

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tooth loss (TL) is a crucial measure of oral healthcare and the efficacy of oral disease management [1]. Despite improvements in awareness and treatment worldwide, TL remains a major public health issue [23]. TL can impair not only mastication, but also self-esteem and social interactions due to its effects on appearance, the ability to have a conversation, and the willingness to laugh [45]. These problems can significantly reduce quality of life [678]. Moreover, the impairment of chewing abilities due to TL is associated with deficiencies and imbalances in nutrition, especially in the elderly population [9].
The main etiology of TL is dental caries and periodontal disease (PD) [10]. Many studies have found dental caries to be the most common cause of TL, although the main cause of TL as age increases is PD, regardless of race or sex [1112]. More than half of the world's population is affected by PD, including an estimated 14 million Koreans in 2016, making it the second-most-frequent outpatient disease, with outpatient medical treatment benefits amounting to about US$ 1.1 billion [13].
Korea is now an aging society, with more than 7% of the population at least 65 years old in 2000, and it is expected to become a superaged society, with more than 21% in this age group by 2026. This increase in the elderly population is resulting in a rapid increase in the proportion of PD patients with chronic wasting disease [14]. Several studies have shown that PD affected the severity and incidence of cardiovascular disease, diabetes mellitus, low birth weight, rheumatoid arthritis, chronic kidney disease, lung disease, systemic cancer, erectile dysfunction, osteoporosis, and Alzheimer disease, with these comorbid diseases in turn being risk factors or risk indicators for PD [1516171819].
Interest in the quality of life related to oral health has increased markedly over the past few decades, prompting a corresponding increase in the number of patients receiving a PD diagnosis and treatment [2021]. Nevertheless, insufficient research has been conducted into trends in TL due to PD, which is considered to be one of the important factors influencing whole-body health and quality of life. Therefore, the purpose of this study was to determine the trends of tooth extraction due to acute and chronic PD using data from the National Health Insurance Service-National Sample Cohort provided by the National Health Insurance Service (NHIS).
MATERIALS AND METHODS
Data sources and study samples
The NHIS has a compulsory-enrollment health insurance database (DB) containing data related to about 52 million Koreans. This DB contains more than 1 trillion clusters of individual DBs that include information on sociodemographic and economic factors, records of medical and dental practices, detailed descriptions and prescription codes, the history of rare incurable diseases, and records of systemic cancer and long-term care services. The NHIS made the Korean National Health Insurance Cohort Database (KNHICD) available to epidemiologists for research purposes in 2013, and the present study was based on a retrospective analysis of the KNHICD from 2002 to 2013. Among the 97% of the population (51,448,491 people) guaranteed to be covered by the NHIS in 2002, 1,476 groups were sampled by stratification according to sex (2 groups), age (18 groups: those aged 1–79 years in 5-year intervals, and those >80 years old), and household income level (41 groups: those with job-based health insurance and those without, accounting for 20 groups each, and the health insurance Medical Aid Program [MAP] in 0 groups). A random sample of 1,025,340 individuals was selected as a representative sample of the population, and the KNHICD was followed up for 12 years until 2013. Among the subjects included in the sample in 2002, those who were no longer present in the DB in 2013 due to death or immigration were replaced by records of newborns born in the same year. In order to protect personal information, the identification number of each patient was anonymized, with all personal information managed only by the NHIS, and we were therefore only provided with an individual's random identification code when requesting the cohort data. This study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational cohort studies (www.strobe-statement.org), and it was approved by the Institutional Review Board of Daejeon Dental Hospital, Wonkwang University (approval No. W1612/002-001).
PD was classified using the Korean Classification of Disease, 6th edition (KCD-6), which is a modification of the International Classification of Disease, 10th edition (ICD-10) based on NHIS criteria. Acute PD (KCD-6 code K05.2, corresponding to ICD-10 code K05.2) and chronic PD (KCD-6 code K05.3, corresponding to ICD-10 code K05.3) were classified according to the criteria of the Centers for Disease Control and Prevention/American Academy of Periodontology Case Definitions and diagnosed by a general dentist or periodontist [2223]. In order to ensure that the diagnoses were accurate, patients with PD were defined as those who were diagnosed at least 3 times.
Total extraction (TE) was defined as including all extractions except for the extraction of deciduous teeth (U4411); thus, this category included the extraction of anterior teeth (including incisors and canines; U4412), posterior teeth (including premolars and molars; U4413), complicated impacted teeth (U4414), simple impacted teeth (U4415), complex impacted teeth (U4416), and completely impacted teeth (including osteotomy and osteoplasty; U4417), as registered in the NHIS description-code DB. Extraction due to periodontal disease (EPD) was defined as occurring in individuals with PD that was diagnosed at least 3 times, leading to the extraction of teeth other than deciduous teeth and impacted third molars. Within the category of EPD, immediate extraction due to periodontal disease (IEPD) was defined as extraction on the same day as the diagnosis of PD.
Statistical analysis
Based on multivariate logistic regression analysis, we assessed the incidence of TE, EPD, and IEPD according to sociodemographic factors (sex, age, household income, health status, and area of residence). Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to identify the sociodemographic risk factors associated with extraction. P values <0.05 were considered to indicate statistical significance. All statistical analyses were performed by the Department of Health Insurance Research, Ilsan Hospital, NHIS and the Department of Periodontology, Daejeon Dental Hospital, Wonkwang University using the SAS statistical package (version 9.2, SAS Institute, Cary, NC, USA) and SPSS statistics (version 19, IBM Corp., Armonk, NY, USA).
RESULTS
Incidence of tooth EPD
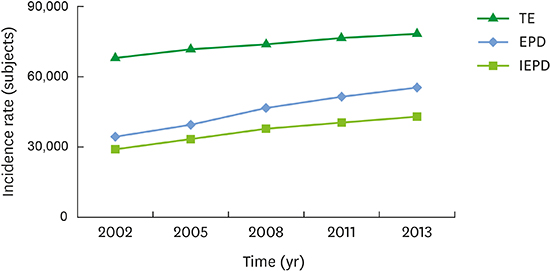
TE was performed in 67,976 patients in 2002, of whom 34,402 (50.6%) received EPD. In 2013, 55,447 (70.8%) of the 78,311 patients in whom TE was performed had been diagnosed with PD. The number of patients with TE and EPD both increased between 2002 and 2013. The number of patients who underwent IEPD also increased, from 29,067 in 2002 to 43,003 in 2013 (i.e., by 32.4%; Figure 1).
 | Figure 1Incidence of tooth extraction according to the presence of acute PD in Koreans during 12 years of follow-up in the National Health Insurance Service-National Sample Cohort.
PD: periodontal disease, TE: total extraction, EPD: extraction due to periodontal disease, IEPD: immediate extraction due to periodontal disease.
|
The number of patients who underwent EPD due to acute PD increased from 4,588 in 2002 to 6,806 in 2013 (i.e., by 32.6%). The number of patients who underwent IEPD due to acute PD increased only slightly, from 2,241 in 2002 to 2,494 in 2013 (i.e., by 11.3%). In contrast, the number of patients who underwent EPD and IEPD due to chronic PD steadily increased, from 29,814 in 2002 to 48,641 in 2013 (i.e., by 38.7%) and from 26,826 in 2002 to 40,509 in 2013 (i.e., by 33.8%), respectively (Figure 2).

Associations between sociodemographic factors and tooth extraction
The risks of TE, EPD, and IEPD were lower among females than among males (P<0.001). In all TE cases, the OR increased significantly with age among patients in their 20s, while it decreased with age among patients in their 60s, and especially among those in their 70s. The risk of TE increased with income level. Similarly, the OR was 2-fold higher among patients in the NHIS (self-employed and employees) than among those in the MAP. The OR for TE was lower among patients with disabilities than among those without disabilities. In addition, the OR was higher among patients living in urban areas than among those living in rural areas (Table 1).
Table 1
Results of multivariate logistic regression of the incidence of tooth extraction according to the presence of PD in Korean during 12 years of follow-up in the National Health Insurance Service-National Sample Cohort

The multivariate logistic regression adjusted for sex, age, household income, insurance status, health status, and area of residence.
PD: periodontal disease, TE: total extraction, EPD: extraction due to periodontal disease, IEPD: immediate extraction due to periodontal disease, OR: odds ratio, CI: confidence interval, MAP: Medical Aid Program, NHIS: National Health Insurance Service.
a)Statistical significance (P<0.05).
![]()
In terms of sociodemographic characteristics, the OR for tooth extraction was lower among females for both acute and chronic PD, and it increased monotonically with age until the patients were in their 60s, but not in their 70s. In addition, the OR was significantly higher in patients with higher income levels, in the NHIS (self-employed and employees), without disabilities, and who lived in urban areas (Table 2).
Table 2
Results of multivariate logistic regression of the incidence of tooth extraction according to the presence of acute and chronic PD in Korean during 12 years of follow-up

The multivariate logistic regression adjusted for sex, age, household income, insurance status, health status, and area of residence. Classified as acute PD (KCD-6 code K05.2, corresponding to ICD-10 code K05.2) and chronic PD (KCD-6 code K05.3, corresponding to ICD-10 code K05.3) according to the criteria of the Centers for Disease Control and Prevention/American Academy of Periodontology Case Definitions.
PD: periodontal disease, OR: odds ratio, CI: confidence interval, MAP: Medical Aid Program, NHIS: National Health Insurance Service, KCD-6: Korean Classification of Disease, 6th edition, ICD-10: International Classification of Disease, 10th edition.
a)Statistical significance (P<0.05).
![]()
DISCUSSION
This study investigated the relationship between the incidence of tooth extraction and sociodemographic factors, using a cohort of 1 million people who constituted a 2% representative sample of the total population of Korea. The incidence of TE, EPD, and IEPD was higher in males and in those with high household incomes, who were enrolled in the NHIS (self-employed and employees), who had no disability, and who resided in urban areas.
In our previous study conducted in the same population 1 year ago, we found that the number of cases of periodontal nonsurgical (subgingival scaling, root planing, and curettage) and surgical treatments (open-flap debridement, guided tissue regeneration, and guided bone regeneration) has also been increasing steadily with the increasing incidence of PD [20]. In terms of promoting periodontal health and preventing TL, periodontal treatment can be considered effective when the incidence rates of EPD and IEPD are reduced. However, in contrast to our expectations, the incidence of TE has been increasing, while the rates of EPD and IEPD have been increasing even more rapidly. As for the above-mentioned trend, the rates of EPD have been increasing monotonically because of both acute and chronic PD, while those of IEPD are also increasing steadily.
The ORs for EPD and IEPD were higher among patients in their 30s to 50s than among those in their 20s, and then decreased in patients in their 60s. The ORs were 3 times higher among patients in their 50s than among those in their 20s. The ORs were lower among patients in their 60s than among those in their 50s, but were 2.7 times higher among patients in their 60s than among those in their 20s. This may be due to access to dental healthcare services being better for patients in their 30s to 50s than for those in their 20s owing to their higher economic status [242526]. Although the medical costs for dental diagnosis and treatment are largely covered by health insurance, 74.5% of all dental diagnoses and treatments performed in 2010 were not covered by health insurance. This may be why a large proportion of patients in this study who received dental treatment and underwent tooth extraction were in their 30s to 50s.
The decrease in the OR for tooth extraction with age among patients in their 60s observed in this study may have been due to a reduced access to dental clinics and limitations of the cohort DB used in this study. Older patients experience greater physical and economic difficulties in accessing dental clinics [2728]. As the DB used in this study involved patients who voluntarily visited dental clinics to receive a diagnosis of PD, patients who received a NHIS description-code (extraction) and vulnerable patients who could not visit dental clinics were excluded. This limitation of the study may explain why the incidence and OR for tooth extraction were both significantly lower among beneficiaries with low economic status and patients with disabilities who had greater physical difficulties.
IEPD did not differ significantly by area of residence, which may have been due to the relatively high physical accessibility of dental clinics in Korea. Practicing dentists represented 81.6% of all licensed dentists in Korea in 2014, which is the second highest proportion among the Organization for Economic Cooperation and Development (OECD) countries after Australia [29]. Statistics provided by the Health Insurance Review and Assessment Service show an average of 4.7 dentists per 10,000 persons in Korea in October 2016, which is higher than the average proportion of dentists worldwide. This proportion was higher than the average in regions with more than 1,000,000 residents, as well as the average in rural areas [30]. Such a high proportion of dentists may explain the absence of differences in tooth extraction rates among different regions in Korea.
Access to dental clinics has increased as household incomes and education levels have improved over time. Although dental healthcare policies and medical systems for improving oral health and reducing TL have been improved, TE, EPD, and IEPD are being performed at an increasing rate. Numerous studies have found that education level is closely associated with TL, with a low education level being an important risk factor for TL [313233]. The cohort DB used in the present study did not include any information on education level, and so we could not assess the direct effects of education level on the extraction rate. However, we found that the TE, EPD, and IEPD rates were more than 2-fold higher among patients with high income levels and among those who were not beneficiaries of health insurance [20].
The Korean government has consistently increased its coverage for dental diagnoses and treatment to reduce the financial burden from dental services for people of all socioeconomic backgrounds and living in all types of areas of residence (e.g., the government has included prophylactic scaling and dental implants in health insurance coverage since 2013). However, despite these efforts, even greater social and economic costs are anticipated because of population aging and increases in income disparities, which are occurring more rapidly in Korea than in other OECD countries. In addition, the cohort DB used in this study only included data collected between 2002 and 2013, so changes in trends regarding tooth extraction in response to recent changes in dental healthcare policies could not be assessed. Nonetheless, the NHIS is planning to continue adding a longitudinal cohort DB in the near future, so meaningful results could thereby be obtained if we continue to assess continuing trends in the incidence of tooth extraction.
Notwithstanding the limitations of this study, the rates of TE, EPD, and IEPD were shown to have steadily increased despite the implementation of dental healthcare policies to expand public health insurance coverage. Moreover, these trends varied with both income and education levels. Changes in trends regarding tooth extraction according to healthcare policy changes should be monitored through consistent patient follow-up, which will help ensure optimal policy reviews and revisions.
 XML Download
XML Download