

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A variety of modalities can be used as treatment options for periodontal bone defects. Among those modalities, guided tissue regeneration (GTR) and guided bone regeneration (GBR) have been established as reliable procedures when applied in the vicinity of teeth and implants. Conceptually, GTR prevents the downward growth of epithelial tissue and creates a space that recruits osteogenic cells from the periodontal ligament and surrounding bone [123].
The function of the barrier membrane allows this mechanism to be implemented, and several properties are required for a barrier membrane to be used for reconstructive purposes. The barrier membrane should have excellent biocompatibility, the ability to block unwanted cells, and be easy to manipulate [4]. In the past, nonabsorbable membranes have been extensively used, but the trend has shifted to the use of absorbable membranes due to the risk of exposure and infection posed by nonabsorbable membranes and the need for surgical removal. However, since absorbable membranes are not rigid, they can easily collapse into defects that are not completely containable [5].
Space provision has been suggested to be a crucial factor for predicting regenerative outcomes [6], and superior results have been reported using therapies combining bone substitute materials and absorbable membranes [78]. Bone graft materials support the membrane by helping to retain the desired volume and to promote osteoconductive properties [3]. Among the several bone graft materials commercially available, a collagenated xenogeneic block-type bone substitute has recently been introduced and can be useful for non-containable defects such as dehiscence and 1- or 2-wall defects [91011].
Many different types of absorbent membranes, both natural and synthetic, have been developed, but membranes made from collagen are the most frequently used [212]. A common method of production is to extract collagen from a xenogeneic species and add a cross-linking agent to regulate the degradation time [13]. However, the application of cross-linking agents is associated with foreign body reactions, inflammation, decreased integration, and decreased vascularization [314]. A novel natural extracellular matrix (ECM) membrane (NEM; Lyso-Gide, Oscotec Inc., Seongnam, Korea) has been developed to minimize these problems. This membrane originates from the porcine pericardium and is composed of 2 layers, which is an advantage for barrier membrane function. The upper layer is very thin (<0.1 mm) and dense in order to prevent apical tissue penetration. The lower layer (<0.2 mm) is a micropore structure for positioning bone-forming cells. The degradation products are mainly collagen type I and hydroxyproline. This ECM-based membrane can be maintained for up to 3 months without a cross-linking agent [13].
The purpose of this study was to investigate the feasibility of regenerative therapy using a collagenated bone graft and absorbable membrane for intrabony defects. We compared the effects of the NEM to the effects of using a widely used ECM membrane (WEM; Bio-Gide, Geistlich Biomaterials, Wolhusen, Switzerland). We compared the membranes both clinically and radiologically in reconstructive bone graft procedures applied to bone defects around the teeth and implants.
MATERIALS AND METHODS
Study design
This study was a prospective, double-blinded, randomized controlled clinical trial. According to a parallel group design, bone defects were filled with deproteinized bovine bone mineral collagen (Bio-Oss Collagen, Geistlich Biomaterials) and randomly assigned to either the Lyso-Gide or Bio-Gide membrane patient groups. The protocol was approved by the Research Ethics Committee of the Seoul National University Dental Hospital (approval No. CGE14002) and registered as a clinical trial (http://cris.nih.go.kr, approval No. KCT0001814). All procedures were performed in compliance with the Declaration of Helsinki and the Consolidated Standards of Reporting Trials (CONSORT) 2010 statements. All participants received detailed descriptions of the study and provided written informed consent prior to the intervention.
Study population and randomization
Fifty-nine participants were recruited from June 2014 to April 2016 from a pool of patients undergoing treatment at either the Department of Periodontology or the Department of Oral and Maxillofacial Surgery at the Seoul National University Dental Hospital in Seoul, Korea.
The inclusion criteria were that the patients needed to be adults over 20 years of age with the presence of bone defects around their natural teeth or implants due to periodontal disease in the maxilla or mandible. The exclusion criteria were as follows: 1) the presence of acute infection; 2) the need for tooth extraction due to extensive bone loss; 3) pregnancy; 4) uncontrolled hypertension or diabetes; 5) a history of malignant tumors or mental illness; 6) serious cardiovascular, respiratory, kidney, liver, digestive, hematologic, or neurological disease; 7) hyperthyroidism or hypothyroidism; 8) history of a drug allergy; 9) severe depression or anxiety disorder; or 10) alcohol abuse within the previous year.
The test and control groups were allocated at a ratio of 1:1 using a pre-generated randomization table and each subject was assigned an identification code. The subjects, clinicians, and investigators were not informed of the assigned group.
Ten participants were excluded after screening, and 49 subjects were enrolled and randomly assigned to the control (n=24) or test group (n=25). Three patients dropped out due to withdrawal of consent. We performed procedures and analyzed their results in a total of 46 subjects (control group, n=22; test group, n=24) (Figure 1). The general characteristics of the subjects are shown in Table 1.
 | Figure 1Flow diagram for the phases of the randomized controlled trial.
CBCT: cone-beam computed tomography, VAS: visual analog scale.
|
Table 1
General characteristics of the subjects
![]()
Surgical procedures and postoperative care
After more than 10 hours of training to ensure technical reproducibility, 4 skilled periodontists performed all the regeneration procedures. The surgical sites were treated under local anesthesia (2% lidocaine with 1:100,000 epinephrine). Intrasulcular incisions were made and full-thickness flaps were elevated. Thorough curettage of granulation tissue was conducted and deproteinized bovine bone mineral collagen (Bio-Oss Collagen, Geistlich Biomaterials) was used to fill the defects. The NEM and the WEM were trimmed and applied to the test and control groups, respectively. Antibiotics, analgesics, and mouthwash were prescribed for 5 to 7 days. At 7 to 10 days postoperatively, the sutures were removed and any adverse events were evaluated. Patients were instructed on oral hygiene maintenance and received professional prophylaxis as needed.
Evaluation of dimensional changes
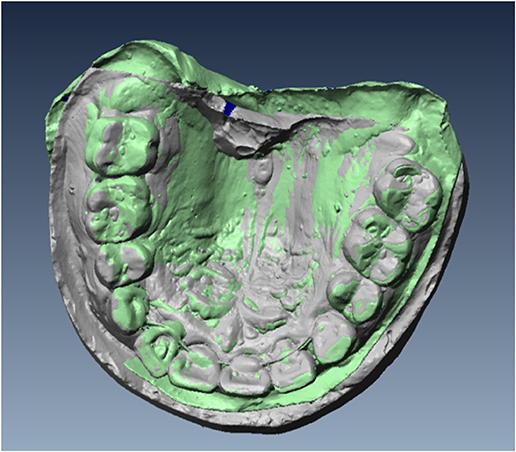
At 1 week and 6 months postoperatively, alginate impressions were taken and plaster models were made with dental stone (GC Fujirock EP, GC Corp., Tokyo, Japan). The models were computationally imaged using an optical scanner (DScan version 1.1, E.G.S solution, Lazzaro, Italy) and DentalCAD software (E.G.S solution). The 1-week and 6-month models of each patient were superimposed using software (Polyworks, Innovmetric, Quebec City, Canada), with the adjacent teeth used as the reference point (Figure 2).
A region of interest (ROI) was set in the image of the 1-week model and the average surface vector was calculated. The ROI was then scanned perpendicularly to the average surface vector and the volume was measured. The 6-month model was measured in the same manner. Dimensional changes were evaluated by dividing the difference between the volumes measured in the 2 models by the surface vector.
Quantity of bone tissue
Cone-beam computed tomography (CBCT) (Dinnova 3, HDX Corp., Seoul, Korea) images were obtained (with a scan time of 7 seconds at 120 kV and 10 mA) immediately after and 6 months after the surgical procedure.
The unprocessed CBCT images were merged and re-sliced at a resolution of 0.1 mm using OnDemand3D software (Cybermed Inc., Daejeon, Korea). Three-dimensional reconstructed images were centered on the bone defect and segmented, and the images on the day of surgery and 6 months postoperatively were set in the same range. The amount of change was assessed by the volume ratio of the segmented regions between the 2 different time points.
Width and height
In the axial and sagittal directions, the initial width and height of the intrabony defect on the day of surgery were compared to the residual defect below the grafted bone substitutes after 6 months, using CBCT imaging and OnDemand3D software (Figure 3).
 | Figure 3Sagittal CBCT images of the mesial intrabony defect of the upper left canine tooth obtained immediately after the operation and 6 months postoperatively. The filled bone substitutes can be observed on the CBCT image taken immediately after the operation, and were well integrated with the surrounding bone tissue at 6 months. (A) CBCT image obtained on the day of surgery. (B) CBCT image obtained 6 months after the operation.
CBCT: cone-beam computed tomography.
|
Data analysis
The sample size was calculated in order to provide 80% power to recognize a significant difference of 6 mm3 between groups, with a 95% confidence interval and a standard deviation of 7.68. A power analysis demonstrated that 21 subjects per group were required, and P values <0.05 were considered to indicate statistical significance.
The primary endpoint was the quantity of bone tissue in the intrabony defect measured by CBCT. The dimensional changes of the impression model and the changes in the width and height of the defects below the grafted bone substitutes were the secondary endpoints.
The Shapiro-Wilk test was applied to assess the normality of the distributions of each parameter. The nonparametric Mann-Whitney U test was used to compare the differences in dimensional change, quantity of bone tissue, and the width and height of the defect between the test and control group. The independent t-test was applied to assess the differences in age between the test and control group. The Pearson χ2 test was performed to compare the proportions of gender, jaw positions, and right/left locations in the jaw between the test and control group. The impression data for dimensional changes in 4 subjects were lost and the mean imputation method was applied. SPSS version 23.0 (SPSS Inc., Armonk, NY, USA) was used for analysis.
RESULTS
Evaluation of dimensional changes
The dimensional changes are shown in Table 2. The magnitude of the changes was −0.8 mm3/mm2 and −0.6 mm3/mm2 in the test and control groups, respectively. The difference between the groups was not statistically significant (P≥0.05).
Table 2
Clinical and radiographic dimensional changes

![]()
Quantity of bone tissue on CBCT
The volumes measured in the same region around the grafted area on the day of surgery and 6 months postoperatively are shown in Table 2. The calculated percent change was 102.8% in the test group and 100.7% in the control group. The difference between the groups was not significant (P≥0.05).
Changes in width and height on CBCT
The width and height results of the defects measured by CBCT on the day of surgery and 6 months later are shown in Table 2. Initially, both the width and height of the defects were similar between the 2 groups (P≥0.05). The decrease in width was 1.5 mm and 1.4 mm in the test and control groups, respectively, and the difference between the 2 groups was not statistically significant (P≥0.05). The height decreased by 1.3 mm and 1.3 mm in the test and control groups, respectively, and the difference between the 2 groups was not statistically significant (P≥0.05).
DISCUSSION
The present study demonstrated the effectiveness of reconstructive procedures in combination with collagenated xenogeneic bone substitutes and a barrier membrane. In addition, the efficacy of the newly developed membrane when applied to intrabony defects around teeth and implants affected by periodontal disease was evaluated clinically and radiologically.
CBCT analysis provided measurements in 3 dimensions and confirmed the regenerative outcomes. Previous studies have mainly used 2-dimensional images from periapical radiographs and evaluated changes in intrabony defects by clinically measuring the probing depth and the attachment level [15]. CBCT can be used to observe the whole area, including buccal and lingual surfaces, which can be masked in 2-dimensional images. CBCT is a non-destructive method that can verify the surgical site 3-dimensionally without re-entry. Moreover, CBCT has the advantage of providing high-quality images with a lower radiation dose than CT [1617].
The bone mineral quantity as measured by CBCT slightly increased in both groups at 6 months postoperatively, with no statistically significant difference between the 2 groups. This observation indicates that the bone graft materials covered by barrier membranes were well maintained and exhibited osteoconductive properties. The collagenated xenogeneic bone substitutes used in this experiment were expected to remain longer, even in the defects that were not completely containable, because the substitutes were block-type, rather than granule-type. Furthermore, since the membranes were used in combination, the bone grafts could maintain stable enough to be well integrated into the pristine bone. This helped to sustain the provision of adequate space and contributed to a favorable regenerative outcome [5]. There has been little human clinical research on GTR or GBR using collagenated xenogeneic bone, and it is difficult to compare results directly due to the heterogeneous measurement methods. However, previous studies have all showed good regenerative outcomes [9101118].
The width and the height of the bone defects below the grafted bone substitutes also decreased in both the test and control groups at 6 months postoperatively. The extent of reduction was not statistically significantly different between the 2 groups. It can be assumed that the filled bone substitute material was absorbed at the base of the defect and that new hard tissue formed. The regenerated tissue provided normal bone structure in the cortical and trabecular layers, which corresponded to the histological and radiographic results described in previous reports. According to the histologic evidence, the graft particles were embedded between the new bone tissues. This was due to the slow reabsorption rate, the encapsulation of the particles in more connective tissue in the coronal portion, and the presence of fewer bony walls in the defects [9101718].
One of the more notable results is that the dimensions in the impression model, including the soft tissues, were reduced in both groups at 6 months postoperatively, whereas the bone quantities measured on CBCT slightly increased. A careful interpretation of this finding would suggest that the prominent postoperative edema and wound dehiscence 1 week after surgery may have contributed to larger dimensions compared to the fully healed state after 6 months. This conclusion is supported by a previous study on postoperative morbidity after regenerative surgery on intrabony defects, which reported discomfort from edema and wound dehiscence at 1 week and a rapid decrease in discomfort thereafter [19].
According to the present data, the 2 membranes used in the test and control groups demonstrated similar efficacy in GTR and GBR procedures. This corroborates data from a previous study of our group in which ridge preservation in extraction sockets was performed using NEM and WEM [20]. NEM is comparable to the most commonly used membrane (WEM), and has the advantage of being inexpensive and not requiring a cross-linking agent. Clinicians were asked on a questionnaire about the operability of the membrane during surgery. These data were not analyzed in the present study, but NEM showed better results for all questions regarding the ease of adaptation and trimming and tear resistance.
In conclusion, the combined use of a collagenated bone graft and an absorbable membrane in intrabony defects is a reliable and predictable regenerative therapy around the teeth and implants. In addition, the 2 resorbable ECM membranes showed similar regenerative outcomes in terms of clinical and radiographic results.
 XML Download
XML Download