

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Volumetric changes in the alveolar ridge after tooth extraction have been discussed in the literature. Alveolar ridge resorption was found to be significantly greater on the buccal side than on the lingual side [12]. In an experimental animal study, Araújo and Lindhe [3] reported that the buccal bone wall was composed of bundle bone. According to the bundle bone theory, bundle bone loses its function after extraction and is resorbed by osteoclasts. In addition, buccal bone is thinner than lingual or palatal bone. Therefore, the thin buccal plate can be traumatized during the extraction procedure. Some authors have studied resorption patterns after extraction. Schropp et al. [4] reported that the width of the residual ridge decreased by up to 50%, and that two-thirds of the bone resorption occurred within the first 3 months.
Ridge preservation using biomaterials with or without a barrier membrane has been shown to reduce bone resorption in comparison to not using biomaterials [56]. Various techniques have been suggested to minimize ridge resorption. In a systematic review, Vignoletti et al. [7] reported that the scientific evidence does not provide clear guidelines regarding the type of biomaterial. Some randomized controlled clinical trials have been reported on volumetric changes of soft tissue after extraction using different techniques for ridge preservation. Jung et al. [8] reported that the application of demineralized bovine bone mineral with 10% collagen at the bone level and the application of a collagen matrix or an autogenous soft tissue punch graft at the soft tissue level resulted in smaller vertical and horizontal changes in the alveolar ridge than was observed after spontaneous healing in a radiographic analysis. Schneider et al. [9] also reported similar results using cast models.
The regenerative process begins with the migration of cells from the blood vessels, and the occurrence of angiogenesis in an extraction socket is also a prerequisite for successful ridge preservation. Rapid angiogenesis may provide a shortened healing time and promising results. Fibroblast growth factor-2 (FGF-2) is a multifunctional growth factor that plays an important role in the induction of proliferation and morphogenesis in various types of cells, including periodontal ligament cells [10]. FGF-2 has been reported to have osteogenic and angiogenic effects [1112].
The selection of a suitable carrier matrix is one of the most important issues for growth factor application. The carrier matrix should release growth factors properly and function as a scaffold. Collagenated biphasic calcium phosphate (BCP) has an osteoconductive effect and can be used to deliver growth factors for bone regeneration [13]. BCP is composed of slowly resorbing hydroxyapatite and rapidly resorbing tricalcium phosphate. Compared to absorbable collagen sponges, BCP has better performance for some properties, such as dimensional stability, but its degradation properties and release characteristics have not been well established [1415]. The collagen matrix stabilizes the bone particles and helps with the absorption of blood coagulum in the initial stage of healing. Composite bone particle and collagen grafts are highly hemostatic, can to expand to fill defects, and stay retained when placed into an extraction socket [16].
The aim of this study was to evaluate volumetric and histologic changes in edentulous alveolar ridge areas after ridge preservation using basic fibroblast growth factor-2 (bFGF-2) in combination with collagenated BCP.
MATERIALS AND METHODS
Surgical procedure
The experiments were performed in 6 adult male beagle dogs weighing 10–12 kg. The maxillary second premolars and third premolars were extracted. A total of 24 extraction sockets were involved in this experiment. There were 3 groups: an experimental group, a positive control group, and a negative control group. In the experimental group, a collagenated BCP block (Osteon II collagen, Genoss, Suwon, Korea) was soaked in 0.6 μg/mL of bFGF-2 (Genoss) for 10 minutes and placed in the extraction socket. The graft was covered with a collagen matrix (Mucograft, Geistlich, Wolhusen, Switzerland). In the positive control group, the extraction sockets were filled with the BCP blocks without bFGF-2. In the negative control group, no biomaterial was placed in the fresh extraction socket (Table 1). This protocol was approved by the Seoul National University Institutional Animal Care and Use Committee at Seoul National University, Seoul, Republic of Korea (SNU-130806-4-1).
Volumetric changes
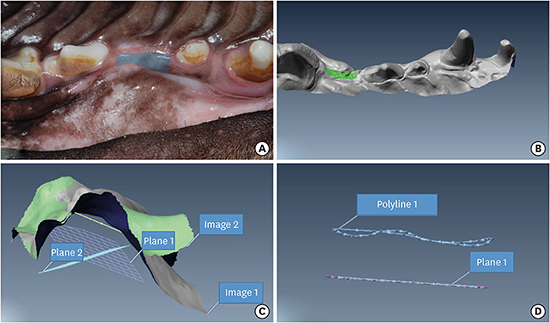
Impressions were taken using pre-fabricated individual trays at 2-, 4-, and 12-weeks after the surgical intervention (Figure 1). An optical scanner (DScan version 1.1, E.G.S solution, Lazzaro, Italy) was used to scan the casts. Scans of the 2-week casts were matched with the corresponding scans of casts at 4 weeks and 12 weeks using digital imaging software (Polyworks®; Innovmetric, Quebec, Canada). While superimposing the different scans, the adjacent teeth were used as reference points to ensure precise alignment. A region of interest (ROI) was established in the scan of the 2-week cast. The average surface vector was calculated for the ROI. Then, this ROI was projected onto a plane perpendicular to the average surface vector. This area was then projected onto the scans of the 4-week and 12-week casts (Figure 2). The volumetric change was divided by the area of the projection and interpreted as describing the amount of displacement between the surfaces.
 | Figure 1Surgical procedure. Six beagle dogs and 24 extraction sockets were involved. The maxillary second premolars and third premolars were extracted. Twelve teeth were extracted at the first intervention and other 12 teeth were extracted at the second intervention. Impressions were taken at 2-, 4-, and 12-weeks after surgery. The dogs were sacrificed 12 weeks after the first intervention.
|

Histologic evaluation
The block specimens were fixed in formalin solution. The slides were sectioned in the buccopalatal plane and stained with hematoxylin and eosin. Two specimens were obtained from each extraction socket. Histological observations were made using light microscopy (BX50, Olympus, Tokyo, Japan). The ROI was set to the coronal portion of the socket after general observations with low magnification (Figure 3).
RESULTS
Volumetric changes
Swelling was observed in the experimental group until 2 weeks. Between 2 and 4 weeks after surgery, the volumetric changes in the experimental group were larger than those of the positive and negative control groups. In the experimental group, however, the volumetric changes between 4 and 12 weeks were smaller than those in the other groups. This difference did not reach statistical significance (Table 2).
Table 2
Volumetric changes of extraction sockets (mm, n=4)

Values are presented as mean (standard deviation).
h2wks: height of residual bone 2 weeks after surgery, h4wks: height of residual bone 4 weeks after surgery, h12wks: height of residual bone 12 weeks after surgery.
![]()
Histologic evaluation
The extraction sockets of all groups healed well, without any inflammatory cell infiltration.
Four weeks after the extraction, the negative control group exhibited small areas of woven bone formation (Figure 4A). A large portion of the socket was composed of fibrous connective tissue. Fibroblasts were the most common cell in this group. There were some osteoblasts and endothelial cells, and bone formation was apparent. Woven bone formed and was lined by osteoblasts and fibroblasts in the positive control group (Figure 4B). Residual BCP granules were observed and some osteoclasts were identified near graft particles. In the experimental group, there were more osteoclasts surrounding the materials than in the positive control group (Figure 4C). There was distinct resorption of residual graft particles and collagen fibers that were parts of the collagenated BCP. However, osteoblasts and fibroblasts were also observed, and some formation of woven bone from the existing bone took place where enhanced angiogenesis was observed.
 | Figure 4Histologic evaluation. (A) Negative control, 4 weeks: a large portion of the socket was composed of fibrous connective tissue. (B) Positive control, 4 weeks: woven bone had formed and was lined by osteoblasts. Some osteoclasts were identified near graft particles. (C) Experimental group, 4 weeks: there was distinct resorption of residual graft particles. Woven bone from the existing bone was formed where enhanced angiogenesis was observed. (D) Negative control, 12 weeks: a limited amount of new bone was observed. The woven bone was lined by inactive and flat osteoblasts. (E) Positive control, 12 weeks: osteocytes were found in the newly formed bone and bone maturation had progressed. (F) Experimental group, 12 weeks: new bone formation and angiogenesis were evident. More mature bone and faster healing were found (A–F: bar=100 μm). Arrowheads, arrow, and asterisk indicate osteoclasts, osteoblasts, and vessels, respectively.
|
In the negative control group at 12 weeks, a limited amount of new bone was observed, and woven bone was lined by inactive and flat osteoblasts. Adipocyte-like cells were observed in the soft tissue between the bone matrix, but few osteoclasts were evident. This means that bone remodeling was not active in the negative control group (Figure 4D). In the positive control group at 12 weeks, there remained grafted particles similar to those observed at 4 weeks (Figure 4E). However, osteocytes were found in newly formed bone, and bone maturation had progressed compared to the observations made at 4 weeks. New bone formation and angiogenesis were evident in the experimental group (Figure 4F). Remnants of graft particles were also observed in the experimental group, but the amount of graft material was less than in the positive control group. The bone trabeculae coalesced with each other, indicating the maturation of newly formed bone. Blood vessels were observed and were surrounded by new bone. Generally, more mature bone and faster healing were found in this group.
DISCUSSION
The aim of this study was to evaluate the alveolar ridge after ridge preservation using bFGF-2 in combination with collagenated BCP. It is notable that the volumetric changes in the experimental group were larger than those of the positive and negative control groups between 2 and 4 weeks. Swelling of the soft tissue was observed in the experimental group at 2 weeks. This swelling may be explained as the result of the angiogenic effects of bFGF-2. These results are consistent with those of Lu et al. [15], who reported considerable initial swelling in their study of BMP-2 loaded absorbable collagen sponges and collagenated BCP on supra-alveolar peri-implant defects. Kodama et al. [17] found many blood vessels in the bone defects at sites treated with FGF-2 during the early healing period. No inflammatory cell infiltration was observed, and blood vessels were evident.
The regenerative process begins with the migration of cells from the vascular spaces. Vascular systems also supply oxygen and nutrients. Angiogenesis is essential for successful bone induction during osteogenesis [18]. Some previous studies have been reported that FGF-2 had osteogenic and angiogenic effects [1112]. In a beagle dog study, FGF-2 promoted angiogenesis and the proliferation of fibroblastic cells in the early regenerative phase [7].
Collagenated BCP was used in this study. Clinical manageability was improved by adding collagen to BCP, in contrast to particle-type carriers, which have some limitations such as space maintenance and application to various defects. When the carrier matrix is loaded with growth factor, it should release growth factors properly. Unlike absorbable collagen sponges, the sustained release of growth factor is possible with collagenated BCP [13]. After the initial swelling subsided, the magnitude of the volumetric changes in the experimental group and positive control group was smaller than in the negative control group. This result indicates the ridge preservation effect of collagenated BCP with or without bFGF-2.
In this study, distinct resorption of residual bone and collagen fibers was noted at 4 weeks in the experimental group, as well as more mature bone and faster healing at 12 weeks. Rapid angiogenesis induced by bFGF-2 may have contributed to these promising results, indicating an enhanced healing process in the extraction sockets. Based on the findings of the present study, bFGF-2 may be considered for use as a therapeutic molecule in ridge preservation procedures.
 XML Download
XML Download