

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the advances in the knowledge and technique of the autologous breast reconstruction, maximum safety as well as surgical efficiency is an important issue nowadays12. At present, various imaging modalities are utilized to plan and facilitate the selection and dissection of perforators345. While the deep inferior epigastric artery (DIEA) is known as anatomically consistent, its perforator (DIEP) varies widely between individuals and sides of the abdomen. Specific anatomic variations have been anecdotally reported, and some variation could affect the difficulty or safety of the operation if unrecognized678910.
Preoperative evaluation using computed tomography angiography (CTA) can reveal variants that might affect surgical planning, thereby either encouraging or discouraging perforator dissection. We categorized some patterns of DIEA/P that would either facilitate or hinder dissection, and analyzed their incidences. We also provided detailed information about the CTA protocol used in our institution including multiplanar reconstruction (MPR) imaging and maximum intensity projection (MIP) imaging reconstruction, and delineated their usage.
MATERIALS AND METHODS
The following protocol was approved by the Institutional Review Board of Asan Medical Center (IRB No. 2017-1033). All patients who underwent immediate autologous-only breast reconstruction using abdominally based free flap between January 2011 and December 2012 were enrolled in this prospective study. CTA was performed 2 or 3 weeks prior to the surgery unless it was contraindicated for medical reasons or refused by the patient.
1. CT protocols
All included patients were preoperatively imaged using a 64-multidetector computed tomography (CT) scanner (Somatom Definition 64; Siemens Medical Solutions, Erlangen, Germany) using the following settings: 120 kVp, effective 200 mAs, 0.5 second gantry rotation time, 512×512 matrix, 3 mm slice thickness, 3 mm slice interval on MPR imaging, 20 mm slice thickness, and 5 mm slice interval on MIP imaging. Intravenous nonionic contrasting agent (100 mL of 400 mg iodine/mL iomeprol: Iomeron®; Bracco, Milan, Italy) was injected at a rate of 4 mL/second. The bolus was tracked through the descending aorta starting at the DIEA. Monitoring was started after a 10 seconds delay, and 1 image was taken every 1.25 seconds. If a threshold of 150 Hounsfield units was reached at the descending aorta, CT was performed after another 10 seconds delay. This delay allowed the distal filling of the peripheral small arteries. The raw data were reconstructed in the axial plane at a 0.75 mm slice thickness and 0.4 mm intervals using standard kernels. The reconstructed images were processed at the workstation (PetaVision for Clinics 2; Asan Medical Center, Seoul, Korea).
2. Perforator identification
This anatomic study was mainly based on the 2-dimensional craniocaudal axial images that were scanned in sequence. Perforators that were distinctly visualized (measured diameter >1 mm) on the MPR protocol image were considered as adequate. Perforating vessels piercing the anterior sheath of rectus abdominis muscle from the level of upper margin of the umbilicus to thirty slices (9 cm) below were identified and traced proximally to the point where the main DIEA emerged from the external iliac artery, approximately at the level of the inguinal ligament.
3. Perforator course classification
Intramuscular part of the vessel referred to the course truly surrounded by rectus muscle, and excluded such part passing immediately under the anterior sheath or under the deep (posterior) surface of rectus muscle enclosed by fatty perivascular tissue that was readily distinguishable from the muscle belly. Perforators that would facilitate dissection were categorized as ‘favorable’ perforators which had no or very short (<1 cm longitudinal length) intramuscular courses. The circummuscular (septocutaneous) perforator did not have any intramuscular course, and thereby either medially or laterally circumvented the muscle (Fig. 1, 2). The perforators with a long subfascial course or a long submuscular course had a very short intramuscular course (<1 cm based on the longitudinal distance of the muscle, or within three CT slices; Fig. 3, 4).
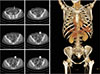
On the contrary, perforators that would hinder or even rule out dissection were categorized as “unfavorable” perforators. The absence of the DIEA meant there was no pedicle enhanced at the level of the inferior margin of the flap, or there was an apparent severance (Fig. 5). The absence of an adequate DIEP meant that there was no distinct perforator that penetrated into the fascia on the MPR image (Fig. 6). Early muscle penetration referred to a DIEA that entered the rectus abdominis muscle right after it emerged from the external iliac artery without coursing under and/or lateral to the rectus abdominis muscle, and soon arborized into smaller branches, which would result in a long cumbersome intramuscular dissection and unusually small vessel caliber for microanastomosis (Fig. 7).
RESULTS
total of 115 patients were included as our study cohort. No patients had previously received radiotherapy, and 5 patients were ex-smokers who quit smoking at least 4 weeks prior to surgery. No patients were diagnosed with peripheral vasculopathy or diabetes. The mean age of the patients were 42.4 years (range, 28–61 years), and the mean weight of the mastectomy specimens was 350.5 g (range, 100–737 g).
Sixty-seven patients had no abdominal scars. Low transverse scars were found in 24 patients, laparoscopic scars in 14 patients, right lower quadrant (appendectomy) scars in 6 patients, and vertical scars in 8 patients. Four patients had more than one scar.
An average number of 3.7 perforators (range, 0–7 perforators) were distinctly visualized in the entire flap territory on MPR-CTA. Table 1 and 2 demonstrated the incidences of patterns of perforator course that were either favorable or unfavorable. Out of 425 perforators, 89 perforators (20.9%) had a favorable course. Most common were long submuscular course followed by direct vertical muscle penetration (51 perforators, 34.8% of the patients) which was twice more common in the lateral row perforators. Long subfascial course was observed in about 15.6% of the patients which was also more commonly observed in the lateral position. Perforators that did not have any intramuscular course were found in 13.9% of the patients. Overall 56.5% of the patients had at least one favorable DIEA/P course.
The incidences of the ‘absence of DIEA’ and ‘absence of adequate DIEP’ were based on the number of hemiabdomen. Three hemiabdomens in three patients with past surgical history was found to have no DIEA available. There was no adequate perforator (>1 mm on the MPR protocol) in 8 hemiabdomen. One patient had no adequate DIEP on either side of her abdomen. Eleven DIEAs showed the pattern of early muscle penetration: two patients had this pattern of DIEA on both sides of their abdomen. These patients were operated with muscle sparing free transverse rectus abdominis myocutaneous (TRAM) flaps.
All preoperatively selected perforators were of adequate size and demonstrated a visible pulse. Of all the DIEP flaps that were actually performed (n=65), 41.5% were based on the medial perforators and 58.5% were supplied by the lateral perforators.
DISCUSSION
The full utilization of various image modalities has been shown to be effective with positive clinical benefits, and CTA is one of the most effective and competitive techniques due to its sensitivity, specificity, availability of 3-dimensional reconstruction, and cost11121314. Our preferred CTA protocol (MPR imaging) might be less sensitive than MIP reconstruction that can clearly visualize almost every available perforator. We mark the perforator that is distinctly visible in ≥1 slice with a measured diameter >1 mm when penetrating the fascia in MPR image. The actual diameter may differ from as observed on CTA, but we have always encountered a perforator with an arterial diameter >1 mm having visible pulse when using this selection criterion15. MIP reconstruction is then utilized to confirm the detailed course of the selected perforators.
Katz et al.16 demonstrated a classification scheme. However, only circummuscular pattern was classified as highly favorable, and only obvious absence of the DIEA was classified as hostile. Ireton et al.17 also categorized some patterns of DIEA perforators through systematic review. Our findings have been anecdotally reported in the literature as uncommon variations or case reports6789. The variations were not uncommonly observed in our present series and aided accurate surgical planning and lead to expeditious and safe harvest of the flap.
We categorized perforators mainly according to their intramuscular course which reflected the convenience of dissection. The circummuscular perforator has been reported as an anatomical variration, with various titles such as subfascial, pararectal, and septocutaneous, with an incidence of as high as 15%. If dissection proceeds in two directions, care should be taken in the anterograde dissection because the lateral circummuscular perforator could be mistaken for a laterally escaping branch1819.
Perforators which transpierced the muscle within three CTA slices (<1 cm) were labeled as having a short intramuscular course. Those perforators have two typical patterns, either a long subfascial course or a long submuscular course, and passed the muscle almost vertically. A perforator with a long subfascial course can be useful when preoperatively recognized. If unrecognized, an inadvertent fascial incision may damage this valuable perforator. A perforator that takes a long submuscular course was relatively common, and the most common point of emersion was at the tendinous intersection of the lateral row. It corresponds with the common saying that the lateral perforators usually followed a short linear intramuscular course.
There were courses that discouraged perforator dissection, including DIEA and/or adequate DIEP absence, and very early entry into the muscle and division into smaller branches. DIEA absence is reported as an anatomic variation or surgical sequela69. We experienced 3 patients with unilateral absence or discontinuity of DIEA, all of whom had low transverse abdominal scarring. All 3 patients had previously undergone a hysterectomy prior to 1995. Whilst a Pfannenstiel incision is theoretically and clinically harmless to DIEA, a Maylard incision routinely severs the rectus abdominis muscle and could potentially damage the vessel20.
We encountered 1 patient who did not have an adequate perforator in either side and thus free musclesparing (MS) TRAM was planned and performed. We believe that MS free TRAM with a small piece of muscle is still a safe and reasonable option when adequate DIEP is not identifiable on preoperative CTA. When carefully selected, free DIEP flaps and muscle sparing free TRAM flap resulted in comparable surgical outcome2122.
One inherent limitation of our study is that this anatomic study is mainly based on CTA images. Although we encountered all the pre-identified perforators intraoperatively, the contralateral side of the flap could only be evaluated by the images. Also smaller perforators that were not visualized in our MPR protocol could not be identified nor classified.
CONCLUSION
In conclusion, preoperative CTA evaluation of DIEA/P can be used to identify favorable as well as unfavorable courses for dissection to aid surgical planning. Overall 56.5% of the patients had at least one favorable DIEA/P course pre-identified by the CTA, most common being long submuscular course followed by long subfascial course.








 XML Download
XML Download