

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prevalence of food allergy has increased within the last 2 decades, throughout the world [1]. Food allergy in Asia is less commonly observed than among Western countries [2]. With the advent of the social media, parents have become increasing concerned of food allergy and the information on food allergy is widely shared over the Internet. As a result, a large number of children were perceived to have food allergy based on history alone.
In the Thai society, children with suspicion of having food allergy are commonly subjected to diet elimination from all foods potentially causing allergic reactions (‘big 6’ or ‘big 8’ foods, i.e., cow milk, egg, wheat, peanut/tree nuts, soy, and seafoods-fish/shellfishes) without a proper medical evaluation. Such practice can cause undue stress to the families (frustration, apprehension) and difficulties in acquiring food substitutes. Moreover, these children are prone to develop nutritional deficiencies due to extensive food avoidance. There is an absolute need for conducting a proper diagnostic evaluation for food allergy to ensure that avoidance is limited to only those with true allergy to foods.
Oral food challenge (OFC), particularly double-blind, placebo-controlled food challenge (DBPCFC) is the gold standard for the confirmation of food allergy [34]. Among those children presented with parental complaints of food allergy, positive OFC could only be confirmed in 30% or less [56]. Despite such findings, OFC is infrequently performed in allergy practices due to inadequate procedural set up, risk for side effects and reluctance of physicians to carry out this effort-dependent procedure in busy daily practices [78]. In Asia, aside from China, Japan, Korea, and Singapore, reports of OFC results are limited [9101112]. Such scarcity of information has led to uncertainty of epidemiology of food allergy from this part of World such as types of foods commonly causing reactions, severity of the reactions and of efficacy/safety of the OFC procedure. In this report, we present our 16-year experience of OFC at the Siriraj Hospital, the largest hospital in Thailand and with the longest establishment of allergy services in this Thailand.
MATERIALS AND METHODS
A retrospective chart review of 228 children scheduled for OFC at the Allergy clinic of Pediatric Department, Siriraj Hospital, Mahidol University between 1996–2012 was conducted. Indication for OFC among these patients were major complaints of food allergy requiring confirmation (n = 210), chronic urticaria (n = 8), unknown recurrent anaphylaxis (n = 1), severe atopic dermatitis (n = 6), chronic vomiting from unknown cause (n = 1), and recurrent pneumonia from unknown cause (n = 2). Nineteen patients were excluded from the analysis due to incomplete chart data (n = 19), refusal for challenge (n = 1), and not showing up for OFC (n = 2). Data from 206 children and from a total of 306 challenges were analyzed (see Fig. 1 for flow chart of inclusion and exclusion of recruited subjects).
 | Fig. 1Study details indicating inclusion and exclusion of participants. DBPCFC, double-blind, placebo-controlled food challenge; OFC, oral food challenge.
|
The following data were obtained; demographic data (i.e., age, sex, race, associated allergic diseases, family history of allergic diseases and of food allergy) types of foods chosen for challenges, results of food challenges, skin testing wheal sizes, and specific IgE levels (when available).
Skin testing was performed using skin prick testing with commercially available extracts (ALK-Abello, Port Washington, Port Washington, NY, USA) and/or prick-to-prick test using cooked/uncooked foods when appropriate [13]. Positive skin testings were defined as those with wheal diameter of 3 mm greater than negative control. Serum food-specific IgE were measured using ImmunoCap system (Thermo Fisher, Uppsala, Sweden) and SpIgE value of ≥0.35 kUA/L was interpreted as positive with range from 0.35-over 100 kUA/L.
Food challenges were mainly performed in an open fashion (n = 297) with 9 challenges carried out by double-blind, placebo-controlled food challenge (DBPCFC). The method of open and double-blind OFC was performed following standard recommended protocol [14]. During the early part of the study (prior to 2010), DBPCFC was performed using placebo and active foods packed in capsules [15]. This was later changed to the current recommendation using masking media suitable for individualized foods suspected [14]. Food challenges were supervised by allergists/allergy fellows prior to, during, and after challenges to classify negative/positive reactions. Positive challenges were defined when patients developed significant symptoms/signs in one or more of the following body systems; cutaneous system (maculopapular rash, urticaria, angioedema), respiratory system (rhinorrhea, cough, wheezing), gastrointestinal system (nausea, abdominal pain, vomiting, diarrhea), neurological system (drowsiness, sudden change of behavior, change of consciousness, convulsion), and cardiovascular system (hypotension, cardiovascular collapse). The study was reviewed and approved by the Human Ethic Committee of the Faculty of Medicine Siriraj Hospital (approval number: 394/2556).
During the study period, there were 2 separate major studies on food allergy involving OFC conducted at our institute (on shrimp and wheat allergy). For the shrimp study, 68 patients with convincing history of shrimp allergy and with positive skin testing to shrimp extracts were challenged on separate sessions to large water shrimp (Macrobrachium rosenbergii) and to large tiger prawn (Paneus monodon) [16]. Twenty-five patients from the shrimp study was included in this review (with 7 gave positive results – 28%). The wheat OFC study involved those with definite wheat allergy at one point of time in life to determine the natural history of wheat allergy [17]. Eleven patients were included in this review (with 5 positive challenge – 45%).
Statistical analyses were performed using IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA). Descriptive analysis were used for describing demographic data, results of OFC, type of foods, frequencies of symptoms and signs of positive/negative challenges. Association between results of challenges pertaining to demographic data, skin testing, SpIgE were analyzed by using the chi-square test.
RESULTS
The mean age (±standard deviation [SD]) of the 206 patients were 5.85 ± 4.22 years (range, 4 months to 17 years). All patients were Thai. There were 65 patients within the younger age group (<3 years old) and 141 patients in the older group (≥3 years old).
Sixty of 206 patients (29%) had positive OFCs whereas 84 of 306 challenges (27.5%) were positive. The mean age (±SD) of patients with positive challenges was 6.7 ± 4.6 years old. No statistical significant association between age, sex, history of other allergic diseases, family history of allergic diseases, and results of challenge (Table 1). Positive challenges were observed more frequently among females (28 of 81, 35%) than among males (31 of 125, 26%).
Table 1
Demographic data of the study population (n = 206)

Values are presented as mean ± standard deviation or number (%).
*All: 5.85 ± 4.22. †Allergic diseases: asthma, allergic rhinitis/conjunctivitis, and atopic dermatitis.
![]()
Shellfish accounted for the largest number of positive/total challenges (29 of 71 challenges 40%), followed by wheat (19 of 48 challenges, 40%). Other foods with positive/total challenges were cow's milk (14 of 66 challenges, 21%), egg white (8 of 47 challenges, 17%), egg yolk (7 of 29 challenges, 24%), soy (3 of 18 challenges, 17%), chicken (2 of 8 challenges, 25%), and banana (2 of 3 challenges, 67%). Few foods giving only negative results were fish, pork and beef.
As shown in Table 2, 65 children were 3 years of age or less. Positive challenges were observed in 15 of 65 children in this group (23%). The most common food with positive challenges for this group was wheat (7 patients), followed by cow's milk (6 patients), egg white (4 patients), egg yolk (4 patients), and chicken (2 patients). For those 3 years of age and older (141 children), 214 challenges were carried out. Forty-five children (32%) had positive OFC (61 challenges). Shellfish was the most common food causing positive challenges (29 patients), followed by wheat (12 patients).
Table 2
Results of positive/total oral food challenges of foods types among children of the 2 age groups
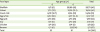
Values are presented as number of positive/total challenges (percentage of challenges according to each food).
![]()
Reactions of cutaneous system were most commonly observed (and accounting for the only system involved in 57.1%). Moreover, cutaneous reactions were found in conjunction with every reaction of other body systems among those with reactions involving more than one body system. Anaphylaxis occurred only in 1 subject underwent OFC to wheat. The patient responded well to adrenaline administration. Oral allergy syndrome was observed predominately to shellfish (Table 2).
Skin testing was performed in 98.4% of patients. Among those with positive OFC, skin test was positive in 70%, whereas among negative OFC, the test was positive in 23% (p < 0.01). Specific IgE was performed in 56.9%. It was positive in 66% and 42% in a group with positive and negative OFC results accordingly (p = 0.07).
DISCUSSION
The low of positive OFC rate in our study (29%) confirms earlier findings by Bock and Atkins [5] and by Fleischer et al. [6]. Moreover, patients in this study included those previously recruited for our shrimp and wheat studies, we therefore anticipated a much higher positive OFC rate. Since this is a retrospective data, we were not able to collect complete data on presenting symptoms that may/may not be used for predicting positive challenges. Surprisingly more females gave positive OFC than males which is in contrast to findings reported on epidemiology of food allergy, particularly in younger ages [4].
Despite the fact that some of shrimp challenges (25 challenges) was recruited from our previous of shrimp study, results of positive challenges (28%) among these patients were lower than overall positive shrimp challenge in this review (40%). This indicates that shrimp is truly a major food allergy among Thai children, confirming the results of previous epidemiologic study that shrimp are the most important foods causing allergic reactions among older children in Thailand [8].
In this study, wheat was the second most common food giving positive challenge (total positive rate of 40%). Seven out of 10 children with age less than 3 years had positive wheat OFC whereas the rate is lower for those over 3 years old (31.5%). This suggests that wheat allergy can present quite early in life. As with shrimp, a small number of wheat OFC (11 patients) was from our previous study on natural history of wheat allergy in children. Since eggs was the food with the largest number of subjects recruited for OFC in this review (n = 76) follows by cow's milk (n = 66) and wheat (n = 48), we therefore feel that selection of subjects in our study reflected the real clinical situation occurring in the Thai community. In addition, the result of our study supports the notion by several Thai allergists that there is an increase in numbers of children with wheat allergy in Thailand. A large scale epidemiologic study for wheat allergy in Thailand is warranted.
It is of note that systemic reactions from shrimp from this study were quite serious. Eight of 29 patients with shrimp sensitivity developed symptoms to more than one body system, some of which was severe reactions. However, no anaphylaxis was observed with shrimp challenges (only 1 patient had anaphylaxis during a wheat challenge). Similar to a report from Singapore, oral allergy syndrome was only observed among those with positive shrimp challenge [18].
In conclusion, positive OFC occurred only in 30% of patients in this review. This confirmed that OFC is needed to confirm the diagnosis of food allergy. Shrimp allergy was the most common cause of positive challenges. A large number of wheat OFC in this study suggested an increase in wheat allergy in Thailand.
 XML Download
XML Download