

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Plastic bronchitis has previously been referred to as fibrinous bronchitis, cast bronchitis, Hoffman bronchitis, and pseudomembranous bronchitis. The main pathogenesis of this disease is the presence of obstructive mucus plugs in the bronchus that do not resolve by themselves. In plastic bronchitis, mucus plugs interfere with air flow and block the bronchial tubes, inducing acute respiratory insufficiency. This condition was first identified as bronchial wrinkles by Galen in the 2nd century. The first case of plastic bronchitis in published literature was described in an autopsy report of a person who died of pneumonia or croup in 1899.12) Plastic bronchitis can be caused by several factors, such as congenital heart disease, allergy, sickle cell disease, and cystic fibrosis. It has also been reported in infectious diseases such as influenza virus in children.3) Pathologically, it is divided into type I and type II, depending on the presence or absence of inflammatory cells, and can be classified based on the underlying diseases. Type I is known as the inflammatory type. Type I bronchial casts are formed when there is an inflammatory response, infectious disease, and allergic reaction. On the other hand, type II bronchial casts have mucinous components. Type II plastic bronchitis is usually observed in patients with underlying cardiac diseases.4) Plastic bronchitis is a very rare disease, with fewer than 1,000 cases reported worldwide so far, and therefore, the prevalence of this disease according to age is unknown. It is known to predominantly occur in women, but the cause of this female predominance is not known.5)
CASE
A 6-year-old boy visited emergency room of Seoul National University Children's Hospital during winter, complaining of respiratory difficulty. When he was an infant, he developed macrocytic hypochromic anemia. At that time, it was suspected that the anemia was due to a drug allergy. We tried to determine the cause of the patient's anemia but found no apparent cause, and the anemia spontaneously recovered. He subsequently suffered from atopic dermatitis and egg allergy, but he was lost to follow-up.
Three days before visiting the emergency room, the patient had a cough with sputum and a body temperature of 37.8°C. Within a day, his symptoms aggravated and he had difficulty in breathing. He was unable to sleep because of the cough. His parents also recently had a respiratory infection. When he arrived at the emergency room, the pulse oximetry was 68%. His blood pressure was 108/67 mmHg, pulse rate was 154 beats/min, respiratory rate was 52 breaths/min, and the body temperature was 37.4°C. Crackles and wheezing were audible in both lung fields. The lung sound of the right lung was weaker than that of the left lung.
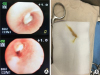
Oxygen (15 L/min) was supplied via a facial mask with a reservoir bag, but the oxygen saturation did not rise above 70%. The white blood cell count was 32,280 cells/μL, of which 89.1% were segmented neutrophils and 4.5% were lymphocytes. Hemoglobin level was 12.4 g/dL. The platelet count was 526,000/μL. The level of C-reactive protein in blood was 3.16 mg/dL. His arterial blood gas analysis revealed that blood pH was 7.14; pCO2 was 63 mmHg, pO2 was 46 mmHg; and oxygen index was 35. Endotracheal intubation was performed immediately, and he was transferred to the pediatric emergency intensive care unit. The initial chest radiograph showed that the patient's right lung was totally collapsed (Fig. 1A). Endotracheal tube adjustment and massive pulmonary physiotherapy were performed. The mechanical ventilator was adjusted to a higher setting which included an FiO2 of 1.0, and empirical antibiotics (piperacillin/tazobactam, vancomycin) were administered. Oseltamivir was also administered because the patient fell ill during the flu epidemic season. Inhalation of nitric oxide was started. However, respiratory acidosis, hypercapnia, and hypoxemia remained persistent, with the arterial blood gas analysis showing that the blood pH was 7.09, pCO2 was 86 mmHg, pO2 was 45 mmHg, and oxygenation index was 40. Thus, we performed veno-venous (from the right femoral to the right internal jugular vein) extracorporeal membrane oxygenation (VV ECMO) within 9 hours of the patient's emergency room arrival. Three hours after ECMO insertion, we performed flexible bronchoscopy. We found that thick mucus plugs were obstructing the right bronchus intermedius and upper lobe orifice (Fig. 2). After removal of the thick mucus plugs, the right lung could be ventilated, and the tracheal deviation decreased, as observed using a chest radiograph (Fig. 1B). The endotracheal aspiration samples tested negative on the flu rapid antigen test and the respiratory syncytial virus rapid antigen test. However, real-time multiplex polymerase chain reaction (PCR) detected the presence of influenza A virus in the endotracheal aspiration. There was no bacterial growth in blood, endotracheal and bronchoalveolar lavage cultures. The Mycoplasma pneumonia antibody titer was 1:640, but PCR did not detect the presence of M. pneumonia in endotracheal aspiration and bronchoalveolar lavage fluid. After 4 days, we could decrease the FiO2 to 0.3 on the ventilator settings, and the oxygenation index was lower than 10 (Fig. 3). We performed washing via bronchoscopy 2 more times due to persistent right upper lobe atelectasis. We stopped the VV ECMO on hospital day 6. The patient could breathe without a ventilator on hospital day 11, and was discharged without any sequelae on hospital day 19. After discharge, he was able to breathe normally and is currently undergoing regular follow-up.
 | Fig. 1(A) Initial status of plastic bronchitis; initial chest radiograph showed that the 6-year-old patient's right lung was totally collapsed. (B) Status of plastic bronchitis after bronchoalveolar lavage; after removal of the thick mucus plugs, the right lung could be ventilated, and the tracheal deviation decreased. Infiltration of the left lower lung was present.
|

DISCUSSION
Usual symptoms of plastic bronchitis are dyspnea, cough, fever, chest pain, and hemoptysis, and these symptoms may not be distinguishable from those of other diseases, such as pneumonia, status asthmaticus, or foreign body aspiration.6) On imaging, routine chest radiographs of patients with plastic bronchitis can show atelectasis or compensatory hyperinflation. Pneumomediastinum and emphysema are common to radiographic findings for this group of diseases. Urgent bronchoscopy is very important for the diagnosis and treatment of plastic bronchitis because it cannot be easily distinguished from other diseases. Ultimately, urgent removal of the mucus plugs using bronchoscopy is crucial, but it should be performed while providing a supplement of oxygenation. This is to avoid the risk of hypoxic ischemic encephalopathy due to the hypoxemia before and after the procedure. In order to prevent hypoxic damage, we perform ECMO on patients before the bronchoscopy procedure.7)
Most influenza infections in children improve spontaneously over time, but in some patients, they lead to neurological or pulmonary sequelae because of severe pneumonia or encephalitis.8) Recently, several papers on influenza and plastic bronchitis in children have been published.91011) In particular, a paper from a single center in China reported that 2 out of 14 patients died from hypoxia due to plastic bronchitis and multiple organ failure associated with it between 2009 and 2014.11) In another study, influenza B, which is known to be more infectious than influenza A, was reported to cause plastic bronchitis.10)
The patient described in the present case report was not diagnosed with asthma but had allergic diseases, such as atopic dermatitis and recurrent urticaria. It is possible that the patient's susceptibility to allergies influenced the development of plastic bronchitis. Several plastic bronchitis cases are associated with asthma; however, there is controversy about the inclusion of plastic bronchitis in the asthma spectrum and severe asthma or secretory hyper-responsiveness.12)
In the present case, immediate respiratory support was achieved, and emergent bronchoscopy enabled early discharge without sequelae. The most important treatment for plastic bronchitis is to remove the plugs using bronchoscopy. Rigid bronchoscopy is needed if the plugs cannot be removed by flexible bronchoscopy.13) In some cases, the treatment of an underlying disease that can cause plastic bronchitis is important. If there is a problem in the circulation of the lymphatics, interventions, such as embolization or duct ligation may be required.1415) Viral infection is often associated with plastic bronchitis, and therefore antiviral agents can be helpful, such as in our case. Although the association between bacterial infection and plastic bronchitis is low, there are reports that plastic bronchitis can cause a tracheoesophageal fistula.16) In such cases, appropriate antimicrobial agents that the bacteria are susceptible to should be administered. Supportive care, including inhaled steroids, bronchodilators, mucolytics, inhaled heparin or tissue plasminogen activator, and dornase alfa may also be used, but their effectiveness are unclear.3) Consequently, we think that removing the mucus plugs emergently and preventing the worsening of hypoxemia during the procedure can improve the prognosis of patients with plastic bronchitis.
 XML Download
XML Download