

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic periodontitis is an inflammatory disease induced by pathogenic periodontal bacteria [12]. Porphyromonas gingivalis (P. gingivalis) is a bacterium commonly associated with chronic periodontitis [345] and is responsible for stimulating inflammatory responses related to tissue destruction in some areas [67]. Recently, P. gingivalis has been revisited as a “keystone pathogen” for plaque formation and growth via its synergistic interactions with other pathogens [8].
Conventionally, periodontal diseases are classified according to the clinical attachment level (CAL) [91011]. The CAL indicates the degree of attachment loss, which is the sum of gingival recession and the probing pocket depth (PPD). Gingival recession implies past inflammation of the site, while an elevated PPD suggests current inflammation. Accordingly, the CAL is an index that represents inflammation in the past and present and is advantageous for determining the prognosis of individual teeth [1213].
Recently, an attempt was made to quantify the present inflammatory burden posed by periodontal diseases. The periodontal inflamed surface area (PISA) is the sum of the PPD of bleeding on probing (BOP)-positive sites for the total dentition and can be easily calculated using routine periodontal charting [14]. Gingival bleeding is a critical sign of inflammation and a useful parameter for identifying teeth with active inflammation [1516]. PISA values represent the degree of periodontal inflammation in a quantitative manner and can be used to distinguish subjects with actively inflammatory dentition from those with non-inflamed or healed dentition. However, the relationship between PISA and conventional periodontal indexes has not been examined in systemically healthy periodontal patients. In addition, the presence of periodontal pathogens has not been evaluated in relation to the periodontal inflammatory burden.
This study aimed to evaluate associations between PISA and periodontal disease. For this purpose, correlations between PISA and conventional periodontal indexes and classifications were examined, and the association between PISA and P. gingivalis expression was investigated.
MATERIALS AND METHODS
Study subjects
This study was a cross-sectional post-hoc analysis of data from a prospective cohort study investigating the association and impact of chronic periodontitis on the clinical features of ankylosing spondylitis (AS) [17]. In the original cohort study, 84 AS patients from the Rheumatology Clinic at Seoul National University Bundang Hospital were enrolled, and age- (within 5 years) and gender-matched healthy controls (n=84) were recruited from the same geographical area through local advertisements. The present study used data from the healthy controls without AS because the AS patients had been taking anti-inflammatory drugs affecting gingival inflammation, including sulfasalazine (n=25), anti-tumor necrosis factor alpha agents (n=25) or non-steroidal anti-inflammatory agents regularly or as needed (n=63).
Subjects were excluded if they had received periodontal therapy within the previous 6 months or had taken antimicrobial agents, immunosuppressive drugs, or corticosteroids within 3 months before enrollment. Additional exclusion criteria included a history of diabetes or clinical inflammatory bowel disease. The study was approved by the local Ethical Committees (IRB No. B-1206/156-001), and written informed consent was obtained from all participants. The study complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Clinical data collection
Age, gender, smoking and drinking history, socioeconomic status, education levels, co-morbidities, recent medication history, body mass index (BMI), dental visits within the past 12 months, and brushing habits were recorded at baseline for all subjects by a well-trained oral health researcher.
Periodontal examination and conservative periodontal treatment
A periodontal examination that included the plaque index (PI), PPD, CAL, and BOP was performed by a single dentist (Lee JT) at 6 sites per tooth, excluding the third molars, using a University of North Carolina (UNC)-15 periodontal probe (Hu Friedy, Chicago, IL, USA). The BOP was presented as the ratio of the BOP-positive surface to the total dental surface and the PI as the ratio of the plaque-positive surface to the total dental surface. All measurements were made as previously described [111819].
In this study, chronic periodontitis was defined according the following criteria proposed by the Centers for Disease Control and Prevention working group. Severe periodontitis was defined as at least 2 sites with attachment loss ≥6 mm (not on the same tooth) and at least 1 site with a PD ≥5 mm. At least 2 sites with attachment loss ≥4 mm (not on same tooth) or at least 2 sites with a PD ≥5 mm indicated moderate periodontitis. If neither moderate nor severe periodontitis applied, mild periodontitis was recorded [11].
Analysis of gingival crevicular fluid (GCF)
The presence of P. gingivalis DNA in crevicular fluid was identified with a polymerase chain reaction (PCR)-based investigation [20]. GCF was collected from the tooth with the deepest sites using 3 sterile paper points (Diadent Group International, Burnaby, Canada). Prior to sampling, the sites were cleaned of supragingival plaque and saliva using sterile cotton pellets and were isolated with cotton rolls and air [21]. Each paper point was inserted into the gingival crevice until it met resistance and left in place for 30 seconds. The paper points with GCF were immediately placed in a sterile tube and stored at −20°C until they were analyzed. The presence of P. gingivalis was determined using rpoB-specific primers (GenBank accession No. NC_010729), as previously reported [22]. The templates were prepared by suspending the paper strip in 200 μL of sterile water, followed by boiling for 10 minutes and centrifuging for 30 minutes. The 143-bp PCR products were detected on 1.5% agarose gel. The presence of P. gingivalis was determined based on whether the PCR test result was positive.
Analysis of blood samples
Peripheral venous blood was sampled at enrollment and then centrifuged, and the serum was stored at −80°C. P. gingivalis strain FDC381 (ATCC® BAA-1703™) was grown in brain-heart infusion broth (Difco, Detroit, MI, USA) supplemented with hemin (5 μg/mL), vitamin K (0.5 μg/mL), and cysteine (0.05%). The cultures were incubated under anaerobic conditions at 37°C for 3 days. After the removal of the media, the P. gingivalis cells were washed with phosphate-buffered saline 3 times and then treated with 3% formaldehyde. After centrifugation, the cells were washed with sodium carbonate coating buffer (pH 9.6). A 96-well microtiter plate (NUNC, Roskilde, Denmark) was coated with 1×107 cells/well in 50 mM sodium carbonate coating buffer (pH 9.6) overnight at 4°C. After blocking with albumin, serum diluted to 1:200 or more was added to the plate. Anti-P. gingivalis immunoglobulin G (IgG) antibodies were detected using horseradish peroxidase conjugated to anti-human IgG antibodies (1:6,000 dilution, Millipore, Billerica, MA, USA) and 3,3′,5,5′-tetramethylbenzidine (Kirkegaard & Perry Laboratories, Inc., Gaithersburg, MD, USA). The serum antibody level was defined as the inverse value of the largest serial dilution for which detectable antibodies were observed.
Statistical analysis
After the creation of the original study database, 2 authors (Park SY and Ahn S) pre-planned all the statistical analyses. Prior to the statistical analysis, a power analysis of this study was performed. At a given sample size of 84 subjects and with an odds ratio of 2, a P. gingivalis DNA detection prevalence of 0.4, and a significance level of 0.05, the power analysis for the logistic regression analysis was calculated as 81.8% (G*Power 3.1.5, Franz Faul, Universität Kiel, Germany).
One-way analysis of variance with the Bonferroni post hoc test or χ2 test was performed to examine the periodontal condition according to the conventional classification. To examine the relationship between PISA and periodontal conditions, the Student's t-test, Spearman rank correlation test, or the Pearson correlation test was conducted using PISA and periodontal variables. To evaluate the associations between PISA and periodontal conditions, univariate linear regression analysis was performed to identify other significant variables affecting PISA values (P<0.1). In this analysis, the PISA and serum P. gingivalis antibody level values were log-transformed because of their skewness. BMI, smoking, classification of periodontal diseases, brushing, BOP, PI, P. gingivalis expression, and serum P. gingivalis antibody levels significantly influenced PISA values. Among these factors, BOP and current smoking were excluded as variables for the multivariate analysis due to their collinearity. For PISA and other significant variables, a final model was established for multivariate linear regression. P values <0.05 were considered to indicate statistical significance. The statistical analyses were performed using STATA/SE13 (Stata Corp., College Station, TX, USA).
RESULTS
The characteristics of the subjects included in this study are summarized in Table 1. Of a total of 84 subjects, 68 were male and 16 were female. Because of the etiology of AS, the age- and gender-matched control group that was used in the present study also had more male subjects. The mean (standard deviation) age of the subjects was 37.8 years (11.1 years). Thirty-five subjects (41%) were positive for P. gingivalis DNA. Of the 84 subjects, 28 (33%) were diagnosed with no or mild periodontitis, 40 (48%) with moderate periodontitis, and 16 (19%) with severe periodontitis. BOP (%), PI (%), the proportion of P. gingivalis DNA detection in the group, and serum P. gingivalis antibody levels increased with disease severity, and this trend was statistically significant (Figure 1).
Table 1
Characteristics of the subjects included in this study

Values are presented as mean (standard deviation).
BMI: body mass index, BOP: bleeding on probing, PI: plaque index, PISA: periodontal inflamed surface area, P. gingivalis: Porphyromonas gingivalis.
![]()
 | Figure 1Periodontal conditions according to the severity of periodontal disease (A-D). Box-plot diagrams showing BOP (%) and PI (%) according to the severity of periodontal disease; BOP and PI increased with disease severity (P=0.04 and P=0.10, respectively; 1-way ANOVA with the Bonferroni post hoc test; A and B). A histogram showing P. gingivalis DNA detection in periodontal patients; P. gingivalis DNA detection was more frequently observed in subjects with severe periodontal disease (P<0.01; χ2 test; C). A box-plot diagram showing that serum P. gingivalis antibody levels were also higher in patients with severe periodontal disease (P<0.01 and P<0.01, respectively; 1-way ANOVA with the Bonferroni post hoc test; D).
BOP: bleeding on probing, PI: plaque index, ANOVA: analysis of variance, P. gingivalis: Porphyromonas gingivalis.
|
Correlations between PISA and variables affecting periodontal disease
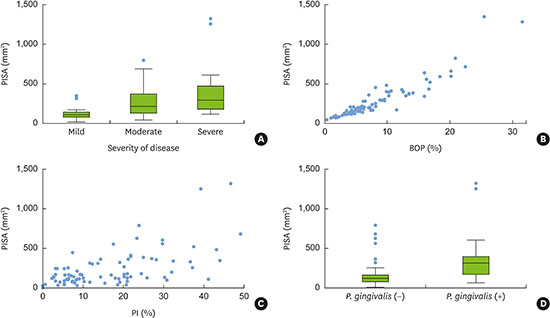
PISA values increased with increasing periodontal disease severity, and this difference was statistically significant (Spearman correlation coefficient=0.52; P<0.01; Figure 2A). In addition, the PISA values showed a positive correlation with the BOP index and the PI (r=0.94; P<0.01 and r=0.60; P<0.01, respectively; Pearson correlation test; Figure 2B and C). The subjects in the P. gingivalis (+) group had significantly higher PISA values than those in the P. gingivalis (−) group (P<0.01; Figure 2D).
 | Figure 2Correlation of PISA values with periodontal conditions (A-D). A box-plot diagram showing PISA levels in periodontal patients according to the severity of the diseases; PISA values significantly increased with increasing periodontal disease severity (Spearman correlation coefficient=0.52; P<0.01; A). Scatter plots showing correlations of PISA and BOP and of PISA and PI (r=0.94; P<0.01 and r=0.60; P<0.01, respectively; Pearson correlation test; B and C). A box-plot diagram showing PISA values in subjects in P. gingivalis (+) or P. gingivalis (−) groups; the P. gingivalis (+) group showed significantly higher PISA values than the P. gingivalis (−) group (P<0.01, Student t-test; D).
PISA: periodontal inflamed surface area, BOP: bleeding on probing, PI: plaque index, P. gingivalis: Porphyromonas gingivalis.
|
PISA values as a multifunctional index integrating the conventional periodontal indexes
In the multivariate linear regression analysis, the quantity of current smoking, the presence of periodontal disease, and PI were significantly associated with PISA values (Table 2). P. gingivalis DNA detection and serum P. gingivalis antibody levels did not significantly influence the PISA value. In a prediction curve to estimate PISA values, it was found that PISA values increased with the PI and quantity of current smoking (Figure 3). However, PISA values did not significantly differentiate moderate periodontitis from severe periodontitis, although they showed distinct values between mild periodontitis and the other types.
Table 2
Linear regression analysis of factors affecting PISA

PISA: periodontal inflamed surface area, CI: confidence interval, BMI: body mass index, BOP: bleeding on probing, PI: plaque index, N/A: not applicable, P. gingivalis: Porphyromonas gingivalis.
![]()
 | Figure 3Graphs predicting PISA values according to the multivariate linear regression analysis. PISA values increased with PI and the quantity of current smoking (A). When the severity of periodontal disease was incorporated into the analysis, the PISA value also increased with increasing PI, but there was no difference between moderate and severe disease, although PISA values showed distinct values between mild disease and moderate or severe periodontitis (B).
PISA: periodontal inflamed surface area, PI: plaque index.
|
DISCUSSION
In this study, we demonstrated that PISA is a representative periodontal index describing periodontal inflammation. PISA showed significant correlations with conventional periodontal classifications or indexes and significantly increased with PI and the quantity of current smoking. To our knowledge, this study is the first to investigate the factors affecting PISA in systemically healthy periodontal patients.
Unlike conventional periodontal indexes, PISA values represent an individual's periodontal condition as a continuous variable, which avoids the loss of information during statistical analysis [23]. PISA facilitated multivariate regression analysis, as a variable that integrates disease severity and conventional periodontal measurements, such as BOP and PI. Continuous variables have some merits in data processing compared with categorical variables. Furthermore, PISA values integrate periodontal conditions into a value rather than presenting them as discrete data. For example, although massive datasets have resulted from conventional periodontal charting (data from 168 PPDs, 168 CALs, 168 BOPs, 168 gingival indexes, and 168 PI values can be obtained from a person with 28 teeth if 6 sites per tooth are measured), the data are discrete and can be difficult to apply and integrate for statistical analysis. In addition, data losses occur during the data processing for statistical analysis, and accurate descriptions of the patient may be unavailable at times. Therefore, PISA is an advantageous index, as it represents a subject’s periodontal condition as a continuous variable.
In addition, PISA might bridge the gap between conventional periodontal classifications and an individual's current periodontal status. In a recent review of periodontal disease and cardiovascular diseases, some previous studies have failed to identify statistical associations between periodontal and systemic diseases [24]. However, other studies using PISA values to determine periodontal status showed a significant relationship between periodontal and systemic diseases [2526]. Therefore, PISA could be considered an alternative periodontal index that represents an individual's periodontal status and could be widely applied in various periodontal studies. However, the evidence supporting PISA as a comprehensive periodontal index remains insufficient, and this study may provide the scientific background for using PISA to assess chronic periodontitis.
P. gingivalis is one of the major pathogens implicated in chronic periodontitis, and 88% of the subjects with severe periodontitis were P. gingivalis (+) in this study. Recently, P. gingivalis has emerged as a target bacterium for explaining the relationship between periodontal and systemic diseases [2728] and has been suggested to be a pathogen responsible for the propagation of rheumatoid arthritis (RA) [2930]. P. gingivalis is the only known pathogen expressing peptidylarginine deiminase, which induces adaptive immune responses, including the production of anti-citrullinated peptide antibody, which is exclusive to RA [3132]. Our previous study showed that P. gingivalis carriage status was associated with spinal dysmobility in AS patients [17]. However, the present study failed to show a significant relationship between P. gingivalis DNA detection, PISA, and serum P. gingivalis antibody levels. Since periodontal diseases are caused by complex pathogens including P. gingivalis, the total amount of plaque was a more significant factor inducing periodontal inflammation in this study. Similarly, serum P. gingivalis antibodies did not significantly influence periodontal inflammation. The role of the specific antibody remains controversial. Some researchers have reported that the antibody exerted positive actions in treatment and was associated with a better disease prognosis [23334]. In contrast, others have suggested that elevated antibody levels are a result of repeated bacterial infections, rather than an ability to clear the subgingival infection [3536]. Therefore, antibodies to P. gingivalis and the presence of P. gingivalis did not weaken or aggravate periodontal inflammation in systemically healthy periodontal patients.
Smoking is well-known factor affecting periodontal inflammation. The harmful effects of smoking were thoroughly reviewed in an article by Kinane and Chestnutt [37]. Smoking influences host-related factors through its impacts on the subgingival niche and the microflora therein, as well as the host defense system, including the inflammatory and immune systems. In addition, periodontal treatment outcomes are also influenced by smoking; smokers show less resolution of gingival inflammation, less reduction of PPD, and less gain of CAL than non-smokers. Müller et al. [38], in a longitudinal study, reported that smokers had a high risk of transitioning from non-BOP to BOP. Therefore, smoking increases the number of BOP-positive sites, corresponding to an increase in PISA. Indeed, the quantity of current smoking increased PISA in a dose-dependent manner. Therefore, current smoking is considered to be a strong confounder affecting the results of studies about periodontal inflammation and systemic diseases when PISA is used as a periodontal index.
This study has several limitations. First, this study was a sub-group analysis, and the sample size was not sufficient to control for the many confounding variables or for comparative subgroup analyses. Second, we did not perform quantitative measurements of P. gingivalis, and correlations between P. gingivalis and PISA could not be examined. Third, the effects of other representative periodontal pathogens on PISA were not evaluated. To confirm the additional effect of specific pathogens on periodontal inflammation, a quantitative analysis through standardization of the GCF sampling methods is needed in further studies.
In conclusion, PISA was closely correlated with conventional periodontal indexes and was significantly associated with plaque and smoking quantity. For the general application of PISA, further cross-sectional clinical studies in large populations and longitudinal studies of the changes in PISA values with disease progression and remission should be conducted.
 XML Download
XML Download