

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fibroma of the tendon sheath is a rare benign soft tissue tumor that typically occurs in the upper extremities, especially the fingers. The most common symptom is a slow-growing mass with no pain or swelling. When it occurs in a finger, finger movement may be limited due to interference with tendon excursion through the flexor pulley system. Moreover, depending on where the tumor occurs, fibroma may also cause localized symptoms such as carpal tunnel syndrome1 or trigger-finger2. Fibroma of the tendon sheath is almost always found adhering to the tendon sheath or tendon3, whereas it is extremely rare to find this tumor within the tendon. Grenga4 reported a case of intratendinous fibroma in a 10-year-old boy presenting with a slow-growing, non-tender mass in the palmar aspect of a finger, which limited finger movement. The mass was 1.5 cm in size and was located within the flexor digitorum profundus (FDP) tendon, interfering with the excursion of this tendon. Closed tears of the FDP tendon in pediatric patients are very rare, whereas cases involving avulsion tear of the FDP tendon are more common5. However, reports of a closed longitudinal tear of the FDP tendon have not been found in the English literature to date. We report the case of a 12-year-old baseball player with a longitudinal partial tear at the FDP finally diagnosed as an intratendinous fibroma.
CASE REPORT
A 12-year-old male baseball player complained of pain in the proximal interphalangeal joint (PIPJ) of the middle finger after a hyperextension injury caused by a baseball impact six weeks previously, which was managed with conservative treatment. Physical examination revealed tenderness and swelling at the palmar side of the PIPJ of the left middle finger. Although passive range of motion showed no limitation, active range of motion was limited (range, 0–70 degrees). There was no triggering.
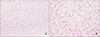
Preoperative radiography revealed no abnormalities, whereas magnetic resonance imaging (MRI) revealed a longitudinal partial tear at the FDP tendon of the left middle finger (Fig. 1). Surgical treatment was planned to allow the patient to return to his sports activity. After making a zigzag skin incision on the palmar side of the middle PIPJ under general anesthesia, the cruciate pulley and parts of the A2 pulley were incised. A longitudinal tear was found in the FDP tendon. Further splitting of the tear revealed a 0.8×0.5×0.5 cm mass (Fig. 2). The mass was well demarcated and was excised easily, followed by tenorrhaphy with continuous suture. Histopathological examination confirmed the mass to be a fibroma (Fig. 3). In the one-month postoperative follow-up, there was no pain in the PIPJ of the middle finger, and the range of motion in the joint returned to normal. In the one-year postoperative follow-up, the patient was able to play baseball without pain. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
DISCUSSION
The most common form of benign soft tissue tumor in the hand is ganglion, followed by giant cell tumor. Fibroma is a very rare form of benign soft tissue tumor. It occurs mostly in patients aged 20–49 years, and its prevalence is twice as high among male than female patients. The diagnosis of fibroma is based on the medical history of the patient and clinical tests; however, radiological examinations such as MRI or ultrasonography may be useful. Plain radiography typically shows negative results; however, positive results may be found when a large mass is compressing the surrounding muscles or fat or when bony erosion is present. Differential diagnoses include epidermal cyst, neurofibroma, nodular fasciitis, leiomyoma, and giant cell tumor. In particular, the clinical features of giant cell tumor and fibroma are very similar to each other. Both types of tumor commonly occur in the fingers, attached to the tendon sheath, and they show similar MRI signal intensity and form a grayish-white multiseptated mass that is hard and well encapsulated. However, a fibroma can be differentiated from a giant cell tumor on the basis of histopathological findings. Fibrotic changes in the matrix of a fibroma are more severe than in a giant cell tumor. Moreover, in fibroma, spindle cells are more abundant, the frequency of giant cells is low, and foam cells and siderophages are rare. Satti6 described fibroma in the tendon sheath as an end or hardening stage of a giant cell tumor that may have been the result of progressive vascular damage. Fibroma may occur anywhere on the limbs; however, it is especially common in the finger, hand, and wrist areas. Millon et al.7 reported that, of 208 hand tumor excision cases in soft tissue over a 15-year period, fibromas of the tendon sheath of the finger flexor tendon accounted for 1%. The relapse rate after tumor excision was ≥24%8. Fibroma that occurs in a finger may interfere with tendon excursion, causing limited movement and triggering9. There has been only one previously reported case of fibroma found within a tendon4; it is typically found as an indolent mass adhering directly to the tendon sheath or the tendon itself37. In our case, a fibroma with a size of 0.8×0.5×0.5 cm, which was too small to be detected by visual inspection alone, was found, and it remained asymptomatic until several finger injuries occurred. It is believed that the finger injury led to the underlying intratendinous fibroma, causing a longitudinal tear of the FDP tendon, which in turn caused limited movement and pain in the finger.
Most cases of closed flexor tendon injury following finger injury in children involve avulsion rupture of the FDP tendon10, which is rare5. Mid-substance rupture of the flexor tendon in adults often occurs when an underlying pathologic condition is present, but it rarely occurs without any underlying pathology5. Traumatic closed mid-substance flexor tendon rupture in children is extremely rare, although Badur et al.5 reported a case of mid-substance flexor tendon rupture that occurred in a 12-year-old child with no underlying pathology. In our case, the underlying pathology of the child was intratendinous fibroma, and this was the first case in which midsubstance longitudinal partial tear was caused by this tumor.
We report one case of a longitudinal partial tear accompanied by an intratendinous fibroma at the FDP tendon of the left middle finger after a hyperextension injury caused by the impact of a baseball. Longitudinal flexor tendon tear in adolescents is extremely rare; when it occurs, the possibility of an underlying pathology should be considered.


 XML Download
XML Download