

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The increase in the prevalence of food allergy, observed in some regions of the world, it has been considered as a second wave in the epidemic of allergic diseases [1]. This phenomenon has been observed, both in pediatric and adult population [23]. The prevalence of self-reported food allergy shows variations ranging from 0.4% to 6.0% [4].
For its potential to cause severe or fatal allergic reactions, nuts such as peanuts, walnuts and sesame seeds or seafood such as shrimp, fish or crab, have received more attention. Thus, the prevalence of nut or peanut allergy in the adult population has been estimated at 1.3% [5] and for seafood at 2.3% [6]. However, seeds like almond, hazelnut, chestnut, pistachio and sunflower seed or seafood such as octopus, oyster and clams, have been scarcely studied.
In developing countries, there is a lack of epidemiological information related to food hypersensitivity, including nuts and seafood [78]. The possible variations in the prevalence of allergic reactions to food due to habits and customs as well as the availability of foods that depend on geographical conditions it is unknown. For these reasons, the objectives of this study are to determine the prevalence of allergic reactions associated with the consumption of nuts and seeds or seafood and to identify the types of foods, as well as to describe the clinical manifestations most frequently related to allergic reactions in a sample of university students.
MATERIALS AND METHODS
Design and subjects
The methods of this study have been previously described [9]. In summary, from a universe of 25,269 students enrolled in the Autonomous University of the State of Mexico, 1,200 students between 18 and 25 years of age, born in the State, were selected and analyzed transversely from February to May 2014.
Questionnaire
Hypersensitivity to nuts and seeds, and seafood was determined through a structured questionnaire [9], answered by each participant. The instrument investigated demographic variables and the personal or family history of allergic diseases diagnosed by a physician. Then, if the subjects reported any adverse reaction related to the consumption of any food, they were been questioned about any discomfort associated or not with the consumption of some nuts and seeds, or seafood.
Definitions
For this study, a perceived allergic reaction was defined if the subjects answered positively to the question: Do you have any discomfort, reaction or symptoms after eating some food or drink? Then, if the adverse reaction was associated to nuts and seeds or seafood. A probable allergic reaction was considered when the participants answered affirmatively to the previous question and the symptoms were typical of those involved in allergic reactions, for example, skin, urticaria and angioedema; respiratory system, shortness of breath, wheezing, and throat tightness; gastrointestinal system, vomiting and diarrhea, and the discomfort originated within 2 hours of ingestion of food [510]. A systemic reaction was defined when, in addition to the above, 2 or more organs or systems were affected.
Statistical analysis
The prevalence of a perceived, probable, and systemic allergic reaction to nuts and seeds or seafood was determined by calculating their frequency; and their respective confidence intervals at 95% (95% CI). Data was processing with the IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
Characteristics of the population
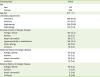
The sample of students analyzed consisted of 501 men and 699 women; the average age of the population was 19.7 years. Mainly medical students (43.1%) represented the sample. The most common atopic comorbidity was allergic rhinitis, followed by hypersensitivity to medications. The most common atopic disease in the mother and father was allergic rhinitis, 5.6% and 3.2%, respectively (Table 1).
Table 1
Characteristics of the study population and prevalence of personal and parental allergic disease (n = 1,200)
![]()
Characteristics of allergic reactions
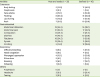
In subjects allergic to nuts and seeds, the main symptoms were gastrointestinal, and of them, abdominal pain, followed by abdominal distension and flatulence. In the skin, the most frequent discomforts were rash and flushing. Pharyngeal oppression was the main respiratory discomfort. On the other hand, in students having seafood allergy, again the most frequent intestinal discomfort were abdominal pain and abdominal distention. Half of all students with this allergy showed flushing and approximately 40% had body pruritus. In the respiratory symptoms, the sensation of pharyngeal oppression and sneezing were the most frequent clinical manifestations. In both cases, episodes of anaphylaxis were not documented (Table 2).
Table 2
Frequency of symptoms in 1,200 university students with allergy to nuts and seeds, and seafood
![]()
Estimated prevalence
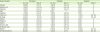
The prevalence of nuts and seeds perceived allergy was close to 3.0% where the most prevalent foods were the walnut (1.0%), Indian nut (0.9%), then the peanut (0.8%), and the least frequent were chestnut (0.2%) and date (0.1%). Probable allergy to nuts and seeds occurred in 0.8%, where walnut (0.5%) and Indian nut (0.4%) were the most frequent. Systemic reaction was documented in 0.2% of the students studied; again, the walnut was the most prevalent (Table 3).
Table 3
Prevalence of nuts and seeds allergy in 1,200 university students
![]()
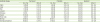
The perception of seafood allergy had a prevalence of 3.5%, where shrimp and octopus stood out (2.8% and 1.1%, respectively). Almost 2.0% of participants had probably allergy, again shrimp (1.7%) stood out as the most frequent. Finally, the prevalence of systemic reaction was 0.5% and shrimp was its main representative (Table 4).
Table 4
Prevalence of seafood allergy in 1,200 university students
![]()
DISCUSSION
Our study reported that 3% of university students had perceived allergy to some type of nuts and seeds: mainly walnuts and rarely peanut. On the other hand, the prevalence of self-reported allergy to seafood was 3.5%, with shrimp being the most frequent food. Intestinal discomfort was the main symptom in students allergic to nuts and seeds, and in the allergic ones to seafood, cutaneous symptoms.
In Mexico and elsewhere in Latin America, studies that estimate the prevalence of food allergy are scarce [78]. Even more, those related to nuts and seeds, and seafood that are more likely to cause severe illness. In addition, previously published studies analyzing the prevalence of food allergy usually focus on products such as peanut, sesame seed or shrimp [51112]. Our study provides valuable information in other foods. Here, 13 nuts and seeds, and 8 different seafoods were identified as allergenic. Among the nuts and seeds, the different types of nuts stood out, in less quantity almond and peanut.
In this study, the frequency for nuts varied from 0.3% to 1.0% depending on the nut species studied. In both Europe [4] and Canada [11], the overall prevalence of nut allergy was consistent with our data. However, the type of nut was not described. Only one study, conducted in the United States, reported the prevalence of allergy to different types of nuts, and these were 0.2% up to 0.8%, according to the nut species [5]. In this way, it seems that nut allergy in our country, is a problem similar to that observed in developed countries.
The prevalence of peanut allergy in our population was 0.8%, similar to that observed in North American countries [51113], or in another city of Mexico [14], but differed substantially from those found in Europe [4].
Sesame seed has emerged as an important allergen. As up to 0.3% of students reported a perceived allergy to it [5111213]; this differs markedly from what is observed in various regions of the world where the prevalence barely exceeded 0.1%. Another emergent allergen that has been gaining notoriety worldwide, are sunflower seeds; however, reports are scarce [15]. It showed a frequency similar to that observed with sesame seeds, pistachios or Brazil nuts (0.3% each), more studies will reveal the true dimension of this problem.
On the other hand, the perception of seafood allergy showed a frequency higher than that observed in other regions of the world, such as Canada [11], United States [6], or Europe [4].
Historically, the introduction of seafood to the usual diet of Mexicans did not take place until the time of Spanish colonization; therefore, there was a lower degree of exposure to this type of food, reflected by a low per capita consumption of seafood in our population [12].
The low seafood consumption could be a condition that favors immunological intolerance, thus facilitating hypersensitivity responses to seafood. Specifically, shrimp is the seafood that caused the most allergic reactions in students, and this is consistent with the findings of other regions of our country [1214]. Comparatively the prevalence of perceived and probable reactions to fish was higher in our population than in the United States [6] or Canada [11], but consistent with different European countries [4].
Symptoms of adverse reactions to food are diverse, which usually depend on: the amount of food ingested, the food preparation, other foods concomitant consumption, the age of the patient, the rate of food absorption, among others [16]. Symptoms that accompany allergic reactions to food are urticaria, angioedema, pruritus, cough, abdominal pain, and tachycardia.
In this study, intestinal symptoms were predominant in subjects allergic nuts and seeds; in contrast, cutaneous manifestations were the main symptoms in subjects allergic to seafood. Perhaps seafood allergic subjects are more likely to develop systemic reactions compared to those who are allergic to nuts and seeds [17].
In Germany, a population-based study showed that the most frequent symptoms were gastrointestinal, followed by cutaneous [18]. On the other hand, a study carried out in Colombia, showed that pruritus, rash and reddish skin were the most frequent symptoms [19]. However, neither of them determined the prevalence of symptoms according to food group. It is recommended that allergic symptoms should be categorized according to the food group that triggers discomfort, in order to establish patterns, such as that observed in oral allergy syndrome after consumption of Rosaceae family foods, such as peach, apple, plum, etc. [20].
In this study, we take into account our definition of systemic reaction (which may well correspond to anaphylaxis), it was observed a systemic reaction prevalence to nuts and seeds, and seafood of 2 of 1,200 (0.17%) and 6 of 1,200 (0.5%) respectively. In order to extrapolate the results to entire student population (25,269), it is estimated that 43 or 126 students with anaphylactic reactions triggered by nuts and seeds, and seafood. This is especially relevant for public health, if it is considered that nearly four million upper-level students enrolled in the 2014–2015 school year in Mexico [21] thus, there would be about 6,800 cases of anaphylactic reactions related to nuts and seeds and 20 thousand cases to seafood.
In the United States, the prevalence of anaphylaxis in a randomized adult population was 1.6%, food was responsible for 1 in each 3 episodes [17]. In Mexico, it was shown that 1.3% of a randomized adult population had food-related anaphylaxis. Shrimp, fish, and peanuts were the food mostly involved with this type of problem [14]. In another study, 5% of children with food allergies reported anaphylaxis to fruits, seafood and nuts and seeds as the main responsible foods [22].
More recently, a study of schoolchildren showed that 1.2% of the population analyzed had anaphylactic reactions as a manifestation of food allergy, however the food associated with anaphylaxis was not identified [23].
Finally, our study also shows that the food that was mostly related to anaphylaxis was nuts, which is different with the findings in the United States, where peanut was the food mainly related to this problem [24].
It is important to consider the possible limitations of the study. Our results are mainly extrapolated to university student's aged 18 to 25, however, they come from a public university that receives students from all economic strata. Although the sample size was adequate to quantify the prevalence of food allergy, it was not possible to carry out a strictly probabilistic sampling. This could led to skew of students in a particular career, as well as possibly to those subjects who had problems with food intake. A further limitation was the inability to confirm the diagnosis of food allergy through oral challenge tests or allergic sensitization. Finally, since we do not have data on the global prevalence of anaphylaxis in our country, we are unable to determine the accuracy of these estimates.
In summary, this study documents the prevalence of food allergy to certain nuts and seeds, and seafood rarely addressed in previous studies in our country. Particularly it exposes the serious problem of under diagnosis of food-related anaphylaxis in the young adult population, an entity with potential deadly consequences. More studies are necessary to clarify the true dimension of this problem.
 XML Download
XML Download