

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The increasing prevalence of allergic disorders worldwide imposes a significant socioeconomic burden on society. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase IIIwhich surveyed around 1.2 million children across 233 centers in 98 countries found the prevalence of atopic dermatitis (AD) to be 7.9%, asthma 11.7%, and rhinoconjunctivitis 8.5% in 6- to 7-year old children, and 7.3% (AD), 14.1% (asthma) and 7.3% (rhinoconjunctivitis) in 13- to 14-year olds.1 Food allergy affects up to 8% of children and its prevalence has been increasing over the past 2 decades.2
The term “atopic march” was coined to describe the progression from AD in early infancy to other allergic diseases such as food allergy, asthma and allergic rhinitis in later childhood (Fig. 1).34 AD is a chronic inflammatory skin disorder which is marked by skin barrier dysfunction, frequent skin infections and impaired quality of life. In many children, AD is the first manifestation of an atopic phenotype which begins in early infancy. A recent study suggested that the complete manifestations of the atopic march occurred in less than 10% of AD patients5 ; however, approximately 40% of AD patients have food allergy. Severity of AD is a factor determining subsequent development of allergic disease.
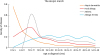 | Fig. 1The atopic march. The figure shows the age at diagnosis of each allergic disease. Reproduced with permission from Ann Allergy Asthma Immunol 2018;120:131-7.4
|
Several prospective birth cohorts have shown associations between early-onset AD and development of asthma and allergic rhinitis in school age.67 The risks appear to be even greater in children with the early-onset persistent AD phenotype.8 The Canadian Healthy Infant Longitudinal Development Study found that children with AD and allergic sensitization had a greatly increased risk of food allergy, asthma and allergic rhinitis compared to non-sensitized children without AD.9
The combined study by the high-risk Melbourne Atopy Cohort Study (MACS) and the population-based Influences of Lifestyle-Related Factors on the Immune System and the Development of Allergies in Childhood plus Air Pollution and Genetics (LISAplus) cohort found that food sensitization in the first 2 years of life was associated with increased risks of asthma and allergic rhinitis by age 10 years.10 A meta-analysis of 13 cohorts studying the atopic march also demonstrated that early food sensitization was associated with increased risks of wheeze/asthma and allergic rhinitis at 4 to 8 years of age.11 Hill et al.12 likewise observed that children with food allergy, particularly peanut, milk and egg allergy, were at increased risk of developing asthma and rhinitis in later childhood.
This review explores the evidence supporting the concept that impaired epithelial barrier in AD initiates progression to epicutaneous sensitization, food allergy and allergic airway disease in later life as well as intervention strategies aimed at preventing progression through the atopic march.
GENETIC PREDISPOSITION TO SKIN BARRIER DYSFUNCTION AND AD
The dual-allergen exposure hypothesis postulates that exposure to environmental food allergens induces sensitization and ensuing food allergy through an impaired skin barrier as in AD. Immune tolerance can, however, be achieved through early oral exposure to food allergens.13
Intact healthy skin serves as an important physical and immunological barrier against the entry of environmental allergens and microbes into the body. The epidermis is comprised of terminally differentiated keratinocytes, which form a cornified layer of keratin filaments aggregated by filaggrin (FLG), involucrin and loricrin. Epidermal lipids, such as ceramides, are produced by keratinocytes and surround the keratin filaments, forming an impermeable skin barrier.14 Skin barrier defects may arise from multiple factors, including defects in terminal epithelial differentiation such as lack of FLG, deficiency of antimicrobial peptides (AMPs), altered stratum corneum intercellular lipids, skin microbiome dysbiosis and immune dysregulation.15
Genetic defects encoding skin barrier proteins and abnormalities in lipid production or tight junctions contribute to epithelial barrier dysfunction that characterizes AD. The FLG gene encodes filaggrin, an essential epidermal protein expressed in the outer layers of the epidermis, playing an important role in maintaining skin barrier integrity. FLG loss-of-function mutations are associated with an earlier onset as well as a more persistent phenotype of AD.16 Polymorphisms in the thymic stromal lymphopoietin (TSLP) gene and its receptor as well as dysregulation of genes involved in epidermal lipid metabolism have likewise been reported to be associated with increased risks of AD and its persistence.171819 Other skin barrier mutations involving the SPINK5 gene20 and corneodesmosin21 as well as genome-wide association study (GWAS)-identified genetic variants22 have also been linked to AD and the development of food allergy.
Kelleher et al.23 found that neonates with increased transepidermal water loss (TEWL) in the first week of life had an increased risk of developing AD at 12 months of age. The strong genetic basis for AD described above supports the view that skin barrier impairment may be evident very early in life, even before the onset of clinical AD.
SKIN BARRIER DYSFUNCTION PREDISPOSES TO EPICUTANEOUS SENSITIZATION AND FOOD ALLERGY
There is now a growing body of evidence supporting the notion that epicutaneous allergen sensitization occurs more readily through an impaired skin barrier.1524 Murine models demonstrated that the application of ovalbumin (OVA) or peanut allergens on abraded mice skin resulted in significant systemic egg and peanut-specific immunoglobulin (Ig) E responses.2526 In a mouse model of FLG deficiency, flaky tailed mice with a 1-bp deletion mutation (5303delA) within the murine FLG gene were treated with topical applications of OVA. These mice displayed increased cutaneous inflammatory infiltrates and enhanced cutaneous allergen priming with raised specific IgE to OVA compared to wild-type mice, even without prior abrasion of the skin. This suggests that FLG mutation-induced skin barrier dysfunction allowed for cutaneous penetration of allergens and the development of systemic allergic responses.27
Several murine models have also described the immunological pathways involved in the progression from epicutaneous sensitization to food allergy. Mice which were epicutaneously sensitized with topical applications of OVA on tape-stripped skin (to mimick scratching) exhibited IgE-dependent intestinal mast cell expansion, increased serum interleukin (IL)-4 levels and systemic anaphylaxis following oral OVA challenge.28 In another study, mice epicutaneously sensitized with OVA or peanut on an AD-like skin lesion demonstrated TSLP-dependent basophil expansion in the skin, which promoted antigen-specific Th2 cytokine responses, increased antigen-specific serum IgE levels and accumulation of mast cells in the intestine akin to IgE-mediated food allergy.29 Conversely, disruption of the TSLP-basophil axis abrogated this allergic response. A follow-up study showed infiltration of IL-4-competent basophils and eosinophils into the skin of these epicutaneously OVA-sensitized mice, indicating that TSLP-dependent basophils mediate Th2-allergic sensitization to food antigens through the production of IL-4 and that these mechanisms likely play a key role in the pathogenesis of epicutaneously induced intestinal food allergy.30
The role of IL-33 in mediating oral anaphylaxis through epicutaneous sensitization is now also emerging. In another murine model of epicutaneous OVA-sensitization, Galand et al.31 showed that mechanical skin damage induced by tape stripping induced local and systemic IL-33 release, which then enhanced IgE-mediated mast cell degranulation and induced anaphylaxis after oral antigen challenge. Disruption of IL-33 signalling through blockade of ST2 (the IL-33 receptor) resulted in the inhibition of oral anaphylaxis.
Findings from clinical studies also support the concept of the atopic march from early skin barrier dysfunction to the development of food sensitization and clinical food allergy. Increased TEWL at 2 days of life was found to be predictive of food allergy development at 2 years of age.32 A birth cohort study found that children with chronic low-dose topical exposure to peanut allergens, in the form of arachis oil, on inflamed skin had an increased risk of peanut allergy at age 5 years.33 Another study found that 32% of children with AD who used oat-based creams had positive patch tests to oat compared to 0% in those who did not.34 The MACS study found that children with AD at age 6 months had increased risks of developing new-onset food and inhalant sensitization by 1 and 2 years of age, respectively.35 In the HealthNuts cohort, infants with AD in the first year of life had an 11-fold risk of developing peanut allergy and 6-fold risk of egg allergy by age 12 months.36 Up to 50% of the infants who had moderate to severe AD in the first 3 months of age requiring topical corticosteroid use subsequently developed challenge-proven food allergy.
Skin microbiome dysbiosis also contributes to skin barrier dysfunction and modulates epicutaneous allergen sensitization. Up to 90% of AD patients are colonized with Staphylococcus aureus. Disease severity and exacerbations are linked to increased S. aureus abundance and reduced local bacterial diversity, which are evident even at non-lesional sites.37 S. aureus perpetuates the pathogenesis of AD through various mechanisms, including disruption of epidermal integrity through protease activity, down-regulation of terminal differentiation markers in the skin and production of virulence factors such as cytolysins, protein A and superantigens.38 Staphylococcal-derived superantigens, such as staphylococcal enterotoxin B (SEB), have been shown to enhance Th2 inflammation in the skin in response to peanut allergens and drive the development of peanut allergy.39 Jones et al.40 also observed that colonization with S. aureus, particularly methicillin-resistant S. aureus (MRSA) was associated with a higher risk of food allergy.
THE MARCH FROM AD TO ALLERGIC RHINITIS AND ASTHMA
The link between AD and allergic airway diseases is influenced by the age of AD onset and its severity. High-risk infants in the MACS study with early-onset persistent AD had a 3-fold risk of developing asthma and allergic rhinitis in later childhood, compared to children with late-onset AD that began after 2 years of age.41 In another Swedish cohort, more than 60% of children with severe AD before 3 years of age developed asthma by age 7, compared to only 20% of those with mild AD.42 The presence of AD was also associated with increased asthma severity as well as greater persistence into adulthood.4344
Inherent genetic susceptibility may also influence one's risk of progression from AD to allergic airway disease. A GWAS study identified shared asthma, hay fever and AD immune-related gene variants, suggesting that these allergic disorders may co-exist because they share genetic risk loci that result in dysregulation of immune-related genes.45 Another AD GWAS study also found genetic loci that overlapped between asthma and AD.46 A multi-stage GWAS study on children with infantile AD and childhood asthma identified novel genetic loci (rs9357733 located in EFHC1 on chromosome 6p12.3 and rs993226 between TMTC2 and SLC6A15 on chromosome 12q21.3) which were specific for the AD-to-asthma atopic march phenotype.47 A Kinesin family member 3A (KIF3A) genetic variant was also found to be associated with AD-asthma comorbidity in a population cohort from the Greater Cincinnati Pediatric Clinic Repository (GCPCR).48
The mechanisms behind the march from AD to allergic airway disease likely arise from initial epicutaneous allergen sensitization inducing robust local and systemic Type 2 immune responses, supporting the view that AD is not merely a disease confined to the skin, but is in fact a systemic disease. Epicutaneous exposure to the Aspergillus fumigatus aeroallergen has been reported to induce nasal hyperresponsiveness to methacholine and inflammation upon subsequent intranasal A. fumigatus challenge in mice through a STAT6-dependent pathway.49 Epicutaneous OVA application to tape-stripped mouse skin, followed by a bronchial OVA challenge, also induced bronchial eosinophilia and airway hyperresponsiveness to methacholine, akin to allergic asthma.26
The inflammatory responses induced by AD are manifested by increased production of Type 2 cytokines such as IL-4, IL-13, IL-25 and IL-33 as well as TSLP. The latter now appears to be a major player in inducing systemic Type 2-immune responses, which are responsible for the pathogenesis of allergic airway diseases. TSLP is an IL-7 related cytokine that is expressed predominantly in skin keratinocytes, pulmonary airways and intestinal epithelium. Increased TSLP expression has been observed in both the skin of AD subjects and asthmatic pulmonary epithelia.50 Intradermal administration of TSLP together with OVA, in mice, leads to an AD-like skin inflammation with epicutaneous OVA sensitization, and results in an allergic asthma-like phenotype upon airway OVA challenge.51 Another murine model demonstrated that overproduction of TSLP by AD skin promoted airway sensitization to house dust mite (HDM) aeroallergens and induced allergic airway responses in sensitized mice.52
EPICUTANEOUS SENSITIZATION WITHOUT AN IMPAIRED SKIN BARRIER
Interestingly, epicutaneous sensitization has been found to cause clinical food allergy or airway allergic disease even without a disrupted skin barrier. These events occur in the presence of an adjuvant or following highly concentrated chronic exposure. Dunkin et al.53 found that mice sensitized to the milk allergen, α-lactalbumin (ALA), through the cutaneous route by direct skin application of ALA and cholera toxin, used as an adjuvant, developed systemic anaphylaxis upon oral challenge with ALA. An outbreak of new-onset IgE-mediated wheat protein allergy was also reported in previously healthy Japanese adults after chronic usage of a wheat-containing facial soap on intact facial skin.54 HDM allergens applied epicutaneously to unmanipulated mouse ears or under an occlusive tape induced Th2 sensitization and eosinophilic airway inflammation upon intranasal HDM challenge.55 In another study, mice cutaneously sensitized to HDM allergen Der p 2 through intact skin developed significant systemic allergen-specific IgE and IgG1 antibody responses.56 These responses were augmented by the addition of lipopolysaccharide (LPS), suggesting that it could act as an adjuvant inducing aeroallergen sensitization through the skin.
Likewise, Walker et al.57 demonstrated that when neonatal mice heterozygous for skin barrier mutations were cutaneously sensitized to food allergens in the presence of fungal (Alternaria alternata) or HDM extracts, they developed food allergen sensitization, food-induced anaphylaxis and increased skin and intestinal inflammation upon oral food allergen challenge. These events were not observed when mice were sensitized with food allergen alone. In these mice, pre-exposure with oral peanut extract before skin sensitization was able to induce oral peanut tolerance. However, co-exposure to A. alternata at the same time as the oral peanut extract reduced the induction of oral tolerance. This suggested that co-exposure to environmental allergens, which alter the skin barrier, may facilitate food allergen sensitization and the development of food allergies early in life in infants with skin barrier mutations.
PREVENTIVE MEASURES AGAINST THE ATOPIC MARCH
The increasing body of knowledge surrounding risk factors for the atopic march has triggered renewed interest in the study of preventive interventions aimed at halting progression through the atopic march. Many of the primary prevention measures have been targeted at reducing the risk of AD development through prophylactic skin barrier protection beginning very early in life in high-risk neonates (Fig. 2). Horimukai et al.58 and Simpson et al.59 both demonstrated that regular application of standard emollients from birth reduced the incidence of AD at 8 and 6 months of age, respectively. The latter study also reported that children in the emollient group had a lower skin pH and altered skin microbiome, with increased proportions of Streptococcus salivarius organisms at various skin sites, compared to the control group, suggesting that these mechanisms may contribute to the preventative effects of emollients in these high-risk infants.60 The Prevention of AD By a Barrier Lipid Equilibrium Strategy (PEBBLES) study, which utilized topical applications of a trilipid-rich ceramide-dominant emollient in high-risk infants from birth to 6 months, showed decreased food sensitization at age 6 and 12 months when emollient therapy was introduced during the first 3 weeks of life.61 Several larger trials are also currently ongoing which aim to assess the efficacy of regular moisturizing for skin barrier protection in early life against the development of not just AD, but also challenge-proven food allergy and allergic airway diseases.6263
 | Fig. 2Emollient therapy for AD prevention. Early skin barrier protection with prophylactic emollient therapy might prevent AD development. Original source: J Allergy Clin Immunol 2014;134:818-23, an open access article under the CC BY license (http://creativecommons.org/licenses/by/3.0/).59AD, atopic dermatitis; FLG, filaggrin; TSLP, thymic stromal lymphopoietin.
|
There is some evidence that probiotic supplementation in pregnancy or infancy may be protective against the development of AD, but no protection against food allergy or other allergic disorders have been proved.64 There is still insufficient evidence for the use of other nutritive interventions such as prebiotics, hydrolyzed formulas or vitamin D supplementation in the primary prevention of allergic diseases.
Secondary prevention of allergic disease involves interventions targeted at high-risk infants or children with known disease such as pre-existing AD, or food sensitization without clinical food allergy, aiming to prevent progression to the next phase of the atopic march. The Japanese Prevention of Allergy via Cutaneous Intervention (PACI) study is one such ongoing randomized controlled trial that plans to measure the effects of aggressive (proactive) treatment of 7- to 13-week old infants with AD versus standard (reactive) AD treatment for the prevention of challenge-proven IgE-mediated hen's egg allergy at 28 weeks of age.65
Several randomized controlled trials have now shown that early introduction of allergenic foods such as peanut or egg to high-risk infants with severe AD or pre-existing food sensitization may reduce the risk of developing peanut or egg allergies, respectively. High-risk infants aged 4-11 months with severe AD and/or egg allergy and peanut skin prick test (SPT) responses of 1-4 mm were enrolled into the Learning Early About Peanut Allergy (LEAP) trial. Infants randomized to consume 6 grams of peanut protein at least 3 times a week or 2 grams 3 times a week had an 81.4% lower risk of developing challenge-proven peanut allergy by age 5 years, compared to those who completely avoided peanut products.66 The Prevention of Egg allergy with Tiny amount InTake (PETIT) study investigated the effects of early introduction of heated egg powder to high-risk Japanese infants with AD on the development of egg allergy.67 The intervention group which received 50 mg of heated whole egg powder between 6-9 months of age, then 250 mg between 9-12 months of age, had 30% lower risk of developing challenge-proven hen's egg allergy at 12 months of age, compared to the placebo group.
Several primary prevention strategies for asthma and allergic rhinitis have also been investigated. These include HDM avoidance in early life and prophylactic sublingual immunotherapy in sensitized children. None, however, have shown sufficient evidence for adoption into routine clinical practice yet.6869
CONCLUSIONS
There is strong evidence for the link between early-onset AD and the development of other allergic diseases in later life. Several preventive interventions such as early regular emollient use and early introduction of peanut and egg in high-risk infants have shown promising results for the prevention of AD as well as peanut and egg allergy. However, more studies are needed to determine the efficacy of these interventions on prevention of other food allergies and allergic airway disorders. Future research should also focus on identifying biomarkers predictive of risk of progression through the atopic march, in order to develop interventions specific to this high-risk group. There is reason to hope that more options will eventually be available to prevent or halt progression through the atopic march.
 XML Download
XML Download