

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nasal polyposis (NP) is a chronic disease presenting with nasal obstruction as the most frequent complaint [1]. Even though the etiology of NP is still vague, many aspects of the disease including risk factors and related morbidities have been studied extensively. It has been documented that NP results in deterioration of quality of life and disturbances of sleep [23456]. However, remarkable consequences of NP such as psychological and cognitive outcomes are relatively poorly studied [7] and supplemental data on these topics is warranted to develop a multidisciplinary and more effective management policy in NP.
Electroencephalography (EEG)-derived event-related potentials (ERPs) are sensitive tools to monitor attention and concentration. Since ERPs are free from cultural and educational influence, they can provide inexpensive and noninvasive insights into the cognitive process [8910]. Particularly, the auditory P300 component is a sensorial perception brain process and electrophysiological event that depends on previous acoustic experience.
It arises as the individual's reaction to a formerly established stimulus and thus, it reflects the conscious interaction of the auditory system with the somatosensorial cortical area and necessitates the active mental participation of the patient. Hence, analysis of P300 can yield valuable objective data about cognitive function [1112].
Previous publications demonstrated that deprivation of sleep results in extension of latency and reduction of amplitude in the auditory P300 amplitude, which reflects a lowered state of awareness [13]. To the best of our knowledge, deterioration of cognitive function due to nasal obstruction in NP has not been reported in the medical literature before now.
The aim of the present study was to evaluate attention and concentration as reflected in changes of P300 latency in patients suffering from chronic hypoxia due to complete nasal obstruction in advanced NP. If such an association can be established, timely identification and more effective management of these relatively less known consequences may be feasible.
MATERIALS AND METHODS
Study design
We performed the current cross-sectional, case-control study in the neurology department of our tertiary care center between 2013 and 2015. The trial was implemented on 60 cases comprising 30 patients with nasal polyps and 30 healthy controls. This study was supported by the Institutional Review Board of Kafkas University Medical Faculty (approval number: 80576354-050-99/117). Written informed consent was given by all participants. This trial was implemented in accordance with principles in the Declaration of Helsinki and good clinical practice guidelines.
Exclusion criteria consisted of presence of systemic problems including cardiac diseases, diabetes mellitus, asthma, obstructive sleep apnea, neurological diseases, hearing loss, or psychological disorders.
Diagnosis of NP was made by the same otorhinolaryngologist according to the proposed criteria and its severity was graded as reported in the literature [14]. Extent of polyps was evaluated based on a 3-point classification system: (1) nasal polyps confined to the middle meatus, (2) nasal polyps below the level of middle turbinate but not causing total obstruction, and (3) nasal polyps causing total obstruction [15]. All patients included in the current study had grade 3 nasal polyps that completely blocked the nasal cavity.
Technique for ERP recording
Recording of ERP was made in accordance with the principles suggested in the recent publication by Yaman et al. [16]. Reproducibility and reliability of the measurements for P300 have been established by studies in normal controls after repeated recordings. In every session, amplitude and latency measurements of P300 were made. Routinely, the P300 recordings were accomplished after overnight sleep prior to breakfast (at 9 AM). All measurements were carried out by the same electrophysiologist in our department, who was blind to patient treatment status.
We utilized a Keypoint G4 workstation equipment (Denmark) auditory oddball stimulus set-up in this study. Electroencephalographic activity was recorded at the frontal (Fz), central (Cz), and parietal (Pz) electrode sites of the 10/20 international system using Ag/AgCl electrodes, affixed with electrode paste and tape, with an impedance ≤10 k Ohm. The reference electrode was attached to the right earlobe, while the ground electrode was attached to the left earlobe.
A standard stimulus of 90-dB sound pressure level (SPL) intensity and 1,000 Hz and a target stimulus of 90-dB SPL intensity and 2,000-Hz frequency pure sound were used. Target stimuli constituted of 20% (n = 60) of 300 total stimuli and were given in between standard stimuli in a random fashion. Patients were instructed to avoid moving, talking, or blinking too much and to look at a fixed point in the middle of the computer screen. They were asked to press the button when they heard random target stimuli administered in between the auditory stimuli.
Before the experimental procedures, an adaptation period of 5 minutes was allowed for every patient and calibration of EEG was performed. Subsequent to the attachment of electrodes, patients were placed on an adjustable chair in an isolated room adjacent to the recording room. Subjects were asked to sit quietly with open eyes, follow the stimuli carefully, and to try to determine rare tones of 1,000-Hz frequency. The amplitudes were measured peak-to-peak.
Statistical analysis
Data was analyzed by means of IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). The normal distribution of variables was tested with the Kolmogorov-Smirnov test and parametric tests were used for variables with normal distribution. We performed the T test for independent-Samples in order to compare the values of P300 latency and age, between the 2 groups. Variables under investigation were expressed as mean and standard deviation. Confidence interval was 95% and level of significance was set at p < 0.05 for all statistical analysis.
RESULTS
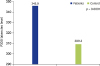
Average ages of NP patients and control group were 31.03 ± 10.1 and 32.08 ± 6.4 years, respectively. There were no significant differences between groups in terms of age (p = 0.5). As illustrated in Table 1 and Fig. 1, P300 latency of NP patients was delayed (345.8 ± 16.6 msec) more than that of the control group (309.3 ± 16.6 msec) (p < 0.001). However, there were no significant differences between control and NP in terms of amplitude of P300 (18.56 ± 6.16 mV; 16.90 ± 6.51 mV, respectively) (p > 0.05).

DISCUSSION
The current study was implemented to evaluate the alterations in concentration and attention in patients with NP. Our results demonstrated that latency of P300 was remarkably extended in NP and this finding may be attributed to chronic hypoxia especially at sleep linked with complete obstruction of nasal cavity in these patients. Thus, it can be speculated that NP may be associated with impairment of attention and concentration.
In the literature, the auditory P300 latency subcomponent was first clinically utilized in assessment of cognitive deterioration in Alzheimer disease [1718]. The auditory P300 ERP occurs when the patient is unexpectedly presented with the target stimulus during a stimulus discrimination task [1920]. This task necessitates the patient to actively relate with cognitive processing in the brain and deflection to the incongruent stimulus is measured by single or multi-channel electrode analysis [21]. The most commonly used stimulus discrimination task is auditory oddball, as we used in this trial, and the P300 component is a large positive deflection of ERP existing 300–500 msec after the stimulus [19]. It is triggered by the 2-tone auditory oddball task and measured at the Pz electrode where it has been shown to produce the most noteworthy P300 differences [22]. Two elements used in the analysis of P300 wave consist of the amplitude (size of the deflection) and latency (time elapsed after stimulus before activation). The amplitude indicates brain activity in the parietal-temporal and prefrontal areas related with auditory memory. Latency is linked with interstimuli frequency of the individual's attention and concentration. The P300 latency constitutes the most common aspect of the wave analyzed in studies investigating cognitive impairment [181920]. P300 latency is supposed to indicate processing of information after stimulus and executive functions such as memory, attention and integration of complex stimuli [2324]. Prolongation of the P300 latency has been linked with progressive cognitive decline [23].
A study demonstrated that in patients with severe obstructive sleep apnea syndrome (OSAS) a significant delay was observed in P300 latency possibly due to sleep deprivation. Notably in OSAS patients, attention deficit was more obvious in young people compared to the elderly [25]. This finding reminds us that impairment of cognitive function does not necessarily occur in conjunction with advanced age [26]. Our results imply an increased information processing time, which indicates that NP patients may require evaluation in terms of cognitive impairment. Since P300 is a sensitive marker for deterioration of cognitive function, systemic and neurological hazards of chronic hypoxia make NP a systemic disease rather than a local nasal pathology.
NP is usually a bilateral disease, and polyps primarily occur in the middle meatus and originate from the nasal mucous membrane of the outlets from the paranasal sinuses. Formation of nasal polyps is mostly induced by chronic inflammatory rhinosinusitis. Nasal blockage from polyps is caused by physical obstruction and a ball valve effect that occurs due to swinging back and forth of the nasal polyp, which prevents airflow [27]. Beyond its healthcare related burden, NP produces indirect costs by reducing productivity and performance [28].
In spite of many studies conducted to assess quality of life and likelihood of sleep disturbances in NP, cognitive and psychological morbidities linked with NP are still obscure.
As far as we know, this study is the first publication documenting a deterioration of cognitive function in NP. This finding may be attributed to chronic hypoxia due to compromised nasal respiration. Nasal obstruction and hypoxia bring about considerable social and economic burden due to impairment of attention and concentration. Hence, multidisciplinary evaluation of patients is crucial to establish an effective treatment regimen.
The main limitations of the current study include cross-sectional design and relatively small sample size. Furthermore, lack of analysis of inflammatory metabolic conditions and variability of nasal polyp size are important restrictions that limit extrapolation of our preliminary results. Also, it is possible that the results of P300 have changed due to psychologic problems caused by nasal obstruction. Although we excluded patients with psychologic disease in this study, psychologic problems not enough to be diagnosed as disease, such as irritability, annoyance, and mild depression, may cause a decrease of concentration. However, we hope that our results draw attention to the cognitive and psychological hazards of NP.
In conclusion, results of the current study imply that nasal obstruction in advanced NP may result in substantial cognitive impairment. Assessment of patients with the P300 latency subcomponent can be a useful diagnostic tool to detect cognitive and psychological consequences.
 XML Download
XML Download