

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cashew plant (Anacardium occidentale L.) belongs to the Anacardiaceae family. While it is native to South America, A. occidentale is cultured in Africa and Asia. The kidney-shaped cashew nut sprouts out externally from the cashew fruit. It is protected by a double-layered hard shell that is toxic and requires processing prior to consumption. Just as the prevalence of peanut allergy is on the rise in Western populations, recent studies suggest a similar trend for cashew nut allergy [12]. In the United States, cashew nut and walnut allergies are the most common tree nut allergies accounting for 15%–30% of all tree nut allergies [3]. In Sweden, a 10-year review estimated the prevalence of cashew nut allergy to be 6% of their food allergy cohort, with evidence of increasing frequency and severity of cashew nut allergic reactions [1]. Cashew nut is commonly consumed in Singapore and in Asia as a snack, as well as used in Indian, Thai, and Chinese cuisines. A study in Leicester comparing White children with South Asian children found the latter to be more likely to be sensitized and allergic to cashew nuts, with a relative risk of 1.94 and 2.59 respectively [2]. There have been no Asian studies looking specifically into cashew nut allergies [456]. An estimated prevalence of self-reported tree nut allergy in Singapore in 2010 was 0.3% [7]. The aim of this study was to investigate the clinical characteristics of cashew nut allergy in Singaporean children.
MATERIALS AND METHODS
A retrospective analysis was conducted between 2008 and 2015 in KK Women's and Children's Hospital, the main tertiary paediatric referral centre in Singapore. Subjects were identified based on a positive IgE (≥0.35 IU/L) to cashew nut in children younger than 18 years. There were no exclusion criteria. These included both cashew nut allergic and cashew nut sensitized children. Clinical notes of subjects were reviewed and data including demographics, atopic comorbidities, clinical reaction to cashew nut, associations with other nuts and test specific measurements were collected.
Associations with other nuts were classified to be allergic, sensitized, tolerant, or unknown. In this study, nut allergic children were defined as subjects who had a documented reaction to the specific nut (that was convincing of an IgE-mediated allergic reaction), with a positive IgE, and/or a positive skin prick test (SPT) (≥3-mm wheal). Nut sensitized children referred to subjects with no known prior exposure to that specific nut but a positive IgE, with or without a positive SPT. Nut tolerant children referred to subjects documented to have no clinical reaction upon ingestion regardless of IgE or SPT results. Subjects in the unknown category referred to those who had not been exposed to the nut and in whom IgE and SPT to the nut had never been performed. Cross-reactivity included subjects who were either allergic or sensitized to a specific nut.
For IgE serologic measurements, we measured specific IgE to cashew nut by using the ImmunoCAP System FEIA (Phadia, Thermo Fisher Scientific Inc., Uppsala, Sweden). For SPT measurements, the skin was prepped with alcohol and cashew nut extract (Stallergenes Greer, Lenoir, LC, USA) was applied to the skin of the dorsal forearm using a sterile disposable applicator, Duotip-Test (Lincoln Diagnostics, Decatur, IL, USA). The mean diameter was calculated from the average of the 2 largest measurements that were perpendicular to each other, and then subtracted by the wheal size of negative control (if any).
Descriptive statistics were analyzed to characterize the population. Ethics approval was obtained from SingHealth Centralised Institutional Review Board (reference number 2015/3084).
RESULTS
A total of 99 subjects were identified. Of these, 52 were cashew nut allergic with a documented clinical reaction that was in keeping with an IgE-mediated reaction to cashew nut while 47 were cashew nut sensitized, with no prior exposure to cashew nut. The demographics of subjects identified are summarized in Table 1.
Table 1
Demographic features of subjects included in study (n = 99)
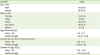
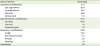
Table 2 summarized the type of clinical reactions subjects reported. In this study, cutaneous manifestations were the most prevalent (71.2%). These included urticaria (53.8%), eye angioedema (30.8%), lip angioedema (19.2%), and perioral rash (1.9%). This was followed by gastrointestinal manifestations (44.2%) and respiratory manifestations (30.8%). Gastrointestinal manifestations included vomiting (40.6%), diarrhea (1.9%), and abdominal pain (1.9%). Respiratory manifestations included cough (13.5%), shortness of breath (11.5%), wheeze (3.8%), and sneezing (1.9%). Notably, 2 subjects (3.8%) suffered from anaphylaxis. One of the 2 patients presented with shortness of breath and hypotension at 4 years old, without cutaneous signs, while the other 2 year old presented with urticaria, drowsiness, and hypotension. Anaphylaxis in this study was based on the World Allergy Organization guidelines [89].
Table 2
Clinical reactions documented among cashew nut allergic subjects
Only 4 subjects in our cohort underwent an oral food challenge (OFC). The first subject was a Caucasian boy who was found to be sensitized to cashew nut (SPT wheal size 5.5 mm, IgE 0.38 kU/L) at 1.3 year old, with no prior cashew nut exposure. At 2 years old, he failed the OFC as he developed urticaria after taking 1,680 mg of cashew nut protein. A second subject, a peanut-allergic Chinese boy, was found to have a SPT wheal size of 2 mm to cashew nut at 2 years old, repeated at 4 years old (SPT wheal size 8 mm), then at 6 year old (SPT wheal size 9.0 mm, IgE 0.83 kU/L). At 6 years old, he passed a cashew nut OFC and tolerated 5,300 mg of cashew nut protein. The third subject was an Indian boy who was diagnosed with cashew nut allergy at 2 years old, after experiencing urticarial rashes and shortness of breath within 30 minutes of cashew nut ingestion. His SPT wheal size then was 11 mm and IgE to cashew nut 3.61 kU/L. Subsequent reassessments at 4, 5.5, and 7 years old revealed improving downward trend of the SPT/IgE readings, to 7 mm/1.03 kU/L, 6.5 mm/0.5 kU/L, and 5 mm respectively. He passed the OFC at 7 years old (tolerated 4,400 mg of cashew nut protein) and was deemed to have outgrown his cashew nut allergy. The fourth subject was a Sri Lankan boy who had an acute clinical reaction to cashew nut ingestion at 1.5 years old. His first allergy evaluation at 3 years old confirmed the diagnosis of cashew nut allergy (SPT wheal size 12 mm). The repeat SPTs done at 4 and 5 years old were 12.5 mm and 7.5 mm, respectively. His first IgE to cashew nut performed at 5 years old was 0.72 kU/L. He too was deemed to have outgrown his cashew nut allergy after passing a cashew nut OFC at 5 years old.
We sought to determine tree nut allergy profiles among cashew nut allergic subjects (Table 3). About half of the cashew nut allergic subjects (51.9%) were evaluated for cross-reactivity to pistachio, and all of them were found to be either allergic (48.1%) or sensitized (51.9%) to it. Cross-reactivity of other tree nuts ranged from 34.8% to 44.7%. Peanut allergy among cashew nut allergic subjects was also explored. Cross-reactivity with peanut was 53.8% (36.5% [n = 19] were peanut allergic, 17.3% [n = 9] were peanut sensitized), 38.5% (n = 20) were clinically tolerant.
Table 3
Nut allergy profile among cashew nut allergic subjects

Among the cashew nut allergic subjects, 71.2% had concomitant allergic rhinitis, 69.2% had atopic dermatitis, and 23% had physician diagnosed asthma. The SPT wheal size's mean was 8.7 ± 4.1 mm, and median (range) was 9.0 mm (0.5–17.5 mm). Cashew nut specific IgE levels had a mean of 15.6 ± 23.8 kU/L and median of 5.5 kU/L (0.38–95.3 kU/L).
DISCUSSION
Singapore is a multiethnic society comprising of 74.1% Chinese, 13.4% Malays, 9.2% Indians, 5.2% others [10]; others referring to Caucasians and communities otherwise specified. Our study cohort consisted of a relatively low numbers of Malays, and relatively higher numbers of Indians and Caucasians. A study conducted in Singapore and Philippines similarly revealed higher prevalence of tree nut allergies among Indians and hypothesized a genetic predisposition among ethnic groups to allergic disease [7]. Another possible reason for higher prevalence of cashew nut allergy among Indians may be due to earlier and higher exposure to cashew nuts as a result of their diet. The greater proportion of Caucasians in our study is not surprising given the steady increase of nut allergy numbers in the West [11].
The findings of our study on clinical reactions are similar to other studies on cashew nut allergic subjects, with cutaneous manifestations being the most common [1213]. Nearly half of these children (44.2%) had gastrointestinal symptoms as their initial presentation. In contrast, a prospective study evaluating cashew nut allergy using double-blind placebo-controlled food challenges yielded gastrointestinal symptoms as the most common allergy manifestation [11]. A likely explanation of this difference in presentation would be due to the nature of a retrospective review. During recall, patients would usually perceive cutaneous symptoms as allergic reactions and not the gastrointestinal symptoms. On the other hand, during a supervised food challenge, physicians would actively look out for and advise patients to report all the possible symptoms.
Only a small number of our cohort had undergone a formal OFC, of which only 1 of 4 was from the cashew nut sensitized group. An OFC is still considered as the gold standard of diagnosis of a food allergy. About half of our cohort (47%) were found to be sensitized to cashew nut, with no prior exposure to cashew. Ideally, these patients should undergo an OFC to confirm clinical allergy versus tolerance. These children were assumed to be cashew allergic and advised strict avoidance, which in some, may be unnecessary. However, conducting OFCs in all such instances with positive blood or SPT results is resource intensive. A study conducted in Netherlands has recently proposed a prediction model comprising gender, SPT measurements and sIgE levels [14].Using the prediction model and a scoring system, the study reported greater discriminability in identifying subjects who have a ≥97% chance of a positive OFC compared to isolated sIgE levels. This model appears promising and needs to be validated in other larger populations before routine clinical use.
Our findings also confirmed that cashew nut is an important cause of food-induced anaphylaxis, with an anaphylaxis rate of 3.8%. This anaphylaxis rate is however a much lower rate compared to other reports – 74% in a retrospective study conducted in Brisbane, Australia [12], 38% in a study conducted in Southampton [15]. This is possibly due to differences in the definitions of anaphylaxis used. In our centre, anaphylaxis is diagnosed if the child fulfilled the diagnostic criteria set out by World Allergy Organization guidelines [8], and the definition of being a “serious, generalized or systemic, allergic reaction that can be life-threatening or fatal” [9]. The lower incidence of anaphylaxis in our population could also be due to a true difference, in which we may be seeing a milder severity phenotype in our local population. Better homogeneity of case definitions in future prospective studies is needed for more meaningful comparisons.
Cross-reactivity with pistachio was also evident among our cashew nut allergic subjects. About half of our cashew nut allergic subjects (51.9%) were further evaluated for pistachio allergy and sensitization. All tested were found to be either pistachio allergic (48.1%) or cosensitized (51.9%). The reason why nearly half of our cohort was not evaluated for pistachio coreactivity was because pistachio was not part of the standard tree nut extract SPT panel, and prick to prick to pistachio was not a routine practice then. Our findings were in keeping with numerous studies which have described high levels of cosensitization with pistachio [11131617]. The true extent of clinical relevance of cosensitization to pistachio needs to be further evaluated by OFCs. A recent prospective study which performed a double blind placebo controlled food challenge with pistachio nut on cashew nut allergic and sensitized subjects found that only about one third of these subjects had clinically relevant pistachio nut allergy [16].
Peanut tolerance was found in 38.5% of the cashew allergic cohort. Tolerance to hazelnut, walnut, almond and Brazil nut ranged from 50% to 57.7%, amongst cashew allergic subjects. A study conducted in the United Kingdom proposed confirmatory challenges to nut allergic subjects to reduce the psychological impact of unnecessary dietary restriction for other nuts [18]. Indeed more data is now emerging to support such an approach. The NUTCRACKER [16] study demonstrated a challenge-proven rate of coallergy to more than one tree nut to be less than 30%; and coallergy between both walnut and pecan, and between cashew nut and pistachio being the most significant.
Notably, there were 3 patients who were deemed allergic to cashew nut based on clinical history but had a negative SPT (<3 mm). A closer examination of these 3 cases revealed possible explanations. The first patient was first seen by the allergy clinic for evaluation of multiple food allergies (including peanut) at 2 years of age. The reported reaction of urticarial rashes to cashew nut was at 9 months old. His SPT wheal size was 2.0 mm, and cashew nut specific IgE was 0.47 kU/L. The second patient's reported reaction was “numbness of the tongue” at 2 years old, and first SPT performed at 4 years old was 0.5 mm, with IgE of 1.04 kU/L. The third patient had his first allergy workup performed for cashew nut at 14 years old, while the reported reaction of shortness of breath to cashew nut was at 3 years old. His SPT wheal size was 1 mm, and cashew nut specific IgE 0.64 kU/L. All 3 patients had equivocal history of a clinical reaction to cashew nut, and an OFC would have been useful.
Strengths of this study include the ability to describe allergic profiles of a large number of cashew nut sensitized children in Singapore. This study is the first to look specifically at cashew nut allergy in Singaporean children. Limitations of this study include having no control group of cashew nut tolerant patients for comparison. Subjects in this study were identified based on a positive IgE to cashew nut, and hence there is a possibility of missing out patients who are cashew allergic but with a negative IgE result to cashew nut. Determination of cashew nut allergy was based on self-reported clinical reactions instead of double blind-placebo controlled food challenge which is the gold standard towards determining allergy. Prospective studies are required for us to better understand cashew nut allergy among Asian populations.
To conclude, cashew nut allergy is a significant tree nut allergy in Singapore, especially amongst the Chinese, Indian and Caucasian races. Most of the cashew nut allergic children presented with cutaneous reactions, though it is still an important cause of food-induced anaphylaxis.
 XML Download
XML Download