

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Wissinger et al.1 first described turrets exostosis in 1966 as an outgrowth arising from the dorsum of the fingers following trauma to the involved finger. Although it commonly affects the hands, other sites like talus2, coronoid process3, hallux4. There have been cases reported of the turret exostosis affecting the phalanges of the index, middle and little fingers1567. Although Turrets exostosis of the fourth finger has never been reported before, it presenting as a swan neck deformity is rare.
CASE REPORT
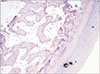
We report a 50-year-old female patient who is a farmer by occupation noticed a gradually progressive swelling over the dorsum of her ring finger of her right hand since one year. She came to us with complaints of mass, deformity and restriction of movements of her finger since three months. On examination, there was a hard, non-tender and immobile. mass palpable over the dorsum of the proximal phalanx of the fourth finger of the right hand. The terminal flexion and extension of the proximal interphalangeal joint were restricted. Due to the restriction of movements of the proximal interphalangeal joint, she developed a swan neck deformity (Fig. 1). Radiographs revealed a bony outgrowth from the dorsum of the proximal phalanx (Fig. 2). Clinical examination and radiographic studies confirmed a dorsal bony outgrowth from the middle phalanx of the fourth finger suggestive of the diagnosis of turrets exostosis. A dorsal fish-mouth incision was made, a sessile bony mass was demarcated over the proximal phalanx of the fourth finger (Fig. 3). The mass was excised and sent for histopathological studies which confirmed the diagnosis. Microscopic studies revealed a tumour composed of mature hyaline cartilaginous cap with underlying lamellar bone displaying mature bony trabeculae with intertrabecular spaces containing yellow marrow components and congested sinusoids confirming the diagnosis of osteochondroma (Fig. 4). The patient was followed-up for one year with no radiological or clinical evidence of recurrence (Fig. 5, 6, 7).
DISCUSSION
Trauma usually precedes turrets exostosis of the hand to the finger1. The mechanism of injury is a sharp injury or repetitive minor injuries which breach the periosteum. This leads to subperiosteal hematoma which ossifies leading to the subperiosteal new bone formation. This new bone formation may go unnoticed due to the overlying soft tissue156. As the lesion increases in size, the symptoms of pain and the appearance of a mass lead the patient to seek medical care. When these lesions affect the dorsum of the phalanges, the extensor mechanism gets damaged leading to loss of extension of the affected finger. In our review of the literature, we found that the phalanges of the index finger and the fifth finger are the most commonly involved. Turrets exostosis of the phalanges of the ring finger (fourth finger) has never been described before156.
The possible differential diagnosis of these lesions includes osteochondroma, proliferation periostitis, malignant lesions like osteosarcoma and osteochondrosarcoma56.
The radiological features of this lesion is a narrow body arising from the bone with a clear delineation from surrounding soft tissue with a smooth dome with a cartilaginous cap8. Histological microscopy also shows evidence of fibrocartilage or hyaline cartilage cap as seen in subungual exostosis and osteochondroma respectively8.
Wissinger et al.1 described the importance of the timing of surgery to ensure a successful outcome. He described that excision should not be done until a minimum period of 4–6 months after initial injury. He reported that the lesion must sufficiently mature and delineate from the surrounding tissues before the decision to operate is made. He explained that the plane of the lesion would be clearly demarcated between the overlying periosteum and the underlying cortex at maturity. This would be the ideal time to take the decision to operate6.
Kang et al.9 reported in his study that a bone scan is a useful tool in determining the time of surgery. He explained that if bone scan uptake reduces by 50% around six months after the initial trauma, it would be an ideal time to perform the surgical excision of the mass. He also explained that there was no clear protocol established yet. In our patient, the bone scan couldn't be performed due to financial constraints. An magnetic resonance imaging scan might be useful in clearly demarcating the plane of the tumour and the underlying periosteum9.
The common complications of turrets exostosis are rupture of the extensor mechanism due to the stretching by the tumour, mechanical block of movements of the adjacent joints of the finger, deformities like fixed flexion deformity or swan neck deformity and lastly recurrence of the tumour9. Our patient presented to us with swan neck deformity and mechanical restriction of movements due to the mass. Recurrence of these lesions is most commonly due to surgical excision of a premature lesion and poor surgical technique19.
An unusual aspect of this case is that the patient gives no definite history of trauma to her finger. However, the authors hypothesise that there could be repetitive minor trauma to the dorsum of her finger due to the nature of her occupation. The turret exostosis of the fourth finger has never been reported in our review of the literature. Our patient surprisingly had a dormant period of one year after which there was a sudden spurt in growth for three months. The patient was followed up for one year after surgery, with no evidence of recurrence of the lesion. The patient had restored the complete range of movement of her finger four weeks after surgery.
In conclusion turret exostosis of the phalanx is rare. This lesion has never been reported to involve the fourth finger of the hand. The timing of the surgery is crucial. The most common complaint is the loss of finger movements due to disruption of the extensor mechanism. Recurrence is a common complication and can be minimized by timing the surgery after the lesion has completely matured.






 XML Download
XML Download