

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Titanium implants are commonly used to rehabilitate function following tooth loss [1]. A variety of preclinical and clinical studies have demonstrated that titanium dental implants exhibit excellent biocompatibility [2] and yield high survival and success rates [3].
Even though clinically successful, potential disadvantages of titanium implants include hypersensitivity to titanium, corrosion of the material, and esthetic problems, predominantly in thin gingival tissues [456]. In order to overcome these limitations and to meet patients' demands for metal-free dental implants and reconstructions, dental implants made of zirconia were introduced [7]. The hard and soft tissue integration of zirconia implants has been thoroughly investigated in preclinical studies [8910], but only limited scientific evidence is available comparing titanium and zirconia implants in the same experimental model.
Successful tissue integration of dental implants relies on osseointegration (at the hard tissue level) and the formation of a peri-implant mucosal seal (at the soft tissue level). The key parameters for assessing osseointegration are measurements of bone-to-implant contact (BIC) and removal torque values [7]. The majority of studies demonstrated no significant differences for those parameters between titanium and zirconia implants [1112]. Moreover, at the soft tissue level, from a quantitative and qualitative point of view, the dimensions of the peri-implant mucosa around zirconia implants are similar to those around titanium implants [1314].
The transition from bone-driven to a prosthetically-driven implant placement often results in buccal bone dehiscence defects [15]. Traditionally, exposed implant threads were treated using guided bone regenerative procedures. While this increases the treatment time and cost, observational studies demonstrated that not all dental implants were completely surrounded by bone in the longer term [1617]. Still, the majority of these implants were considered to be clinically successful, as judged by a stable mucosal margin (MM). More recent clinical data also suggested that small buccal dehiscence defects might not require guided bone regeneration, at least in the short term [15]. These observations are thought to be due to a tight mucosal seal at the soft tissue level. Zirconia dental implants associated with high biocompatibility and reduced plaque accumulation are speculated to be even more tissue-friendly [7]. Comparative evidence of titanium and zirconia dental implants with untreated buccal dehiscence defects is therefore needed. Currently, no preclinical experimental model has been used to study such defects, as it requires a chronic hard tissue defect (similar to a clinical situation).
The aim of the present study was to validate an experimental model for assessing tissue integration of titanium and zirconia implants with and without buccal dehiscence defects.
Go to : 
MATERIALS AND METHODS
The present study was designed as a pilot experimental study. A total of 3 mongrel dogs (2 years old) weighing a maximum of 30 kg were used. The dogs were housed individually under standard laboratory conditions. Access to water ad libitum and a soft diet were provided throughout the entire study period. The protocol was approved by the Institutional Animal Care and Use Committee, Yonsei Medical Center, Seoul, Korea (approval No. 2016-0278).
Surgical procedures
All surgical procedures were performed under general anesthesia. General anesthesia was induced by an intravenous injection of atropine (0.04 mg/kg, Kwangmyung Pharmaceutical, Seoul, Korea) and an intramuscular injection of a combination of xylazine (Rompun, Bayer Korea, Seoul, Korea) and ketamine (Ketara, Yuhan Corporation, Seoul, Korea). Inhalation anesthesia (Gerolan, Choongwae Pharmaceutical, Seoul, Korea) was maintained throughout surgery.
Tooth extraction and creation of chronic defects
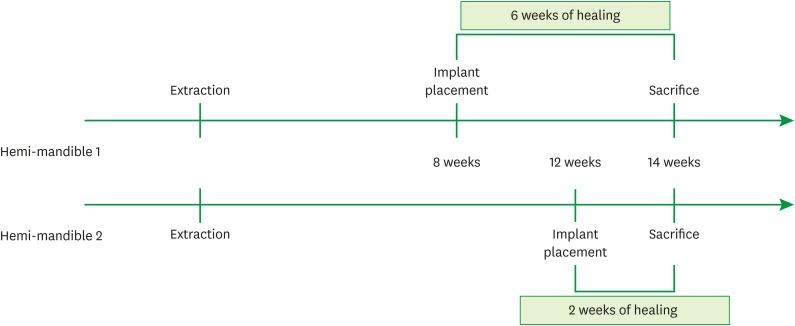
All mandibular premolars (P1, P2, P3, and P4) and the first molar (M1) were bilaterally extracted 8 weeks prior to implant placement. A crevicular incision from P1 to M1 was made, as well as 2 vertical incisions at the mesial side of P1 and the distal side of M1. The mucoperiosteal flap was reflected and the teeth were carefully extracted. Then, a one-wall defect was prepared by removing the buccal bone plate in the surgical sites randomized for undergoing implant placement with dehiscence defects. In all other sites, the extraction sockets were left intact. Primary wound closure was then obtained. Sutures were removed 7 days later.
Implant placement
Implant placement was performed in a staged manner on the left and right sides of the mandible to allow 2 healing time-points (6 weeks and 2 weeks, respectively). A mid-crestal incision was made from the canine to the second molar, and mucoperiosteal flaps were reflected. Five osteotomies for implant placement were performed according to the manufacturer's recommendation, allocating 5 experimental groups bilaterally in each dog (n=3 for each healing time-point) based on a computer-generated randomization list:
1) Z1: zirconia implant (AXIS HEXALOBE™ with a modified surface, Ø4.0×8 mm, AXIS biodental, Les Bois, Switzerland) placed within the bony housing,
2) Z2: zirconia implant (AXIS HEXALOBE™, Ø4.0×8 mm, AXIS biodental) placed within the bony housing,
3) T: titanium implant (CAMLOG® SCREW-LINE Promote® plus, Ø3.8×9 mm, Camlog Biotechnologies, Basel, Switzerland) placed within the bony housing,
4) Z1_D: Z1 implant placed with a 3-mm buccal bone dehiscence defect,
5) T_D: titanium implant placed with a 3-mm a buccal bone dehiscence defect.
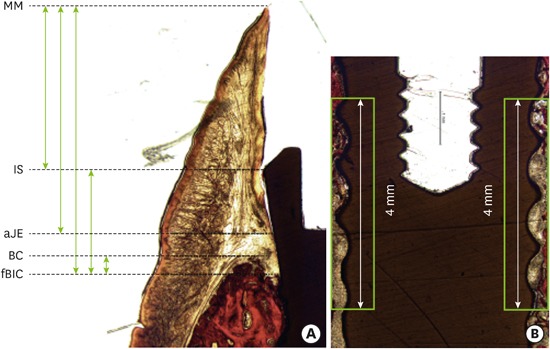
Three (Z1, Z2, and T) of the 5 osteotomies were within the bony housing, with 2 mm of buccal bone present after implant placement. For the other 2 sites (Z1_D and T_D), the preparation of the osteotomies resulted in a buccal dehiscence defect of 3 mm. No further buccal bone was removed in order to maintain a chronic ridge defect (Figure 1A).
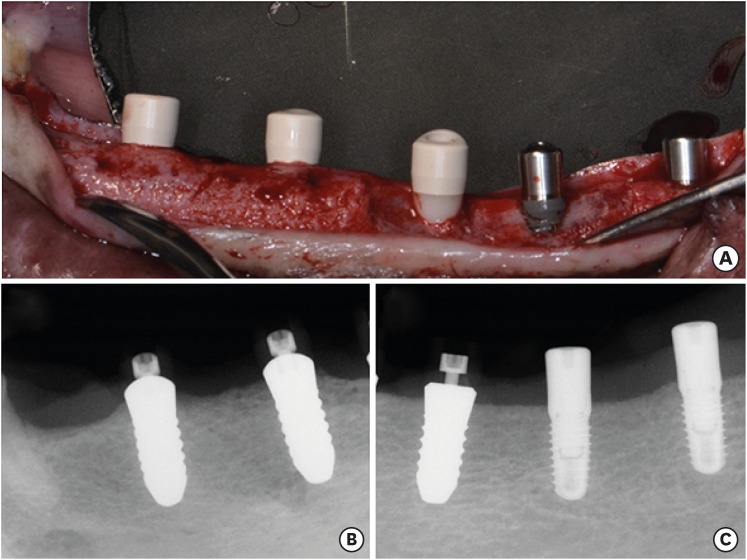
All zirconia implants were placed with the implant shoulder (IS) located 0.7 mm above the bone crest (BC). All titanium implants were placed with the transition between the rough and smooth surface at the level of the alveolar crest (the location of the IS was 0.4 mm above the BC). Healing abutments were connected to the implants and the flaps were sutured to allow for transmucosal healing. The sutures were removed 7 days later. The postsurgical management included daily irrigation with 0.2% chlorhexidine solution (Hexamedin, Bukwang Pharmaceutical, Seoul, Korea) and an intramuscular injection of antibiotics (20 mg/kg, cefazolin sodium, Yuhan Corporation). The dogs were sacrificed 6 weeks after the first implant procedure (one side of the mandible) and 2 weeks after the second implant procedure (opposite side of the mandible) (Figure 2). The implants and surrounding tissues were macroscopically inspected. Digital X-rays were taken using a standardized parallel technique (Figure 1B and C).
Histologic preparation
The harvested mandibles were fixed in 10% neutral-buffered formalin for 10 days. The specimens were trimmed and dehydrated in ethanol, and then embedded in methyl methacrylate. From each specimen, a central bucco-oral section through the implant site at 40–50 µm thickness was prepared using the microcutting and grinding technique adapted by Donath and Breuner [18]. Thereafter, the sections were visualized using van Gieson staining.
Analyses
Histometric analysis
The images from the histological slides were observed and captured using a light microscope (Leica DM6000 B, Leica Mikrosysteme, Wetzlar, Germany) equipped with a digital camera (Leica DFC 450, Leica Mikrosysteme). Subsequently, the acquired digital images were processed and analyzed using a software program (Photoshop CS6, Adobe, San Jose, CA, USA) and an automated image analysis system (Leica Application Suite Ver. 4.3, Leica Mikrosysteme).
Peri-implant soft tissue dimensions and BIC
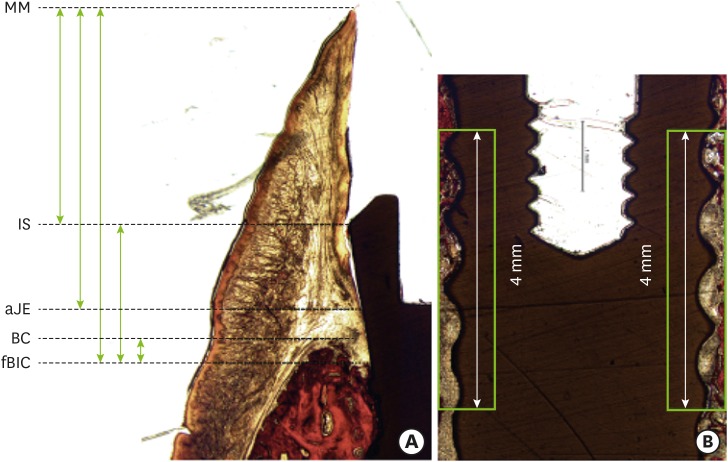
The following landmarks were located [9]: 1) the MM, 2) the IS, 3) the apical extension of the junctional epithelium (aJE), 4) the first bone-to-implant contact (fBIC), and 5) the BC. Subsequently, linear measurements were performed as follows: 1) the level of the mucosal margin relative to the implant shoulder (MM-IS), 2) the length of the junctional epithelium (MM-aJE), 3) the length of peri-implant mucosa (MM-fBIC), 4) the distance between IS and fBIC, with the subtraction of 0.7 mm (zirconia implant) or 0.4 mm (titanium implant) to account for the 2 different insertion protocols and height of the implant collars (IS-fBIC_c), and 5) the distance between the BC and the fBIC (BC-fBIC) (Figure 3A). Moreover, the mean of the buccal and lingual BIC (%) was calculated (Figure 3B).
Statistical analysis
Statistical analyses were performed descriptively to compare the intergroup differences at 2 and 6 weeks, and the intragroup differences over time. Mean values±standard deviation for each parameter are presented to describe the data. Due to the small sample size, no further statistical tests were performed.
Go to :
RESULTS
Clinical observations
All dogs remained healthy during the entire study period. Three implant fractures were observed: 2 in group Z1_D (one in the 2-week healing group and the other in the 6-week healing group) and one in group Z2. No implant lost osseointegration.
Histomorphometric analyses
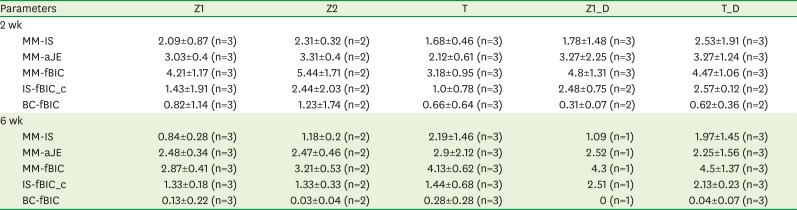
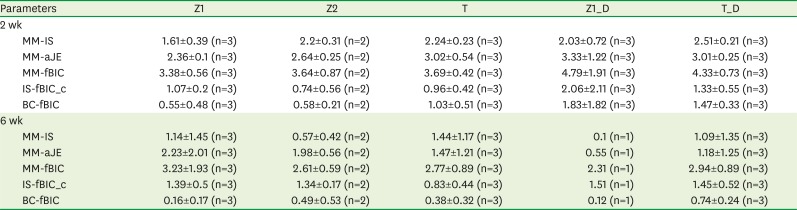
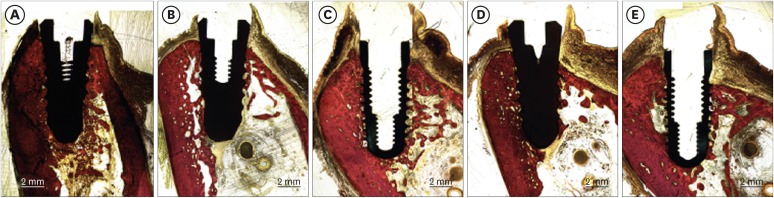
The data of the linear measurements are presented in Table 1 (for the buccal side) and Table 2 (for the lingual side). The fractured implants were only included for the measurements of BIC (Table 3). Figures 3 and 4 are representative histologic views of all groups at both 2 and 6 weeks (Figures 4 and 5).

 | Figure 4Representative histologic views at 2 weeks (van Gieson staining). (A) Group Z1. (B) Group Z2. (C) Group T. (D) Group Z1_D. (E) Group T_D.Z1: zirconia implant with a modified surface, placed within the bony housing, Z2: zirconia implant without a modified surface, placed within the bony housing, T: titanium implant placed within the bony housing, Z1_D: Z1 implant placed with 3 mm of buccal bone dehiscence, T_D: titanium implant placed with 3 mm of buccal bone dehiscence, B: buccal, L: lingual.
|
 | Figure 5Representative histologic views at 2 weeks (van Gieson staining). (A) Group Z1. (B) Group Z2. (C) Group T. (D) Group Z1_D. (E) Group T_D.Z1: zirconia implant with a modified surface, placed within the bony housing, Z2: zirconia implant without a modified surface, placed within the bony housing, T: titanium implant placed within the bony housing, Z1_D: Z1 implant placed with 3 mm of buccal bone dehiscence, T_D: titanium implant placed with 3 mm of buccal bone dehiscence, B: buccal, L: lingual.
|
Table 1
Linear measurements at the buccal area (in mm)
Values are presented as mean±standard deviation. No analyses were performed for implants that fractured.
Z1: zirconia implant with a modified surface, placed within the bony housing, Z2: zirconia implant without a modified surface, placed within the bony housing, T: titanium implant placed within the bony housing, Z1_D: Z1 implant placed with 3 mm of buccal bone dehiscence, T_D: titanium implant placed with 3 mm of buccal bone dehiscence, MM: mucosal margin, IS: implant shoulder, aJE: apical extension of the junctional epithelium, fBIC: first bone-to-implant contact, BC: bone crest, IS-fBIC_c: the distance between IS and fBIC, with the subtraction of 0.7 mm (zirconia implant) or 0.4 mm (titanium implant).
![]()
Table 2
Linear measurements at the lingual area (in mm)
Values are presented as mean±standard deviation. No analyses were performed for implants that fractured.
Z1: zirconia implant with a modified surface, placed within the bony housing, Z2: zirconia implant without a modified surface, placed within the bony housing, T: titanium implant placed within the bony housing, Z1_D: Z1 implant placed with 3 mm of buccal bone dehiscence, T_D: titanium implant placed with 3 mm of buccal bone dehiscence, MM: mucosal margin, IS: implant shoulder, aJE: apical extension of the junctional epithelium, fBIC: first bone-to-implant contact, BC: bone crest, IS-fBIC_c: the distance between IS and fBIC, with the subtraction of 0.7 mm (zirconia implant) or 0.4 mm (titanium implant).
![]()
Table 3
Bone-to-implant contact ratio (%)
Values are presented as mean±standard deviation.
Z1: zirconia implant with a modified surface, placed within the bony housing, Z2: zirconia implant without a modified surface, placed within the bony housing, T: titanium implant placed within the bony housing, Z1_D: Z1 implant placed with 3 mm of buccal bone dehiscence, T_D: titanium implant placed with 3 mm of buccal bone dehiscence.
![]()
Peri-implant soft tissue dimensions
The mean level of the MM was located coronally relative to the IS in all groups. The mean MM-IS distance was highest in group T_D (2.53±1.91 mm) at 2 weeks, followed by groups Z2, Z1, Z1_D, and T (2.31±0.32 mm, 2.09±0.87 mm, 1.78±1.48 mm, and 1.68±0.46 mm, respectively). At 6 weeks, the mean MM-IS distance was consistent in the zirconia implant groups (Z1: 0.84±0.28 mm, Z2: 1.18±0.28 mm, Z1_D: 1.09 mm) and the titanium implant groups (T: 2.19±1.46 mm, T_D: 1.97±1.45 mm) (Table 1).
The mean length of the junctional epithelium (MM-aJE) for zirconia implants without defects at 2 weeks was 3.03±0.4 mm (Z1) and 3.31±0.4 mm (Z2), which was larger than in group T (2.12±0.61 mm). The MM-aJE values in groups Z1_D (3.27±2.25 mm) and T_D (3.27±1.24 mm) were highly scattered compared to the defect-free groups (Z1, Z2, and T). At 6 weeks, the MM-aJE values in groups Z1 (2.48±0.34 mm) and Z2 (2.47±0.46 mm) were less scattered than in the other groups and smaller than at 2 weeks. The MM-aJE in groups Z1_D, T, and T_D ranged from 2.25±1.56 mm (group T_D) to 2.90±2.12 mm (group T) (Table 1).
The mean length of the peri-implant mucosa (MM-fBIC) at 2 weeks was highest in group Z2 (5.44±1.71 mm). The corresponding dimensions were 4.21±1.17 mm and 4.80±1.31 mm in groups Z1 and Z1_D, and 3.18±0.95 and 4.47±1.06 mm in groups T and T_D, respectively. At 6 weeks, the MM-fBIC in groups Z1 (2.87±0.41 mm) and Z2 (3.21±0.53 mm) was smaller than at the 2-week time point, whereas in group T, the dimension at 6 weeks (4.13±0.62 mm) was larger than at 2 weeks. The MM-fBIC in groups Z1_D (4.3 mm) and T_D (4.5±1.37 mm) was similar at 2 and 6 weeks (Table 1).
The corrected distance between IS and fBIC (IS-fBIC_c) demonstrated minimal differences between 2 and 6 weeks in groups Z1, Z2, Z1_D, and T. However, in group T, the dimension of IS-fBIC_c was smaller at 6 weeks (2.13±0.23 mm) than at 2 weeks (2.57±0.12 mm) (Table 1).
BIC
The mean percentage of BIC at 2 weeks was comparable between groups Z1 (34.15%±21.23%) and Z1_D (29.02%±25.32%), but not between groups T (31.77%±11.73%) and T_D (9.32%±3.42%). The BIC in group Z2 (19.81%±2.03%) was lower than in groups Z1 and Z1_D (Table 3).
At 6 weeks, group Z1 demonstrated the highest BIC values (84.08%±1.33%) among all groups, followed by groups T (77.22%±4.48%), Z1_D (73.59%±4.57%), Z2 (67.26%±5.11%) and T_D (65.0%±14.61%).
Go to :
DISCUSSION
The present pilot preclinical study investigated the validity of an experimental model for assessing soft and hard tissue integration following the placement of implants with and without chronic buccal dehiscence defects. The study demonstrated that: 1) the dimensions of the peri-implant soft tissue varied depending on the implant and the healing time, 2) the level of the MM was located more apically at 6 weeks than at 2 weeks in all groups (except group T), 3) the presence of a buccal dehiscence defect did not result in a decrease in the overall soft tissue dimension between 2 and 6 weeks (groups T_D and Z1_D), 4) BIC values were highest in group Z1 at both time points, and 5) buccal dehiscence defects did not increase up to 6 weeks (i.e., there was no further bone loss), thereby supporting the use of this experimental model as a tool to study tissue integration of implants with and without buccal dehiscence defects.
Whereas the periodontium is developed during tooth eruption, the peri-implant mucosa is established during the healing period after implant placement and abutment connection. Extensive research, predominantly on titanium implants, has demonstrated that the dimensions of the peri-implant mucosa are consistent, irrespective of the type of healing (submerged/transmucosal) and the implant system [192021]. Based on an experimental model comparing titanium and zirconia dental implants over a longer healing period (range, 6–12 months), the dimension of the peri-implant tissues did not show any significant differences across implant systems and materials [914]. In the present study, different peri-implant dimensions were measured at 2 weeks depending on the implant material (titanium vs. zirconia) and the surface (Z1 vs. Z2) (Z1: 4.21±1.17 mm, Z2: 5.44±1.71 mm, T: 3.18±0.95 mm). These variations might be attributed to the early healing phase and the initial soft tissue response [22]. At 6 weeks, the peri-implant dimensions appeared to have matured more, as represented by smaller within-group standard deviations. In sites without dehiscence defects, a larger dimension was found for titanium implants (similar to previous studies [2324]) than for zirconia implants (similar to a previous study [9]).
The dimensions of the peri-implant mucosa in groups with dehiscence defects (Z1_D and T_D) were larger than in the corresponding defect-free groups (Z1 and T) at 2 weeks, indicating that the dehiscence defects were covered with soft tissue. Interestingly, these dimensions were maintained around both implant materials up to 6 weeks. Moreover, the level of the MM and the length of the junctional epithelium in groups Z1_D and T_D were not substantially different compared to the defect-free groups (Z1, Z2, and T). Clinically, small dehiscence defects are frequently encountered after implant placement due to remodeling processes following tooth extraction. Such deficiencies are traditionally treated by applying bone regenerative procedures, thereby contributing to increased patient morbidity, higher cost, and an increased treatment time. In a clinical setting, a previous study compared titanium implants with guided bone regeneration to those that underwent spontaneous healing for ≤5 mm dehiscence defects, and demonstrated no statistically significant difference in the mucosal level between the 2 groups [15]. No such data exist for zirconia implants. The similar dimensions of peri-implant mucosa in the present preclinical study at both 2 and 6 weeks may indicate that a small dehiscence defect can be left without bone augmentation. However, considering the increase of bone loss observed in a clinical trial when small dehiscence defects were left untreated around the titanium implants [15], further investigations into mucosal stability at dehiscence defects are required with a larger number of samples. Moreover, the effects of crown insertion and occlusal loading should be investigated.
The percentage of BIC is often used to assess osseointegration. A systematic review based on preclinical studies demonstrated that most of the included studies showed no statistically significant difference in terms of BIC values between zirconia and titanium implants [25]. This is in line with the present study, in which differences were predominantly observed between groups Z1 and T (34.15%±21.23% vs. 31.77%±11.73% at 2 weeks, 84.08%±1.33% vs. 77.22%±4.48% at 6 weeks). The difference in BIC values between group Z1 and Z2 was also notable. It appeared that group Z1 achieved a faster and higher osseointegration level compared to group Z2. This difference might be attributed to the differing surface characteristics of the 2 zirconia implants.
Implant fractures were found in 2 implants in group Z1_D and in one implant in group Z2, but not in any of the titanium implants. Fractures of zirconia implants were previously observed in preclinical studies using canine mandibles [910]. Both studies reported 7 zirconia implant fractures, and the most fractures were observed for one-piece implants. Interestingly, the fracture was related to a specific animal in both studies. Likewise, 2 implant fractures (2 out of 3) in the present study were found in a single dog, suggesting that the specific host can be a confounding factor.
The present study employed a chronic peri-implant dehiscence model, which is more similar to clinical circumstances than an acute model. The establishment of a bony dehiscence defect in conjunction with implant placement (acute model) might render bone healing unpredictable, thereby reducing the standardization of outcome measures. The choice of a chronic defect model is even more important if the early healing phase is considered and the peri-implant tissues are predominantly assessed at the soft tissue level. At the time of implant placement in the present study, healed ridges were present. Sequential drilling and adjusting drill angulation made it more feasible to standardize implant placement in a predictable manner with or without dehiscence defects. At 6 weeks, the values of IS-fBIC_c (the distance between the implant shoulder and the first bone-to-implant contact) were larger in the groups with defects than in the defect-free groups, thereby supporting the use of the present experimental model.
In conclusion, variations in the peri-implant mucosal dimensions were found depending on the implant material, the healing time, and the presence or absence of a dehiscence defect. Up to 6 weeks, there were minimal differences in the marginal mucosa in the presence of a dehiscence defect. A zirconia implant with a modified surface (Z1) resulted in higher BIC values than Z2. The present chronic peri-implant dehiscence model can serve as a useful experimental model to study peri-implant dehiscence defects at the hard and soft tissue levels.
Go to :
 XML Download
XML Download