

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Various periodontal procedures, including resective and/or regenerative therapy, are utilized for the treatment of periodontal defects in patients with severe periodontitis. Furcation involvement in the molars is particularly difficult to treat, because of the complex root anatomy and the degree of bone loss [12]. Anatomical features such as cervical enamel projections, bifurcation ridges, and root concavities can be risk factors for bacterial invasion to aggravate furcation involvement [345]. Consequently, furcal bone defects can develop locally in furcation regions, resulting in severe class III furcation defects. Although periodontal regenerative therapies, including guided tissue regeneration and various bone grafts, have been applied to furcation defects, the effects of these treatments are limited, especially when the vertical opening of the class III furcation defects is larger than 3 mm [6789]. Therefore, resective therapy or tooth extraction may be a practical option for class III furcation defects, even if adjacent bone still exists. However, new biological and regenerative approaches are anticipated to overcome these anatomical problems and to promote clinical reduction and bone filling.
Autologous tooth transplantation is the repositioning of a tooth from one site to another in the same individual. It was first clearly documented in 1956 by Hale [10]. The principle of surgical intervention is still followed and autologous tooth transplantation is a practicable treatment for tooth loss. Currently, dental implants are considered to be a major tooth replacement option in oral rehabilitation. However, complications including surgical accidents, peri-implantitis, and fractures of implant-supported prostheses are increasing [1112]. In contrast, autologous tooth transplantation has been reported as a conservative approach with high success rates (74%–100%) [13141516] for the improvement of esthetics and masticatory function in carefully selected patients. Thus, autologous tooth transplantation can still be considered an alternative biological treatment that has the advantage of autogenous tissue (i.e., periodontal ligament [PDL] and root cementum) grafting without immunological rejection. The PDL contains undifferentiated mesenchymal cells, and has homeostatic and reparative functions that play a crucial role in autologous tooth transplantation/replantation and favorable periodontal wound healing [171819]. Furthermore, several studies have shown that healthy PDL on the root surface of the extracted tooth induced bone formation in various ectopic positions, as well as in alveolar bone defects [202122].
In this study, reciprocal autologous root transplantation was performed, in which mesial and distal extracted roots were replaced with intact PDL facing class III furcation defects to accelerate bone/periodontal regeneration. Thus, the purpose of this pilot study was to investigate the effect of reciprocal autologous root transplantation on periodontal wound healing/regeneration in class III furcation defects in dogs.
MATERIALS AND METHODS
Animals
The unilateral mandibular third and fourth premolars of four 11- to 15-month-old healthy male beagle dogs weighing 10.3 to 12.3 kg were used in this study. The procedures and protocol design described here were approved by the Ethical Committee of the Animal Research Center of Kagoshima University, Japan (MD13152).
Surgical protocol
One surgeon (N.T.) performed all surgical procedures under general and local anesthesia using aseptic protocols. General anesthesia was achieved using sodium pentobarbital (0.4 mL/kg intravenously; Somunopenchiru, Kyoritsu Seiyaku, Tokyo, Japan), maintaining spontaneous breathing. Local anesthesia was performed using lidocaine HCl/epinephrine (2%, 1:80,000; Xylocaine, Fresenius Kabi USA, LLC., Lake Zurich, IL). Root canal treatment, including pulp extirpation and root canal filling, was necessary in the unilateral third and fourth premolars prior to root separation. Subsequently, the resin core was built up using a screw pin for each root canal. After 2 weeks, the mesiodistal root separation of the premolars and class III furcation defects was performed. Briefly, intrasulcular incisions were made from the mesial aspect of the second premolar to the distal aspect of the first molar, and full-thickness flaps were elevated at the buccal and lingual aspects. Following root separation of the unilateral third and fourth premolars, furcation defects (7 mm wide and 6 mm high) were created by bone chisel and fissure burs with sterile saline coolant (Figure 1A-C). The root surfaces adjacent to the defects were planed with Gracey curettes to remove the cementum and PDL. Reference notches were made on the root surfaces at the deepest point of the defects, and at the cementoenamel junction (CEJ) using a #1 round bur. The class III furcation defects (8 defects) in the third and fourth premolars were randomized to receive either reciprocal autologous root transplantation (test) or no further treatment (control) (4 sites/group) (Table 1). In the test group, the separated roots were carefully dislocated with an elevator, maintaining an intact PDL, and extracted with forceps (Figure 1D). The extracted roots were immersed in sterile saline immediately, and remained in sterile saline until transplantation [232425]. The recipient sites were prepared by using fissure burs with sufficient saline irrigation, such that the CEJ of the roots was located at the same level as the proximal existing bone. Prior to transplantation of the roots, the crowns were trimmed to reduce mutual interference in the recipient sites. The mesial root was then transplanted to the distal extraction socket and the distal root was transplanted to the mesial socket in a manner such that root surfaces with intact PDL faced each other in the furcation area (Figure 1E). Following transplantation in the test group, the mucoperiosteal flaps were coronally repositioned and sutured with expanded polytetrafluoroethylene (ePTFE) sutures (Gore-Tex Suture CV-6, W. L. Gore and Associates, Inc., Flagstaff, AZ, USA). The transplanted roots were fixed with a ⌀0.9-mm cobalt-chromium wire (Technoflex, Rocky Mountain Morita Corporation, Tokyo, Japan) using dental adhesive resin cement (Super-Bond C&B, Sun Medical Co., Ltd., Shiga, Japan) (Figure 1F). In the control group, the flaps were coronally repositioned and sutured with ePTFE sutures, and the roots were fixed in the same manner as in the test group. All dogs received analgesics (buprenorphine HCl, 0.1 mL/kg intramuscularly; Lepetan, Otsuka Pharmaceutical, Co., Ltd., Tokyo, Japan) and antibiotics (procaine penicillin G and dihydrostreptomycin sulfate aqueous suspension for injection, 0.05 mL/kg intramuscularly; Mycillin Sol Meiji for Veterinary Use, Meiji Seika Pharma Co., Ltd., Tokyo, Japan) for 3 days after surgery.
Figure 1
Clinical overview of the surgical procedure. (A) Following root separation, a class III furcation defect was prepared. The root surface adjacent to the defect was planed with curettes to remove the cementum and PDL. (B and C) Reference notches were made on the root surfaces at the deepest point of the defects and at the CEJ. (D) The separated roots were extracted and the sockets were prepared. (E) The mesial root was transplanted to the distal extraction socket and the distal root was transplanted to the mesial socket in the same direction. (F) After the mucoperiosteal flap was coronally repositioned and sutured, transplanted roots were fixed with cobalt-chromium wire by dental adhesive resin cement.
PDL: periodontal ligament, CEJ: cementoenamel junction.
Table 1
Experimental design scheme for 4 dogs

| Dogs | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Test | RP3 | LP3 | RP4 | LP4 |
| Control | RP4 | LP4 | RP3 | LP3 |
Following surgery, the dogs were fed only a water-softened diet. For plaque control, a 2% solution of chlorhexidine gluconate was applied 3 times a week throughout the healing period. The sutures were removed 2 weeks after the surgical procedure.
Histological processing
Ten weeks after surgery, the animals were euthanized by the induction of deep anesthesia with an overdose of sodium pentobarbital. All the defects were dissected along with the surrounding soft and hard tissues. The tissue blocks were fixed in 10% neutral buffered formalin, dehydrated in ethanol and acetone, and embedded in methyl methacrylate resin (Wako Pure Chemical, Osaka, Japan). Before trimming the resin blocks, micro-computed tomography was carried out to obtain optimal aspects of the sections. The resin blocks were sectioned mesiodistally with a diamond band saw (BS-300CP, Exakt Apparatebau, Norderstedt, Germany). Slides were ground and polished to a final thickness of approximately 50 µm using a microgrinding machine (MG4000, Exakt Apparatebau, Norderstedt, Germany) and stained with toluidine blue. For the histometric analysis, 2 sections were selected from the most central area of the bone defect, as identified by the apical notch (N1) and coronal notch (N2) on the root surface.
Histometric analysis
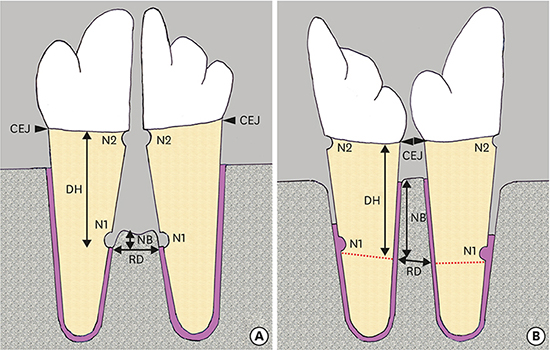
All specimens were analyzed histometrically under a light microscope (BX51, Olympus Optical Co., LTD., Tokyo, Japan) equipped with a computerized imaging system (Win Roof Version 6.0, Mitani Corporation, Fukui, Japan). The mean value of each histometric parameter was calculated for the mesiodistal side. The following parameters (Figure 2A and B) were measured by an experienced masked examiner (Y.S.): 1) defect height (DH): distance between the N1 and N2, 2) new bone formation (NB): distance between the apical extent of root planing and the coronal extent of newly formed bone along the mesial and distal root surfaces in the furcation defect, 3) root resorption (RR): the total extent of cavities in the root surface reaching to the cementum or dentin, 4) ankylosis (ANK): the total extent of the root surface fused to the bone, and 5) root distance (RD): the distance between the mesial and distal roots at the height of the N1. In the test (reciprocal autologous root transplantation) group, the base of the defect was indicated by the line extending from the N1 on the mesiodistal root surface parallel to the line linking the N2 to the opposite side of the CEJ (Figure 2B). The measurements, except for DH and RD, were also expressed as the percentage of the DH or the total length of the root surface in the furcation defects.
Figure 2
Schematic illustration of the landmarks used for histometric measurements in the (A) control (no treatment) and in the (B) test (reciprocal autologous root transplantation) group.
CEJ: cementoenamel junction, DH: defect height, N1: apical notch, N2: coronal notch, NB: new bone formation, RD: root distance.

Statistical analysis
The means and standard deviations of each parameter were calculated for each treatment group using the values obtained from the subject animals. Statistical differences were analyzed using the Mann-Whitney test. P values <0.05 were considered to indicate statistical significance. All calculations were performed using PASW Statistics 18 (SPSS Co. Ltd., Tokyo, Japan).
RESULTS
Clinical observations
Clinical healing after surgery was uneventful at all sites, with limited signs of inflammation throughout the experimental period.
Histologic observations
In the control group, new cementum and new bone were found to a limited extent in the apical portion of the defects (Figure 3A and B). The level of the alveolar bone crest was much lower than in the mesiodistal intact bone (Figure 3A). Extensive collapse of the flap and considerable apical migration of the junctional epithelium were observed in the class III furcation defects (Figure 3C). The collagen fibers appeared to be sparser than those observed in the test group (Figure 3B). There were no abnormal findings, such as bone resorption on the mesiodistal sides, cavities of deep RR, or ankyloses (Figure 3A). In the test group, newly formed bone extended close to the CEJ in the defect area between the transplanted roots (Figure 4A). The level of the newly formed bone crest was comparable to that of the existing bone on the mesiodistal sides (Figure 4A). Dense collagen fibers inserting into the residual cementum on the surfaces of the transplanted roots were observed (Figure 4B and C). ANK was observed in 2 specimens on the mesiodistal sides where the root-planed surfaces faced the existing bone (Figure 4D). RR was detected in both the control and test groups (Figures 3A and 4A).
Figure 3
Representative photomicrographs in the control group. (A) Overview of the class III furcation defects (scale bar=2 mm). (B) Higher magnification of the framed area in (A) (scale bar=100 μm). (C) Higher magnification of the framed area in (A) (scale bar=100 μm), toluidine blue staining.
N1: apical notch, N2: coronal notch, NB: new bone formation, JE: junctional epithelium.

Figure 4
Representative photomicrographs in the test (reciprocal autologous root transplantation) group. (A) Overview of the class III furcation defects (scale bar=2 mm). (B) Higher magnification of the framed area in (A) (scale bar=100 μm). (C) Higher magnification of the framed area in (A) (scale bar=100 μm). (D) Higher magnification of the framed area in (A) (scale bar=100 μm), toluidine blue staining.
N1: apical notch, N2: coronal notch, CEJ: cementoenamel junction, NB: new bone formation, RR: root resorption, ANK: ankylosis.

Histometric analysis
The results of the histometric analysis are summarized in Table 2. There was no significant difference in DH between the 2 groups. The distance between the mesial and distal roots in the test group was significantly shorter than in the control group. NB was significantly greater in the test group than in the control group. In the test group, ANK was detected, although the difference between the test group and the control group was not statistically significant. The occurrence of RR in the test group was significantly higher than in the control group.
Table 2
Histomorphometric parameters for each surgical treatment (4 dogs and 8 sites; 4 sites per group)

DISCUSSION
The amount of NB in the class III furcation defects was significantly greater in the test (reciprocal autologous root transplantation) group than in the control group. These findings may be attributed to the potential of the preserved PDL cells on the transplanted root surfaces. PDL cells with osteoblastic properties express type I collagen, alkaline phosphatase, and basic fibroblast growth factor, as well as proteins that respond to cytokines, such as insulin-like growth factor, bone morphogenetic protein 2, and transforming growth factor β1 (TGF-β1) [262728]. After root transplantation, osteoblasts that are derived from healthy PDL might play an important role in forming new bone along the cementum of the root surface from the basal part of the bone defect. Furthermore, the greater amount of bone formation and reestablishment of attachment in the test group may be explained by the fact that the root divergence was approximately 20°, and the distance between the mesial and distal roots was significantly shorter than in the control group. The condition is thought to be advantageous for facilitating sufficient blood clotting and periodontal wound healing (regeneration) in class III furcation defects. As a result, the bone crest level in the defects became comparable to that in the mesiodistal region, which may contribute to a reduced risk of plaque accumulation in class III furcation defects.
RR is considered to result from severe damage to the PDL and cementum [162930]. The causes of damage are thought to come from physical stress during tooth extraction, the operation outside the oral cavity, or transplantation to the alveolar socket [3132]. Although some RR localized in the cementum or superficial dentin was observed, it may recover through a new attachment-like healing process by cementoblasts differentiated from PDL cells [162933]. It has been demonstrated that enamel matrix derivative (EMD) has TGF-β or bone morphogenetic protein-like activity, and is effective for periodontal regeneration [3435]. Clinically, EMD is applied in cases of tooth autotransplantation or the replantation of an avulsed tooth caused by injury, and it is expected to inhibit ANK or RR and to promote periodontal wound healing [303637]. Therefore, ANK might be inhibited to some extent by using EMD in reciprocal autologous root transplantation. Furthermore, EMD could be expected to decrease RR because it might promote periodontal wound healing of small injuries to the PDL and cementum [38]. It is also important that roots are transplanted in such a manner that they do not press the PDL against bone forcefully in order to minimize ANK [162939]. It has been shown that osteoblasts from neighboring bone invade the damaged PDL and cementum on the root surface before the repair is performed by PDL-derived cementoblasts, and, as a result, the adhesion of the bone and root surface and RR affect bone remodeling. Therefore, these complications are likely to occur when existing bone comes into close contact with the root surface because an insufficient recipient alveolar socket is formed. Considering the morphologic differences between the mesial and distal roots, such as length and flexure, it is necessary to form a recipient socket with a small margin. Thus, positioning of the transplanted root and adequate recipient socket preparation are necessary in order to prevent RR.
Within the limits of an animal pilot study, it can be concluded that reciprocal autologous root transplantation is effective for bone regeneration in class III furcation defects in dogs. We suggest that this novel technique may be a feasible treatment option for preserving teeth in large furcation defects. However, further studies with short- and long-term observations are required to clarify the clinical predictability of this technique and to determine the optimal approach for reciprocal autologous root transplantation in a larger number of animals/humans under strictly standardized conditions.
 XML Download
XML Download