

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The number of elderly people is increasing and the proportion of the elderly population in the US is projected to reach 25% of the population by 2050.1 The prevalence of asthma in the elderly is rapidly increasing worldwide from 3.6% to 17% and was reported at 7.1% in the Korean population.234 However, elderly asthmatics are underdiagnosed, suffer high morbidity and mortality with lower quality of life, which bring economic burden on healthcare systems due to increasing medical service expenses.56
Elderly asthma (EA) is considered to have different pathophysiologic mechanisms, depending on age-related changes in lung function and immune response, epigenetic factors, environmental modification, and various comorbidities; however, most of the previous studies have excluded elderly subjects.17 Aging is a strong factor that contributes to structural and physiological alterations in the airway, loss of lung function, senescence process of immune cells (immunosenescence) and modification of inflammatory response,18 which affects both innate and adaptive immunity.9 Previous studies demonstrated that elderly asthmatics showed lower atopy rate with poor control status.110 In an in vivo model, ovalbumin (OVA)-sensitized aged mice showed a lower level of serum total immunoglobulin E (IgE), less total cellularity with a lower eosinophil counts in bronchoalveolar lavage fluid (BALF), while BALF neutrophil counts were similar between the aged and young mice.8 These findings suggest that inflammatory mechanisms invovled in EA are different from those of non-elderly asthma (NEA), although airway inflammation in asthmatic airways is mainly consists of type-2 inflammation.8 Airway epithelial cells are the first line barrier that responds to external factors and produces various inflammatory mediators, which modulate innate and adaptive immune responses. Cytokines expressed in epithelial cells including interleukin (IL)-33 and IL-31 are known to regulate immune response in asthmatic airway. It is reported that IL-33/IL-31 axis is associated with type 2 inflammation cascades in asthma and allergic disease.1112 In addition, other epithelial cell-derived cytokines such as periostin, transforming growth factor beta-1 (TGF-β1) and eotaxin-2 are known to lead airway inflammation and remodeling.1314 However, the role of these cytokines in EA has not been demonstrated yet.
In the present study, we hypothesized that age-related changes in epithelial cells may affect immune responses of asthmatic airways that modify clinical phenotypes of EA. Serum levels of epithelial-derived cytokines were analyzed in association with clinical characteristics of EA in a cross-sectional cohort of adult asthmatics (with a retrospective design).
MATERIALS AND METHODS
Study subjects
We enrolled 692 normal controls (NCs) and a total of 1,452 asthmatic patients who had been treated in the Department of Allergy and Clinical Immunology, Ajou University Hospital (Suwon, Korea) for more than 2 years with standardized maintenance medications following the Global Initiative for Asthma (GINA) guideline.15 Of the total patients, 234 were classified as EA patients who were diagnosed and enrolled at age ≥ 60 years and the remaining were NEA patients (< 60 years). Previous studies have used different age limits defining EA patients as 55, 60 and 65 years; however, we chose the age cutoff at 60 years in this study. One hundred sixty-three (62.5%) patients were female. Their clinical characteristics were obtained from electronic medical records of each patient including age, sex, disease duration, smoking history, atopic status, asthma severity, sputum eosinophil and neutrophil count, total IgE level, asthma medication and exacerbation histories. Written informed consent forms were collected from the study subject. This study was approved by Ajou University Institutional Review Board (AJIRB-GEN-SMP-13-108).
Collection of clinical data
We analyzed age, sex, asthma duration, onset time, smoking status, atopy, asthma severity, blood eosinophil count, sputum eosinophil and neutrophil count, serum eosinophilic cationic protein (ECP), forced expiratory volume in 1 second (FEV1), and provocative concentration that caused a decrease in FEV1 (% predicted) of 20% on methacholine challenge test (methacholine PC20). Severe asthma was defined when patients are in uncontrolled asthma despite of maintaining combination inhalers composing medium/high-dose inhaled corticosteroids (ICS)/long-acting beta 2 agonist with ≥ 2 times of asthma exacerbations requiring systemic steroid (≥ 45 mg for 3 days) following the European Respiratory Society/American Thoracic Society (ERS/ATS) guideline.16 Atopy was defined as a positive result to at least 1 or more allergens on skin prick test with common inhalant allergens including tree mixture, grass mixture, mugwort, ragweed, cat fur, dog fur, Dermatophagoides pteronyssinus, Dermatophagoides farinae, and Alternaria spp. (Bencard, Bretford, UK). Total IgE and ECP levels were measured by the UniCAP system (ThermoFisher Scientific, Waltham, MA, USA). The serum levels of IL-8 (Endogen Inc., Woburn, MA, USA), eotaxin-2 (RayBio Inc., Norcross, GA, USA), TGF-β1 (R&D Systems, San Diego, CA, USA) and periostin (Shino test, Kanagawa, Japan),17 IL-33 and IL-31 (R&D Systems) were measured by enzyme-linked immunosorbent assay (ELISA). Serum samples were collected and frozen at −70°C and thawed before use. The spontaneous sputum samples were collected from the patients, and the total number of cell viability was determined with Trypan blue stain. The slides were prepared for cytological examination with Wright-Giemsa stain, and differential counts were determined by counting 100 leukocytes on each sputum slide. Sputum eosinophil/neutrophil counts were calculated as % of eosinophil or neutrophil number per 100 leukocytes counted.
Statistical analysis
Statistical analysis was performed using SPSS statistical software 20 (SPSS Inc, Chicago, CA, USA). Student's t-test was used to compare clinical parameters; Mann-Whitney U test was applied to compare serum cytokine levels. Pearson χ2 test was used to compare the prevalence rate of clinical parameters. Spearman rank correlation analysis was used to determine an association between the continuous parameters. Predictive values of serum eotaxin-2 and TGF-β1 levels were determined by receiver operating characteristic (ROC) analysis. P values < 0.05 were considered statistically significant. ROC analysis was performed to differentiate the severe phenotype from the non-severe phenotype among EA patients.
RESULTS
Comparison of clinical characteristics
The clinical characteristics of the study subjects are summarized in Table 1. Significantly higher prevalence rates of late-onset asthma (LOA, onset age ≥ 40 years old) and severe asthma were noted in EA patients than in NEA patients (Table 1). Asthma duration tended to be longer in EA patients than in NEA patients, although statistical significance was not reached (Table 1). Atopy rate, peripheral blood/sputum eosinophil counts, and serum ECP level were significantly lower in EA patients than in NEA patients, while sputum neutrophil count was significantly higher in EA patients (Table 1). When serum total IgE levels were log-transformed to correct the skewed distribution, it was significantly lower in EA than in NEA patients (Table 1). The baseline level of FEV1 (% predicted) was lower in EA patients than in NEA patients, although statistical significance was not reached (Table 1).
Table 1
Comparison of clinical characteristics between EA (age ≥ 60) and NEA (age < 60) patients
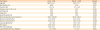
Values are given as number (%) for categorical variables and as mean ± SD for continuous variables. P values were applied by the Pearson χ2 test for categorical variables and Student's t-test for continuous variables.
EA, elderly asthma; NEA, non-elderly asthma; ECP, eosinophil cationic protein; FEV1, forced expiratory volume in 1 second; Ig, immunoglobulin; methacholine PC20, concentration of methacholine to induce a 20% decline in FEV1%; SD, standard deviation.
*Log-transformed data were shown.
![]()
Immunologic features
The serum levels of eotaxin-2 (1,234.7 ± 877.2 vs. 942.5 ± 594.1 pg/mL, P < 0.001), TGF-β1 (30.2 ± 15.3 vs. 25.5 ± 11.2 ng/mL, P = 0.001), and periostin (80.6 ± 39.4 vs. 57.3 ± 29.6 ng/mL, P < 0.001) were significantly higher in asthmatic patients than NCs, while no differences were found in terms of IL-8 (60.9 ± 32.7 vs. 32.7 ± 66.8 pg/mL, P = 0.420), IL-33 (72.2 ± 209.5 vs. 73.1 ± 185.1 pg/mL, P = 0.705) or IL-31 (734.5 ± 2,933.6 vs. 843.3 ± 1,686.6 pg/mL, P = 0.120) levels. When they were compared between EA and NEA patients, significantly lower levels of serum IL-31 and IL-33 were found in EA patients than in NEA patients (Table 2, Fig. 1), while no difference were found in serum IL-8, eotaxin-2, TGF-β1 and periostin levels were not significantly different between 2 groups (Table 2).
Table 2
Comparison of serum cytokine and chemokine levels between EA patients, NEA patients, ENCs and NENCs

Values are given as mean ± SD for continuous variables. P values were applied by Mann-Whitney U test.
EA, elderly asthma; NEA, non-elderly asthma; ENC, elderly normal control; NENC, non-elderly normal control; IL, interleukin; TGF-β1, transforming growth factor beta 1; SD, standard deviation.
![]()
 | Fig. 1Comparison of serum levels of IL-33 and IL-31 between EA and NEA patients. Serum cytokine levels were measured by ELISA. Each mean value is represented and P values were analyzed by the Mann-Whitney U test. P < 0.05 was considered significantly different.IL, interleukin; EA, elderly asthma; NEA, non-elderly asthma; ELISA, enzyme-linked immunosorbent assay.
|
Association of clinical parameters and cytokine levels according to the severity in EA
EA patients were classified into severe and non-severe eosinophilic asthma (SEA and NSEA). Although there were no significant differences in clinical variables including disease duration, atopy profile, or blood/sputum eosinophils between 2 groups, SEA patients had a significantly lower FEV1 (% predicted) level with a higher prevalence of smoking rate than NSEA patients (Table 3). Significant higher serum levels of eotaxin-2 and TGF-β1 were noted in SEA patients than in NSEA patients (Table 4, Fig. 2). When the cutoff value of serum eotaxin-2 level discriminating SEA from NSEA was determined at 1,181.6 pg/mL, the ROC curve analysis showed 66.7% sensitivity and 60.3% specificity (area under the curve [AUC] = 0.700; 95% confidence interval [CI], 0.575–0.826; P = 0.004, Supplementary Fig. S1). As for the serum TGF-β1 level, the cutoff value that discriminating SEA from NSEA patients was determined at 32.5 ng/mL with 68.2% sensitivity and 66.7% specificity (AUC = 0.664; 95% CI, 0.526–0.801; P = 0.026). There was a positive correlation between the serum eotaxin-2 and TGF-β1 levels in EA patients (r = 0.401; P < 0.001, Supplementary Fig. S2).
Table 3
Comparison of clinical and immunologic findings between SEA and NSEA patients
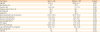
Values are given as number (%) for categorical variables and as mean ± SD for continuous variables. P values were applied by the Pearson χ2 test for categorical variables and Student's t-test for continuous variables.
SEA, severe elderly asthma; NSEA, non-severe elderly asthma; Ig, immunoglobulin; ECP, eosinophil cationic protein; FEV1, forced expiratory volume in 1 second; methacholine PC20, concentration of methacholine to induce a 20% decline in FEV1; SD, standard deviation; CRS, chronic rhinosinusitis.
*Log-transformed data were shown.
![]()
Table 4
Comparison of serum cytokine and chemokine levels between SEA and NSEA patients

Values are given as mean ± SD for continuous variables. P values were applied by Mann-Whitney U test.
SEA, severe elderly asthma; NSEA, non-severe elderly asthma; IL, interleukin; TGF-β1, transforming growth factor beta 1; SD, standard deviation.
![]()
 | Fig. 2Comparison of serum levels of eotaxin-2 and TGF-β1 according to severity in elderly asthma patients. Severe asthma was defined according to International ERS/ATS guideline. Serum cytokine levels were measured by ELISA. Each mean value is represented and P values were analyzed by the Mann-Whitney U test. P < 0.05 was considered significantly different.TGF-β1, transforming growth factor beta 1; ERS/ATS, European Respiratory Society/American Thoracic Society; ELISA, enzyme-linked immunosorbent assay; SEA, severe elderly asthma; NSEA, non-severe elderly asthma.
|
DISCUSSION
In the present study, we characterized the clinical phenotypes of EA and compared serum epithelial-derived cytokines between EA and NEA. EA has been found to present more severe phenotypes (higher prevalence of severe asthma and lower FEV1 [% predicted]) with less type 2 inflammation, but had lower levels of serum IL-33/IL-31 than NEA. Moreover, SEA patients had higher serum levels of eotaxin-2 and TGF-β1 than NSEA. Based on these findings, we suggest that changes of epithelial cell-derived cytokines (serum IL-33, IL-31, eotaxin-2 and TGF-β1) may contribute to present less type 2, but severe phenotypes of EA.
Asthma is characterized by airway inflammation associated with reversible airflow obstruction and airway hyperresponsiveness, which can be exacerbated by allergic and non-allergic triggers including respiratory viral infections.15 Distinct clinical phenotypes of EA are characterized by LOA, fixed airway obstruction and high prevalence of comorbid diseases, which are referred as to intrinsic asthma (lower atopy rate).1819 LOA has been recognized as an asthma phenotype representing greater airway obstruction and more frequent exacerbations followed by lung function decline.1920 Non-Th2 type of LOA in association with aging was reported.21 In addition, respiratory viral infections, the most common asthma exacerbation factors could precipitate LOA, which immunosenescence in elderly patients could enhance virus-induced airway inflammation and asthma exacerbations.212223 It is known that symptoms in EA are more difficult to control and less respond to conventional anti-inflammatory agent such as ICS, and that EA is a less eosinophilic type242526 and can be exacerbated by various comorbid conditions.31027 Moreover, less type 2 inflammation may shift to Th1/Th17 inflammation in EA: allergen-challenged older mice had greater mucous cell metaplasia with higher expression of interferon-γ than younger mice, showing a high bias towards a Th1 response.28 Sputum neutrophil counts were higher in EA patients29; ICS resistant type 2-low asthmatic patients showed increased expression of IL-17, which contribute to develop severe asthma with increased mucus secretion and greater airway obstruction.30 In the present study, the most EA patients had LOA, and had lower atopy rate, lower sputum eosinophilia but higher neutrophilia; they have higher prevalence of severe asthma and lower lung function. In addition, diagnosis of EA is challenging due to cognitive impairment, stagnancy, limitation in performing basic pulmonary tests and comorbidities.1 These findings suggest that EA patients present less type 2, but severe phenotype (due to the aging process and comorbid conditions); therefore, early diagnosis and careful monitoring are essential to achieve control status and to prevent lung function decline.
Airway epithelial cells are the first barrier in the airway which initiates innate/adaptive immune responses. Aging decreases airway ciliary clearance and induces disarrangement of airway cell microtubules.3132 IL-33 (mainly expressed in epithelial cells) and its receptor ST2 have been found to be a key cytokine to derive type 2-mediated eosinophilic inflammation.3334 IL-31 (extensively expressed in activated Th2 cells and partly in monocytes, dendritic cells, basophils and mast cells) and its receptor expressed on immune cells including bronchial epithelial cells play a role in Th2-mediated airway inflammation in the asthmatic airway; IL-31/its receptor levels expressed in bronchial tissue were positively correlated with disease severity or other Th2 cytokine expression in asthmatic airway.353637 Moreover, a close link (synergic responses) between IL-33 and IL-31 was suggested in allergic airway inflammation.1138 In the present study, EA patients had significantly lower levels of IL-33 and IL-31 with lower atopy rate and less eosinophilia compared to NEA patients, suggesting that age-related changes of epithelial cells may reduce expression of IL-33 in the airway of EA, thereby reducing IL-31 expression, which may contribute to develop less atopic/less type 2 phenotype in EA.
There have been several studies suggesting that increased levels eotaxin-2 and TGF-β1 are associated with asthma severity and control status.1439 Eotaxin-2 mainly released from airway epithelial cells is a chemoattractant factor for eosinophils.4041 TGF-β1, which is also released from airway epithelial cells, plays a critical role in epithelial cell apoptosis, subepithelial fibrosis and mucus hypersecretion in the process of airway inflammation/remodeling.394142 In the present study, serum levels of eotaxin-2 and TGF-β1 were significantly higher in SEA than in NSEA patients with a significant correlation was between these 2 cytokines (no significant correlation with serum periostin or total eosinophil count). These findings suggest that eotaxin-2 released from airway epithelial cells plays a key role to attract eosinophils, and that TGF-β1 could lead to fixed airway obstruction and lung function decline in the asthmatic airway of severe EA. We also found no significant difference in serum periostin level between SEA and NSEA. Since serum periostin has been known as a serum biomarker for representing the phenotype of severe asthma in adult asthma cohorts,434445 this conflicting finding may be derived from that serum periostin is a biomarker of type-2 inflammation; EA has less-atopic phenotype. Smoking has been suggested to be a significant risk factor for severe asthma in a Korean adult asthmatic cohort.46 Elderly asthmatics who are smokers are at higher risk of progression into asthma-chronic obstructive pulmonary disease overlap syndrome.4748 In the present study, the prevalence of smoking history (current/ex-smokers) was significantly higher in SEA patients than in NSEA patients, suggesting that smoking is a risk factor for severe asthma in EA patients.
This study has some limitations. First, the number of elderly asthmatics, especially that of severe asthmatics, is relatively small. Secondly, this is a retrospective study based on electronic medical record and we could not monitor Asthma Control Test (ACT) scores of each patients with anti-asthmatic medications when enrolled. Thirdly, we measured cytokine levels only in serum, not sputum sample or BALF samples. Finally, we could not confirm the function of cytokines studied using in vitro and in vivo models. Further studies are needed to elucidate mechanisms by which epithelial cell function and cytokines are modified and alter airway inflammation with age in EA.
In conclusion, age-related changes of epithelial cell-derived cytokines may affect clinical phenotypes and severity of EA.
 XML Download
XML Download