

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peri-implantitis is defined as the presence of soft tissue inflammation and a loss of marginal bone around a dental implant [12]. Peri-implantitis has been found in 28%–56% of subjects, and at 12%–43% of implant sites [34]. As increasing numbers of patients are receiving dental implant restorations, the frequency of peri-implantitis will likely rise.
It is well-known that bacterial infection is the primary cause of peri-implantitis [5]. A history of periodontitis, poor oral hygiene, and irregular maintenance therapy are considered to be risk factors for peri-implantitis [678]. The biofilms involved in peri-implantitis and periodontitis have a similar composition of microbiota, which helps explain the finding that patients with active periodontal disease have a higher risk of peri-implantitis [9]. Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola have been identified as the major bacteria associated with the severity of periodontal disease, and have been together named the “red complex” [10]. A recent systematic review has provided moderate evidence supporting an association of P. gingivalis, T. denticola, and T. forsythia with the aetiology of peri-implantitis, in addition to some evidence supporting an association of Prevotella intermedia and Campylobacter rectus [11]. Hence, the treatment of peri-implantitis focuses on implant surface cleansing. Because of limited accessibility around the implant for plaque control, it is difficult to reduce the bacterial load at peri-implantitis sites by mechanical debridement alone [12]. Although local and systemic antibiotics have been proposed for the management of these problems, the use of antimicrobial agents leads to the development of bacterial resistance [13].
Photodynamic therapy (PDT), which is a new method of treating peri-implantitis and periodontitis, includes a combination of light and photosensitive agents, called photosensitisers [14]. Target bacterial cells are exposed to a photosensitiser, and irradiated with a light at the maximum absorption wavelength of the sensitiser in the presence of oxygen. This results in the production of free radicals and singlet oxygen, which are mortally toxic to bacteria. Alwaeli et al. [15] studied the effects of adjunctive PDT with scaling and root planing for more than a year. Their data demonstrated significant improvements in all evaluated clinical parameters for at least 1 year, and they suggested that PDT, as an adjunctive therapy to scaling and root planing, represented a promising therapeutic concept for persistent periodontitis.
Some bacteria do not require exogenous photosensitisers. Black-pigmented bacteria have porphyrins, which act as endogenous photosensitisers. Fukui et al. [16] evaluated the wavelength and irradiation conditions that were most effective for growth inhibition of P. gingivalis without photosensitisers. Light irradiation at 405 nm specifically suppressed the growth of P. gingivalis, suggesting that visible blue light irradiation can eradicate periodontopathogenic bacteria. Feuerstein et al. [17] also showed that broadband blue light sources, such as light-emitting diodes (LEDs) at 400–500 nm, exerted a phototoxic effect on P. gingivalis. Song et al. [18] compared the antimicrobial effects of blue light on periodontal pathogens in planktonic and biofilm cultures. Blue-light exposure was less effective against periodontal pathogens in a biofilm state than against pathogens in a planktonic state. Therefore, the use of an adjunctive exogenous photosensitiser is recommended when visible light is applied for antimicrobial periodontal therapy.
Recently, a toothbrush with a blue LED has been introduced. To the best of our knowledge, the effects of a blue LED toothbrush, in combination with erythrosine as a photosensitiser, on peri-implantitis-associated biofilms have not been previously examined. Therefore, the purpose of this study was to evaluate the antimicrobial effects of this newly devised LED toothbrush on a peri-implantitis-associated biofilm attached to sandblasted large-grit acid-etched (SLA) titanium surface.
MATERIALS AND METHODS
Titanium disk preparation
Manufactured titanium disks with an SLA surface (Shinheung, Seoul, Korea), measuring 8 mm in diameter and 2.5 mm in thickness, were used. The titanium disks were fixed with a putty-type hydrophilic vinyl polysiloxane material (GC Corporation, Tokyo, Japan) so that bacteria attached to only one side of the disks, and then the disks were autoclaved for sterilisation.
Bacterial strain and culture conditions
The bacterial strain used was P. gingivalis ATCC 33277, which is a stock laboratory strain maintained at the Department of Microbiology and Immunology, Gangneung-Wonju National University College of Dentistry. P. gingivalis was grown in trypticase soy broth (Becton, Dickinson and Company, Sparks, MD, USA) containing 5 μg/mL haemin (Sigma Chemical Co., St. Louis, MO, USA) and 1 μg/mL menadione (Sigma Chemical Co.) under anaerobic conditions in an atmosphere of 5% CO2, 5% H2, and 90% N2 for 3–4 days.
For biofilm formation, 2 mL of trypticase soy broth containing 5 μg/mL haemin and 1 μg/mL menadione was inoculated with 100 µL of a bacterial suspension in 24-well cell culture plates (Corning, Inc., Corning, NY, USA) with titanium disks. P. gingivalis was grown anaerobically for 96 hours at 37°C.
Instrumentation and quantitative evaluation of bacterial removal
The hydrophilic vinyl polysiloxane material was removed after the 96-hour incubation period. The SLA titanium disks with bacteria were divided into 5 groups of 8 disks each (Table 1), as follows: control, a commercial PDT kit (PerioWave System, Ondine Biopharma, Vancouver, Canada; Figure 1A), brushing with a toothbrush (Smart E-care, AinA, Daegu, South Korea; Figure 1B) alone (B), brushing combined with an LED light (BL), and brushing in combination with an LED light and erythrosine (BLE). The light was emitted by 2 blue LEDs (465 nm, 64 mW), 1 red LED (630 nm, 44 mW), and 1 white LED (550 nm, 64 mW). The disks in the commercial PDT-kit group were placed in methylene blue (1 mL, 100 μg/mL) for 60 seconds and then irradiated with a diode laser (670 nm, 160 mW) for 30 seconds. The disks in the B group were only brushed for 30 seconds. The disks in the BL group were brushed with an LED light for 30 seconds. Erythrosine (1 mL, 22 µM) was applied to the disks in the BLE group for 60 seconds, and the disks were then brushed with an LED light for 30 seconds. After treatment, the disks were placed in a test tube and vortexed with 3 mL of phosphate-buffered saline (PBS) and glass beads (0.15 mm in diameter, Daihan Scientific, Wonju, Korea) for 60 seconds. The suspension of detached bacterial cells was spread on trypticase soy agar plates containing 1 mg/mL yeast extract, 1 μg/mL menadione, 5 μg/mL haemin, 5% sheep blood (Hanil-KOMED, Seongnam, Korea), and 1.5% Bacto® Agar (Becton, Dickinson and Company) using a spiral plate system (IUL, Barcelona, Spain). The plates were incubated anaerobically for 96 hours at 37°C. An automated counter (IUL) was used to count the number of colony-forming units (CFUs). The percentage of surviving bacteria was calculated by dividing the CFU value on the test-group disks by the CFU value on the untreated control-group disks.
Table 1
Treatment protocol

PDT: photodynamic therapy, B: brush alone, BL: brushing with a LED light, BLE: brushing with a LED light and erythrosine, LED: light-emitting diode.
![]()

Scanning electron microscopy (SEM)
SEM was performed to visualise the number of remaining bacteria and the morphological changes that may have occurred in the bacterial cell walls. An additional disk was prepared for each group, and rinsed twice with 1 mL of PBS. A solution of 2.5% glutaraldehyde was used to fix the disks at room temperature for 1 hour, followed by specimen dehydration using a standard graded series of ethanol solutions including 70% and 90% ethanol for 60 minutes per step, and ending with 5 changes of 100% ethanol for 30 seconds each. After critical point drying, the disks were mounted on a stub, coated with gold, and observed with SEM. The surfaces of the disks were observed using variable-pressure field-emission SEM (SUPRA55VP, Carl Zeiss, Oberkochen, Germany).
RESULTS
Antimicrobial effects
The mean counts of viable bacteria and percentages of bacterial reduction are presented in Table 2. The control group showed a significantly higher log CFU/mL value than the PDT, BL, and BLE groups (P<0.05). The number of viable bacteria was significantly lower in the BLE group than in the other groups (P<0.05). The values in the control and B groups were not significantly different (P>0.05). Compared with the control group, the bacterial reduction rate was 52.9%, 49.4%, 62.7%, and 75.6% in the PDT, B, BL, and BLE groups, respectively. Statistically significant differences were found among the treated groups, with the BLE group demonstrating the greatest antibacterial effects.
Table 2
Counts of viable bacteria and percentages of bacterial reduction on the SLA surface of titanium in different treatment groups

| Group | Log CFU/mL (mean±SD) | Bacterial reduction (%) |
|---|---|---|
| Control | 7.49±0.10a) | - |
| PDT | 7.04±0.44b) | 52.9 |
| B | 7.16±0.23a,b) | 49.4 |
| BL | 7.04±0.18b) | 62.7 |
| BLE | 6.60±0.66c) | 75.6 |
SLA: sandblasted large-grit acid-etched, CFU: colony-forming unit, SD: standard deviation, PDT: photodynamic therapy, B: brush alone, BL: brushing with a LED light, BLE: brushing with a LED light and erythrosine.
a,b,c)Different superscript letters indicate significant differences (P<0.05).
![]()
SEM
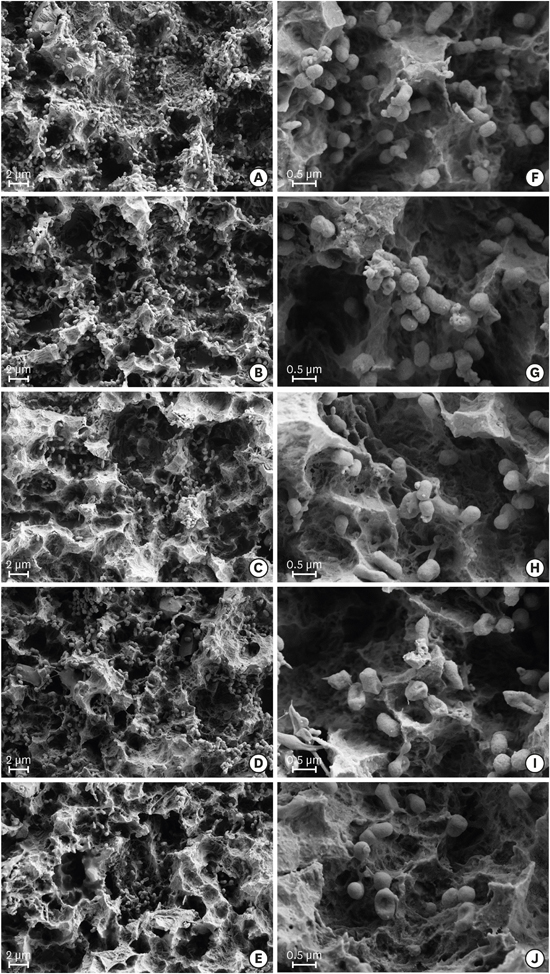
Representative SEM images of bacterial cells on the SLA titanium surfaces are shown in Figure 2. Most of the titanium surfaces were covered with bacterial cells, and titanium surface alterations from the treatments were not observed (Figure 2). The B, BL, and BLE groups (Figure 2C-E) showed fewer surface-attached bacterial cells than did the control and PDT groups (Figure 2A and B). The control and B groups (Figure 2F and H) showed intact bacterial morphology. In contrast, the outer cell walls of the bacteria in the PDT, BL, and BLE groups were damaged (Figure 2G, I, and J).
 | Figure 2Scanning electron microscopy images of Porphyromonas gingivalis cells attached to the sandblasted large-grit acid-etched surface: (A, F) control group; (B, G) photodynamic therapy group; (C, H) brush alone group; (D, I) brushing with a LED light group; (E, J) brushing with a LED light and erythrosine group.LED: light-emitting diode.
|
DISCUSSION
This study was designed to evaluate the efficacy of a LED toothbrush on a biofilm associated with peri-implant disease attached to an SLA titanium surface in vitro. Currently, an SLA surface is considered the standard for titanium implants, although several studies have found that rough surfaces facilitated bacterial biofilm formation [1920]. Berglundh et al. [21] studied the influence of implant surfaces on the progression of experimental peri-implantitis and found that the progression was more severe on SLA surfaces than on machined ones.
Peri-implantitis induces marginal bone loss and gingival recession, which increases the exposure of the fixture surface. The fixture surface is threaded, and is thus hard to clean with conventional instruments such as a metal curette or ultrasonic scaler. To overcome this problem, air-powder polishing devices and a rotating titanium brush have been devised, which seem to be effective [22]. However, few instruments are available for patient-administered mechanical plaque control of implants. The use of a powered toothbrush, adjunctive antiseptic rinse, and irrigation has been evaluated, but the data on their efficacy are not definitive [23]. Therefore, a need for the development of new instruments has emerged, and an LED toothbrush has been invented to fill this need.
Brushing is essential for oral hygiene management. Park et al. [24] evaluated the effects of brushing on the efficiency of bacterial removal. After resorbable blasting media titanium disks were incubated with P. gingivalis for 2 days, brushing was performed with a dentifrice for a total of 40 seconds, which significantly reduced the amount of bacterial adherence. However, SEM images showed that there were some bacteria remaining, residing in pits on the titanium surface.
In this study, SEM images from all the groups that included brushing showed decreased numbers of bacteria on the SLA titanium disks (Figure 2C-E). The percentage of bacterial reduction was 49.4% in the B group. However, the B group did not show a significant difference from the control group. In this study, an SLA surface was used, which is rougher than a resorbable blasting media surface. Moreover, we did not use a dentifrice, as it could affect the experimental data.
Brushing an SLA surface can provide an additional advantage. Park et al. [25] examined the effects of brushing with a dentifrice on an SLA titanium surface, which may facilitate smoothing of the surface. The authors recommended that meticulous oral hygiene with brushing must be reinforced for patients with dental implants for them to maintain a clean exposed implant surface.
The LED toothbrush uses PDT to kill additional bacteria, and PDT has been used for the treatment of peri-implantitis. Deppe et al. [26] assessed the efficacy of nonsurgical PDT for moderate versus severe peri-implantitis bony defects. They concluded that nonsurgical PDT could stop bone resorption in moderate peri-implantitis defects, but not in severe defects.
In our study, application of a toothbrush with LEDs and a commercial PDT kit showed significant antimicrobial effects on the biofilms formed on SLA surfaces; the percentages of bacterial reduction were 52.9% in the PDT group, 62.7% in the BL group, and 75.6% in the BLE group (Table 2). The SEM examination revealed morphological alterations of the bacteria in the PDT, BL, and BLE groups (Figure 2G, I, and J), which seemed to be due to the bacteria-killing effects of the 2 blue LEDs (465 nm, 64 mW) and the commercial PDT kit.
P. gingivalis uses external haem as an iron source for growth [27]. Therefore, these bacteria accumulate a black pigment on the cell surface, which mainly consists of iron protoporphyrin IX. This endogenous porphyrin can act as a photosensitiser [28]. Porphyrins exhibit an intense absorbance peak at around 405 nm, followed by several weaker peaks at 505, 540, 575, and 630 nm [29]. This specific wavelength of light causes excitation of protoporphyrin IX. The wavelength of the blue LED (465 nm) matched the maximum absorption wavelength of porphyrin. Fukui et al. [16] showed a significant inhibition of bacterial growth after only 1 minute of blue light irradiation (405 nm, 50 mW). Soukos et al. [30] likewise reported that application of blue light twice daily for 2 minutes (455 nm, 70 mW) over a period of 4 days suppressed natural intraoral biofilm formation.
The use of an LED toothbrush with erythrosine treatment resulted in a greater number of killed bacteria than did the use of an LED toothbrush alone (Table 2). Habiboallah et al. [31] studied the photodynamic killing effect of visible blue light in the presence of erythrosine as a photosensitiser on P. gingivalis. Exposure to visible blue LED light (440–480 nm, 570 mW), in combination with erythrosine, significantly reduced the viability of the bacteria. The wavelength of blue light does not exactly match the maximum absorption wavelength of erythrosine (525 nm) [32]. However, erythrosine has been used as an oral plaque-visualising agent, and white light (500–550 nm, 22.7 mW) used with erythrosine showed an antimicrobial effect on Streptococcus mutans [33]. The toothbrush used in our study also had a white LED, which was expected to kill S. mutans. The red LED, also embedded in this toothbrush, may help heal oral wounds. Fekrazad et al. [34] compared the effects of red (630 nm), green (532 nm), and blue (425 nm) lasers in terms of accelerating oral wound healing in diabetic rats. Wound healing occurred faster with the red laser than with the blue or green lasers.
It can be concluded that the combination of a blue LED toothbrush and erythrosine was effective against peri-implantitis-associated biofilms attached to a titanium surface. Because tooth brushing is performed 1–3 times a day, an LED toothbrush can be used as an instrument for patient-administered mechanical plaque control of an exposed implant fixture. Based on the findings of the current study, we conclude that the combination of erythrosine and an LED toothbrush was more effective than a commercial PDT kit in reducing the number of P. gingivalis cells attached to an SLA titanium surface in vitro. Based on the SEM images, irradiation with LED light from a toothbrush induced destruction of the cell wall of P. gingivalis, a bacterial strain associated with peri-implantitis. This LED toothbrush may help control bacteria around exposed dental implants.
 XML Download
XML Download