal and ventral aspects of the fenestration (Fig. 1). When approximately 90% of the diverticulotomy had been performed, equine laryngeal forceps (Karl Storz Endoscopy-American, USA) were inserted through the nostril contralateral to endoscope insertion and used to hold the central tissue within the rectangular fenestration and facilitate laser excision of the grasped tissue from the auditory tube diverticula median septum prior to removal.
For specimens assigned to auditory tube diverticulotomy at the CNO location, an equilateral triangular incision with an approximate 2 cm side length was created bilaterally midway between the nasopharyngeal ostium and the DR (Fig. 1). Creation of the triangular incision was facilitated by passage of the endoscope via the contralateral nostril. The first incision was oriented parallel to the plica salpingopharyngeus and was the rostral boundary of the fenestration. The remaining incisions joined the dorsal and ventral rostral incision borders and were directed toward the central DR. When approximately 90% of the diverticulotomy had been performed, equine laryngeal forceps (Karl Storz Endoscopy-American) were used to hold the central tissue within the triangular fenestration and facilitate laser excision of the grasped tissue prior to removal.
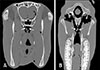
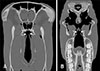
One specimen from each surgical group (DR and CNO) underwent computed tomography imaging using a 16-slice fan-beam scanner (Gemini TF Big Bore PET/CT scanner, helical CT X-ray tube with an 85 cm bore; Philips Healthcare, USA) to identify the location of fenestration sites and relative anatomical structures. All heads were then sectioned with a band saw (Hantover, USA) in the sagittal plane approximately 1 cm from the midline to avoid the median septum and photographed. A digital caliper (Grainger Industrial Supply, USA) was used to measure tissue thickness for each fenestration site after heads were sectioned. For both techniques, measurements were made centrally within the incisional borders of each fenestration, and these measurements were recorded and averaged for each location.
Statistical analysis
Continuous data were examined for normality using the Shapiro-Wilk test, and, if data were normally distributed, they were reported as mean ± SEM. A two-sample t-test was used to compare total laser energy, laser activation time, surgical duration, and tissue thickness at the surgical borders between surgical procedures, as well as to compare the duration of the first two and last two surgical procedures within both DR and CNO groups. Statistical significance was considered to be p < 0.05.
Results
Mean age of horses (n = 10) was 3 ± 0.2 years (range, 2.5–4 years). Five female and five male horses were enrolled, with breeds consisting of four Quarter Horses and six Quarter Horse-crosses. Mean distance between the left and right medial canthus was 20 ± 0.3 cm. Mean distance from the medial canthus to the ipsilateral nostril was 27 ± 0.3 cm. The DR measurements were: height, 2 ± 0.1 cm; width, 1 ± 0.1 cm; perimeter, 6 ± 0.2 cm, and area 2 ± 0.2 cm2. The perimeter of each diverticulotomy performed in the CNO location was 6 cm and the area was 1.7 cm2. Mean endoscopic insertion distance during surgical intervention was 36 ± 0.5 cm for both groups and did not vary between techniques. Laser energy, laser activation time, and procedure duration values are reported in Table 1. The amounts of laser energy and laser activation time, as well as the procedure duration, were greater in the CNO group than in the DR group. Procedure duration did not decrease during the study period in either group (DR, p = 0.41; CNO, p = 0.88), and differences were not observed in perceived diverticulotomy surgical difficulty between the right and left nostrils. Fenestration sites were easily identified on computed tomographic images of the horse head specimens. In the transverse plane, complete communication between the nasopharynx and auditory tube diverticula was observed for both the DR and CNO diverticulotomy locations (Figs. 2 and 3, respectively). On gross examination, communication between the nasopharynx and the auditory tube diverticula was clearly visible in all specimens. The tissue thickness at the fenestration border was greater in the CNO group than in the DR group (Table 1).
Discussion
The present study compared two minimally invasive transpharyngeal endoscopic auditory tube diverticulotomy techniques in horse head specimens. The techniques differed in the location of the diverticulotomy, tissue thickness at the incision site, laser energy quantity, laser activation time, and surgical duration. Both surgical methods resulted in communication between the pharynx and the auditory tube diverticula, visible during endoscopic, computed tomography, and gross examination. Compared to diverticulotomy performed CNO, diverticulotomy performed in the DR required approximately half the laser energy quantity and half the laser activation time. The lower laser energy and activation time required for the DR diverticulotomy is likely related to the single incision required to access both auditory tube diverticula in the DR group. Another contributing factor was that the tissue thickness of the diverticulotomy sites located CNO was nearly five times that at the DR location. However, the CNO diverticulotomy resulted in a larger fenestration into each auditory tube diverticulum than that in specimens undergoing DR diverticulotomy. Both methods were performed by a surgical resident in training without prior experience in laser surgery and, as the time did not decrease throughout the study, the techniques were not considered difficult.
The function of auditory tube diverticula, found in equids, some bats, and a few other mammalian species, has not been fully elucidated [258]. The anatomy of such diverticula is complex, which results in an array of unique disease processes in the horse [4]. Drainage of this site is dependent on a small opening, which is located on the rostral and dorsal aspects of the diverticula when the horse's head is in the neutral position. The long-term clinical significance of creating auditory tube diverticulotomies is an area of interest, especially whether the presence or size of a permanent fenestration has health impacts on the horse. How much the size of the fenestrations will decrease with healing or whether a predictable patency can be achieved is unknown. Previous work has shown that while some fenestration sites heal, others remain patent on follow-up [6719]. One study hypothesized that fenestration within the guttural pouch can alter the local environment triggering the resolution of mycosis [19]. Despite these questions, it is apparent that diverticulotomy is therapeutic when applied to selected primary diseases of the guttural pouch, including tympany, empyema, and chondroids [79].
There are apparent advantages and disadvantages of transendoscopic laser auditory tube diverticulotomy. Advantages of a transpharyngeal minimally invasive approach over transcutaneous open approaches include reduced risk of iatrogenic cranial nerve damage, avoidance of postoperative wound maintenance by horse caregivers, and requirement of light sedation to complete the procedure [671719]. However, disadvantages include the need for specialized equipment and the loss of endoscopic visualization due to hemorrhage, which can occur with laser surgery of the upper respiratory tract [367]. Specific technique selection for clinical application will likely vary with surgeon preference and the disease process undergoing treatment. The goals of treatment for tympany are to allow egress of air from the diverticula, in the face of nasopharyngeal ostium dysfunction [111214151618]. For tympany, diverticulotomy in the DR location is a lower energy strategy, as we have demonstrated, and accomplishes bilateral fenestration with a single incision. The goals of treatment for empyema are to allow lavage and continuous egress of fluid from the diverticula, permitting resolution of inflammation and preventing chondroid formation [9]. Likely, either of the described diverticulotomy strategies would promote fluid evacuation from this region as, regardless of surgical location, either fenestration site would allow drainage. Based on clinical experience, once chondroid formation has occurred, removal is more easily facilitated by larger fenestrations, therefore a CNO-located diverticulotomy might be more appropriate for this disease process. To ensure an unrestricted trajectory for instrument insertion and chondroid removal, the surgical incisions should be located below the plica salpingopharyngeus or the plica could be partially removed. Regardless of which technique is ultimately selected, both transpharyngeal endoscopic auditory tube diverticulotomy approaches evaluated in the present report are considered to have a low risk of iatrogenic nerve or vessel trauma because of the separation between the surgical site and these sensitive structures. This is further supported by previous reports, in which transpharyngeal laser application resulted in successful clinical outcomes [71619].
Endoscopic technology and use of diode lasers have expanded the use of minimally invasive surgical applications in the horse. In our experience, the advantages associated with the application of such technology, including magnified and enhanced visibility within the airway and the ability to finely focus the direction of incisions, in part, justify the associated equipment costs. Despite these advantages, limitations to consider are that the diverticulotomy surgical techniques described do require specific instruments and experience. Although our results showed that surgical time did not shorten with an increased number of operations and that the techniques were feasible for a surgical resident to perform, the use of cadaveric tissues is not an accurate representation of clinical cases. During laser surgery in an equine hospital, movement of the horse can make the creation of incisions more difficult and can increase surgical duration. Undertaking a similar study in standing, sedated horses would allow assessment of operative hemorrhage, comparison of total surgical duration, and provide more information relative to the clinical application of these techniques.
Transpharyngeal endoscopic auditory tube diverticulotomy is straightforward to perform and results in clear communication between the pharynx and the auditory tube diverticula. Incisions located within the DR require significantly less laser energy and laser activation time when compared to bilateral fenestrations located CNO. Further work applying these surgical techniques to horses with diseases of the auditory tube diverticula is warranted.


 XML Download
XML Download