

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Eosinophilic esophagitis (EoE) is a chronic inflammatory condition thought to be caused by food and/or aeroallergen exposure [1]. Compelling evidence points to food antigens as the principle trigger, with multiple studies showing that elimination diets can resolve (and upon reintroduction, cause) the eosinophilic inflammatory infiltrate typical of EoE [2345]. Therefore, elimination diet is advocated as a first line management strategy [6]. However, the duration of dietary therapy required to define success is arbitrary, may vary across treatment centres [45], and there are no data examining the impact of different lengths of initial treatment on outcomes. Confirmation of treatment response requires endoscopy and oesophageal biopsy, but as there is no agreement on what level of oesophageal eosinophilia constitutes a histologic response, a variety of thresholds are employed, with some studies specifying a response as <15 eosinophils per high power field (HPF), and others choosing <5 eosinophils per HPF [78]. Moreover, success of dietary therapies varies across centres, possibly directly because of this difference [9].
Clarification of the optimal duration of dietary elimination required to induce remission is of critical and immediate clinical relevance. Studies of elemental diet showed symptom improvements in less than 2 weeks, but analogous histologic data are not available and no data are available for empiric elimination diets [10]. Based on clinical experience, we postulate that longer durations of dietary elimination may lead to higher response rates and a greater percentage of patients who benefit from a nonpharmacological approach. The aim of this study, therefore, was to determine if prolonged (>6 weeks) dietary elimination can resolve eosinophilic infiltration of the oesophagus in patients with EoE who had a partial or incomplete initial response.
MATERIALS AND METHODS
The research was performed in 2 centres. First, the records of a group of patients previously enrolled in a prospective clinical study (including the 6 food elimination diet, avoiding gluten, dairy, egg, soy, fish/shellfish, and nuts)based in Melbourne Australia (between December 2013 and January 2016, and described in detail previously [2]) were searched. Second, at the University of Chapel Hill, North Carolina (UNC), Division of Gastroenterology and Hepatology, a retrospective chart review was conducted of all patients with a diagnosis of EoE presenting to the UNC, Division of Gastroenterology and Hepatology between the 1st of January 2011 and 1st of April 2017, who received elimination diet therapy followed by upper gastrointestinal endoscopy and biopsy, following a structured clinical algorithm described previously [11]. In addition, records of patients involved in an ongoing prospective study of dietary therapy guided by novel allergy tests (and thus avoiding a more limited number of food groups) were also interrogated. In all cohorts, electronic medical records were used to validate the identified subjects, and to collate physician records, endoscopy findings and histopathology reports. Demographic information (age, sex, body mass index), comorbidities, medications, duration of EoE and previous treatment of EoE were recorded. The date of index (diagnostic) upper endoscopy and biopsy, commencement of dietary therapy, subsequent endoscopy and biopsies, symptoms (defined by dysphagia, odynophagia or food bolus impaction events, and graded as absent, mild, moderate or severe by the treating clinician), endoscopic appearance (using the EoE endoscopic reference score – EREFS, as described previously, also see Table 1 and histology reports were noted [1213]. Histologic response (<15 eosinophils per HPF) was defined based on the clinical report of an expert pathologist. Only patients who had histological evidence of active oesophageal eosinophilia (>15 eosinophils/HPF) after at least 6 weeks of dietary therapy, and who went on to receive an extended course of the initially prescribed dietary elimination followed by repeat oesophageal biopsy were included. The study was approved by the UNC Institutional Review Board (approval number: 17-1708), and the ethics committee of Eastern Health, Melbourne Australia (E19/1213). All patients were consented in the required fashion.
Table 1
Resolution of esophageal eosinophilia with prolonged elimination diet

D, distal esophagus; P, proximal esophagus.
*EREFS is an acronym for a 5-item scoring system of the appearance of the esophagus at endoscopy. The features noted are edema, rings, exudates, furrows, and strictures.
![]()
RESULTS
Seven patients were identified who had a partial reduction in eosinophil count in response to an initial course of elimination diet, and following extended dietary elimination met histological criteria for response. Five patients from Chapel Hill, North Carolina (from a total of 68 attempting elimination diet), and 2 patients from Melbourne Australia (from 52 attempting elimination diet) had such a response, equating to 5.8% (7 of 120). This subset of patients is in addition to those responding to elimination diet at 6–8 weeks, with 29 of 52 (52%) response (Melbourne Australia), and 25 of 68 (37%) initially noted. Patient characteristics and temporality of treatment response are detailed in Tables 1 and 2 and Figs. 1 and 2 (subject numbers as described in Tables 1 and 2 also apply to Figs. 1 and 2). The average of the peak oesophageal eosinophil counts prior to commencing dietary elimination was 38.5 (range, 15–65). Following the initial period of dietary elimination lasting between 6–8 weeks (mean 6 weeks and 4 days) the eosinophil count decreased to an average of 21.5 (range, 15–40). Finally, after an extended period of dietary elimination (mean of 13 additional weeks; range, 7–22 weeks), histological resolution (<15 eosinophils per HPF) was achieved (average peak eosinophil count of 5.2; range, 0–14) in all cases.
Table 2
Characteristics of patients with slow resolution of esophageal eosinophilia with dietary therapy

PPI, proton pump inhibitor; PO, per oral.
*6 Food elimination diet compromised initial complete avoidance of wheat and/or gluten, dairy, egg, soy, nuts, and fish/seafood.
![]()
 | Fig. 1Sequential images at endoscopic images demonstrates improvement at 6 weeks (A to B) with corresponding symptomatic resolution) despite persistence of esophageal eosinophilia. Images for subject numbers 1–4 are shown. (C) When dietary therapy was allowed to continue, endoscopic appearance remained stable or improved further.
|
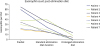 | Fig. 2Prolonged duration of elimination diet results in further decline in esophageal eosinophil count demonstrated at biopsy (eosinophils per high power field [HPF]). Elimination diet=avoidance of 1 or more food groups, and subsequently determining if this has induced a remission by performing endoscopy and biopsy. Most commonly 6 foods are eliminated, which according to standard protocols are: wheat and/or gluten, dairy food, eggs, soy, nuts, and fish (including shellfish). Standard elimination diet duration= approximately 6 weeks. Extended elimination diet duration= approximately 13 additional weeks.
|
The endoscopic appearance (EREFS score,) improved significantly between the index endoscopy (mean score, 6.4; range, 5–8) and subsequent endoscopic assessment (mean score, 2.0; range, 1–4; p = 0.018, Wilcoxon) after the initial period of dietary elimination, and remained substantially improved after histologic response was achieved (mean score, 0.6; range, 0–3). All patients described an improvement in symptoms following the initial period of dietary elimination, and this was sustained with extended dietary measures.
DISCUSSION
The duration of dietary therapy required prior to endoscopy and determination of response by biopsy and eosinophil count has been empirically set at 6 weeks, and several trials have demonstrated efficacy of between 52%–74% using this length of treatment [234514]. We herewith present 7 cases where extension of dietary therapy for mean additional 10 weeks (range, 5–22 weeks) resulted in histologic resolution of EoE (<15 eosinophils per HPF) where the shorter 6-week initial treatment course failed using a histologic outcome alone. This presents an alternative approach to current recommendations, and if replicated in a larger patient population, has the potential to alter management algorithms. The unifying features of this cohort includes the improvement in endoscopic appearance and symptoms after the standard 6 weeks of elimination diet, despite persistence of oesophageal eosinophilia traditionally equated with active EoE. This also raises the question of whether a single treatment outcome of EoE, for example a relatively arbitrary eosinophil count threshold, should predominate in terms of management decisions.
The patients described in this case series are typical of larger studies published by our respective centres and elsewhere, with a male predominance and comorbid atopic illness [215]. While chance alone is always presented as an explanation for hitherto novel observations (and remains possible in smaller studies), this well characterised group had biopsies of the upper and lower oesophagus, had progressive reduction of eosinophil count between all sequential endoscopies, and improvement in clinical and endoscopic features that would be in keeping with slow (or incremental) improvement over time. Admittedly, medications that could influence eosinophil count were used to treat asthma in 2 of the patients (inhaled corticosteroids, aspirin), although no change in medication frequency or dose was made throughout the course of dietary therapy, and with these medications one could argue that any improvement might be limited to the proximal oesophagus. The 2 centres differed slightly in the administration of the elimination diet, the 6 food elimination diet used in Melbourne Australia was more expansive (than that employed in Chapel Hill North Carolina) in that it excluded gluten instead of simply wheat, although it is unlikely that this influenced the slow resolution of eosinophilia discussed, which was nevertheless observed across both groups (and it is as yet unknown if gluten or wheat per se is the trigger for EoE) [211].
In conclusion, we propose that a subset of patients with EoE will benefit from a prolonged period of food elimination before this therapy is declared a failure, and alternative therapies which could include long-term topical corticosteroid use or repeated oesophageal dilatation are utilised. What proportion of patients will benefit, and thus currently are being declared a treatment failure with dietary therapy, is unknown. Given that all the patients described had an initial decline in eosinophil count (albeit not below 15 eosinophils per HPF), improved endoscopic appearance and symptom relief, this triad presents a useful starting point to define a group potentially able to benefit from continued dietary avoidance. Future larger multicentre studies that interrogate pre-existing databases to determine if eosinophil count in fact decreased following dietary elimination (in patients nonetheless classified as nonresponders) may present a clue as to further ‘missed’ cases likely to be similarly helped by extended periods of dietary therapy.
 XML Download
XML Download