

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Staphylococcus aureus is a major cause of community acquired skin and soft tissue infections (CA-SSTI), and can lead to serious systemic infections.1) The outbreak of S. aureus infection has been reported to occur within households, and transmission of S. aureus can be occurred by close contact.23) Retention of asymptomatic S. aureus infection in household members can serve as a repository for transmission to other household contacts.4) Clinicians are currently primarily concerned with community acquired methicillin-resistant S. aureus (CA-MRSA) infection acquired primarily by the community, but methicillin-sensitive S. aureus (MSSA) infection shows similar epidemiological and clinical features.5) Furthermore, the presence of the Panton-Valentine leukocidin (PVL) gene is not limited to MRSA and its presence has not only been recently identified.6) Large, multinational clinical trials indicate that PVL-positive S. aureus isolates are more likely to be MSSA than MRSA.7)
We describe a case of recurrent familial furunculosis caused by PVL-positive methicillin susceptible S. aureus ST1 in Korea.
CASE
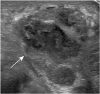
A 16-month-old boy (patient 1) was admitted to the hospital through the outpatient clinic with fever and a palpable mass in the left axilla for 3 days. Multiple furuncles of size 1 cm or less on the waist and legs had been found from 1 month before the hospital visit, but were self-limiting. At the time of visiting hospital, the tender mass in the left axilla was red and about 8 cm in size (Fig. 1). His blood pressure was 90/60 mmHg, pulse rate was 120 beats per minute, respiratory rate was 34 breaths per minute, temperature was 39.9°C, and he had experienced normal growth and development. Ultrasonographic examination of the mass revealed a hypoechoic, septate and complex lesion (Fig. 2, arrow). Ultrasound-guided needle aspiration was performed twice, and cultures of the aspirated fluid all yielded MSSA. The family of the infant comprised the father and mother who got married 3 years ago, the sister and the infant. The father and the mother also had skin infections at the time of their son's visit to the hospital.
Fig. 1
A palpable mass of a 16-month old boy (patient 1). A red tender mass in the left axilla is about 8 cm in size.

Fig. 2
Left axillary mass in a 16-month old boy (patient 1). Transverse sonography shows a heterogeneous hypoechoic mass (arrow) with internal septations.
The 36-year-old father (patient 2) was diagnosed with a left lower leg furuncule. He had stayed in Fiji for 4 years for missions until 2011 when he came back home to Korea. From childhood, he suffered from psoriasis, and there was the occurrence of furunculosis even as a child, but naturally improved without any treatment. After returning home from Fiji 5 years before the hospital visit, he had experienced recurrent skin infections on the buttocks and legs. Unlike before, the skin lesion was larger and there was more pus formed.
The 30-year-old mother (patient 3) was diagnosed with furuncles of the buttocks, the groin and the left leg. She had experienced skin infections in the groin 6 months ago, in the parts of each leg similar to the current presentation, but she said that they improved without treatment. The father and mother had been in their usual state of health before the hospital visit and they had no medical history except for the skin infections.
Surgical incision and drainage were performed for both father and mother (patients 2 and 3) in the dermatologic outpatient clinic; a culture of the aspirated fluid yielded MSSA, like their son. The infant underwent treatment with intravenous cephalosporin for 2 weeks, followed by oral antibiotics, while the parents were treated with oral cephalosporin for a week, at doses based on their body weights. All the patients recovered without any complications. Identification of isolation and antimicrobial susceptibility tests were performed using an automatic system (Vitek 2; bioMérieux, Marcy l'Etoile, France). The susceptibility pattern was confirmed by the disk-diffusion method according to the guidelines of Clinical and Laboratory Standards Institute. All cases with a bacteriologic diagnosis were caused by MSSA, which showed a distinct identical susceptibility pattern: resistance to penicillin G and susceptible to oxacillin, erythromycin, tetracycline, rifampicin, ciprofloxacin, and gentamicin.
Multi-locus sequence typing (MLST) was performed to confirm that the skin infection was caused by the same strain. Selected isolates underwent MLST according to the recommended method.8) The allelic profiles obtained were compared with those deposited in the MLST database (http://saureus.mlst.net). ST1 accounted for all 3 isolates. Polymerase chain reaction (PCR)-based assays were used to assess agr locus nucleotide polymorphism to identify agr specificity group. Three isolates were confirmed as being in agr group I. Staphylococcal enterotoxins (sea, seb, sec, sed, see, seg, she, sei, sej) were identified using PCR assays with primers and conditions previously described.9) Sec and seh were detected in all isolates. Detection of genes encoding the PVL was performed as described and all isolates contained PVL genes.10)
Nasal swab cultures for screening MSSA colonization were performed for the 3 patients and no MSSA strain was identified. In this case, the patients could not visit the hospital on the same day, and they were already on antibiotic treatment when the nasal swabs were obtained; thus, the colonization rate might be underestimated. The 3 patients underwent treatment with mupirocin (twice daily, nasally) for 5 days.
The family members were close contacts sharing towels, bedding and bathroom. Implementation of infection control measures including contact precautions, enhanced hand hygiene and mupirocin treatment were performed. There was no recurrence or new event of skin and soft tissue infections (SSTI) among all these patients during the 7 months follow-up period.
DISCUSSION
We investigated an outbreak of furunculosis caused by a PVL-producing MSSA strain and cross-transmitted through physical contact among family members. In this case, though the father and mother had been experienced skin infections for several years, they resolved without antibiotic treatment. During this outbreak, all three patients were managed by surgical drainage and use of antibiotics. In the case of the infant, the clinical course was worse and the duration of treatment was longer than his parents who had normal immunity. They were in close contact sharing towels, beddings and toilets. By combining S. aureus decontamination and hygiene education strengthening, we successfully interrupted person-to-person transmission and enabled control of the outbreak.
Considering the time of occurrence of recurrent skin infection in the family, the father was concluded to be the index case. Households with previously infected individuals are at high risk for recurrent infection.1112) The risk factor for S. aureus colonization in his father was psoriasis, which he had experienced from childhood, and may cause recurrent SSTIs. It might have been transmitted to the infant's mother after they got married, and could be estimated to have been transmitted to the affected children. The father experienced furuncles sometimes during childhood, but they resolved without any treatment. After staying in the tropical country of Fiji for missionary work, the degree of skin infections was much more severe and aggressive than before.
The outbreak strain was agr type I, PVL positive, MSSA ST1 and positive for sec and seh. PVL is a cytotoxin produced by S. aureus that causes severe tissue necrosis.13) It is produced by fewer than 5% of MSSA strains and could be detected in furunculosis and necrotic hemorrhagic pneumonia.14) Staphylococcal furunculosis can be seriously complicated if the infecting strain harbors genes for the production of PVL.15) Clonal spread of PVL-positive S. aureus within a family and a community were described in various reports.16)
Our case reflects the high risk of relapses and contagiosity of PVL-producing MSSA. Whether these PVLs relate to the father's residency in Fiji for several years is not clear in the present case. The possibility that international travel may result in the acquisition of new S. aureus strains may be considered. Although the exact route of transmission of S. aureus has not been elucidated in this case, there may be the possibility of nasal colonization and transmission by skin contact among the family members.
Previously there were several reports of skin and soft tissue infections associated with PVL-positive MSSA. As an example, during February 2004 to September 2006, familial clusters and sporadic cases of skin and soft tissue infections caused by MSSA strain, spa type 005 and sequence type 22 that harbored PVL genes were observed in northern Italy.17)
There are several limitations to our study. The patients were already on antibiotic treatment when nasal swabs were obtained; thus, the colonization rate might be underestimated. The risk factors of the household spread of S. aureus includes skin conditions, close physical contact among household members, and recently environmental contamination is reported to be a potential mediator of S. aureus transmission and possible reinfection within the household.1819) The relationship between S. aureus colonization of household contacts and the occurrence of S. aureus infection should be studied in this case as well. Precautions to minimize the transmission and decolonization might be useful to reduce the incidence of S. aureus infections among Korean children, and their effects should be studied.
Additionally, PVL-positive MSSA is not well known and the pathogenic potential is probably underestimated. Increasing the awareness of healthcare providers in the community may be important in preventing PVL-producing S. aureus infections.
 XML Download
XML Download