

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Implant-supported restoration has a high success rate over long-term follow-up periods. It has now been recognized as a predictable and reliable treatment option for replacing missing teeth [1]. However, biological complications, including peri-implant diseases (i.e., peri-implant mucositis and peri-implantitis), along with technical complications, have emerged as follow-up periods have been extended [23]. Peri-implantitis was first defined as “inflammatory reactions with loss of supporting bone in the tissues surrounding a functioning implant” [4]. The outcomes of various treatment approaches for peri-implantitis are not always successful or predictable [5]. Moreover, alveolar bone defects around the implant destroyed by peri-implantitis cannot be regenerated in a reliable and predictable way, although various efforts to do so have been made over the last few decades [6]. Hence, prevention of peri-mucositis, the precursor of peri-implantitis, has been suggested as the best approach to treat peri-implantitis [7]. If an infection of supporting tissues around the implant cannot be properly controlled, it will eventually result in loss of the implant [8]. According to another opinion, the significance of peri-implantitis is over-exaggerated. It has been suggested that most implants can function properly over long-term periods since bone loss around the implant does not continue in most cases [9].
As reported in a recent meta-analysis, the prevalence of peri-implantitis in different population samples ranges widely, from 0.4% to 36.6% at the implant level and from 1.0% to 47.1% at the patient level [10]. Different case definitions for peri-implantitis and different population samples in terms of regions and clinical settings across studies are thought to be reasons for the wide ranges of peri-implantitis prevalence rates [1011]. In relation to population samples, ethnicity might affect the prevalence of peri-implantitis because the prevalence of periodontitis has been shown to be high in certain ethnic groups [12]. However, no up-to-date information is available about the prevalence of peri-implantitis in the Korean population.
Various risk factors for peri-implantitis have been evaluated in the literature [13]. They are mainly categorized as implant- or patient-related factors and as systemic or local factors [14]. Implant surface design, implant position and angulation, and prosthesis design in terms of performing plaque control have been suggested as implant-related/local factors [14] while a history of periodontitis and smoking are the most frequently analyzed patient-related/systemic factors associated with peri-implantitis [1516]. Like supportive periodontal therapy (SPT) for the prevention of recurrent periodontal disease, regular maintenance therapy after implant placement has been emphasized as a way to prevent peri-implantitis [17]. However, the prevalence of peri-implantitis in patients with a history of periodontal disease has not been evaluated in relation to SPT. Therefore, the aim of this study was to analyze the prevalence and risk indicators for peri-implantitis in Korean patients with a history of periodontal disease.
MATERIALS AND METHODS
Patient sample
The patients included in this study were retrospectively recruited from those who had been treated at the Department of Periodontology, Chonbuk National University Dental Hospital, Jeonju, Korea. These patients underwent clinical and radiographic examinations for the diagnosis of periodontal disease at their first visit. Periodontal treatment consisting of non-surgical and surgical therapy was provided according to the severity of periodontal disease. After active periodontal treatment was completed, patients underwent SPT over the course of 3 to 6 months. From all patients who had been treated between July 2014 and June 2015, those with implant-supported restorations were selected for this study. A total of 444 patients (219 females and 225 males) with 1,485 implants were selected. The records of these patients were scrutinized to extract clinical and radiographic data related to implant-supported restorations. After screening the available radiographs of the implants, 370 patients (183 females and 187 males) with 1,189 implants were chosen for the group with a history of peri-implantitis (HP). The mean age of those subjects was 58.4 years (range, 28–88 years). The follow-up period after loading of the implant was an average of 5.9 years (range, 0.2–19.1 years) (Table 1).
Table 1
Patient-related risk variables for peri-implantitis
![]()
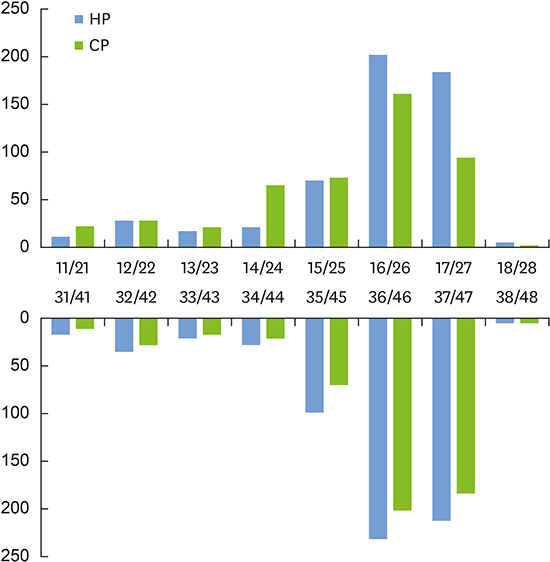
From the HP group, 318 patients (156 females and 162 males) with 1,004 implants were chosen for the current peri-implantitis (CP) group if they had additional clinical data (i.e., pocket depth and bleeding on probing at the implant) (Figure 1). The mean age of this group was 58.1 years (range, 28–83 years). The follow-up period of the implant was an average of 5.7 years (range, 0.2–19.1 years) (Table 1). Most implants in both peri-implantitis groups were placed in the posterior region (Figure 2).


Case definitions of peri-implantitis
Standardized radiographs with the film (Kodak Ektaspeed Plus, Eastman Kodak Co., Rochester, NY, USA) kept parallel and the X-ray beam (Heliodent MD, 60 kV, 7 mA, Siemens AG, Bensheim, Germany) kept perpendicular to the implant were taken at follow-up examinations. Bone level at the implant was assessed as the vertical distance between the bone level at the time of implant placement and the level of bone-to-implant contact. It was measured at the mesial and distal aspect of the implant by the thread pitch. The width of the thread pitch was obtained from the manufacturers' manuals or calculated by dividing the known implant length by the number of threads. An implant with a bone level of more than 3 thread pitches in most cases (2.4–2.5 mm) was considered to indicate peri-implantitis affecting the implant in the HP group. In addition to the radiographic assessment, clinical assessments were performed at follow-up examinations. Probing pocket depth (measured to the nearest 0.5 mm) of more than 5 mm with the presence of bleeding on probing following probing at the corresponding site of the implant were used as criteria to define peri-implantitis in the CP group.
One calibrated examiner (M-SG) who was not involved in the treatment of patients performed all assessments included in the study.
Approval of the original study protocol was obtained from the Institutional Review Board of Chonbuk National University Hospital, Jeonju, Korea (IRB No. CUH 2016-08-029). This study was performed in accordance with the 1975 Declaration of Helsinki, which was revised in 2013.
Variables associated with peri-implantitis
The patient-related risk variables included age, gender (male/female), smoking (yes/no), medical conditions (healthy/compromised), SPT (yes/no), and implant number per patient. The implant-related risk variables included 3 continuous variables (follow-up period after implant loading, implant diameter, and implant length) and 4 binary variables: prosthesis type (single implant-supported restoration or fixed dental prosthesis [FDP]), implant position (maxilla/mandible, non-molar/molar), bone graft (yes/no), and treatment setting (university hospital/private clinic). In addition, the patients were asked to comment on whether they had felt discomfort around the implant as a measure of subjective discomfort (yes/no).
Data analysis
Mean values, frequencies, standard deviations, and ranges of variables were used for data description, with subject and implant as statistical units. The prevalence of peri-implantitis was calculated at the patient and implant levels. To analyze potential variables associated with peri-implantitis, the generalized estimating equations (GEEs) procedure was utilized because of the cluster-correlated data that each patient provided due to having a different number of implants (1–16 implants) [18]. The influence of patient- and implant-related variables on the occurrence of peri-implantitis was reported as odds ratios (ORs) with 95% confidence intervals (CIs) using GEE univariate analyses. The cumulative peri-implantitis rate during the follow-up period was estimated with the Kaplan-Meier method. Data analysis was performed using Stata® 13 statistical software program (Stata Corp., College Station, TX, USA). P values <0.05 were considered to indicate statistical significance in all analyses.
RESULTS
The descriptive characteristics of peri-implantitis in relation to patient- and implant-related variables are shown in Tables 1 and 2. The prevalence of peri-implantitis calculated at the patient and implant levels ranged from 6.7% to 19.7% in the HP and CP groups (Table 3).
Table 2
Implant-related variables associated with peri-implantitis

HP: history of peri-implantitis, CP: current peri-implantitis, NA: not available, FDP: fixed dental prosthesis.
![]()
Table 3
Prevalence of peri-implantitis at the patient and implant levels in groups with a HP and CP

![]()
Among the patient-related risk variables included in the univariate GEE analysis, whether patients received SPT was the only significant indicator of the occurrence of peri-implantitis in both the HP and CP groups (Table 4). Patients not receiving SPT showed 2.8 and 6.1 times higher chances of having peri-implantitis in the HP and CP groups, respectively.
Table 4
ORs, 95% CIs, and P values for patient-related risk variables associated with the occurrence of peri-implantitis assessed by GEEs analysis

OR: odds ratio, CI: confidence interval, GEE: generalized estimating equation, HP: history of peri-implantitis, CP: current peri-implantitis, SPT: supportive periodontal therapy.
![]()
In the univariate GEE analysis of implant-related variables as risk indicators for peri-implantitis, implants supporting FDPs and implants with subjective discomfort were associated with a higher prevalence of peri-implantitis than single implants and implants without subjective discomfort in the HP group. The presence of subjective discomfort was the only implant-related variable significantly associated with peri-implantitis in the CP group (OR, 14.4; P<0.05) (Table 5).
Table 5
ORs, 95% CIs, and P values for implant-related variables associated with the occurrence of peri-implantitis assessed by GEEs analysis

OR: odds ratio, CI: confidence interval, GEE: generalized estimating equation, HP: history of peri-implantitis, CP: current peri-implantitis, FDP: fixed dental prosthesis.
![]()
The cumulative peri-implantitis rate in the HP group estimated with the Kaplan-Meier method was higher than that in the CP group over the follow-up period (Figure 3). In the CP group, the cumulative peri-implantitis rate in patients who did not receive SPT showed a steeper increase than in patients who did receive SPT over the follow-up period (Figure 4).
DISCUSSION
The prevalence of peri-implantitis in Korean patients with a history of periodontal disease was 6.7% at the implant level and 13.2% at the patient level in the CP group. It was 10.3% at the implant level and 19.7% at the patient level in the HP group (Table 3). To the best of our knowledge, this study is the first to report the prevalence of peri-implantitis in a Korean population. The prevalence of peri-implantitis in the CP group was similar to that reported in other studies [10]. It should be kept in mind that all patients in the present study had been treated for periodontal disease, and that almost half of these patients received SPT after completing active periodontal treatment. However, the remaining half of the patients did not receive SPT after completing periodontal treatment or were still receiving active periodontal treatment. Hence, the prevalence of peri-implantitis in the present study should be interpreted in consideration of the fact that patients with a history of periodontitis showed a higher prevalence of peri-implantitis than periodontally healthy patients [1617].
The cumulative peri-implantitis rate in the HP group estimated with the Kaplan-Meier method was higher than that in the CP group throughout the follow-up period (Figure 3). The difference in the cumulative peri-implantitis rate between the HP and CP groups in the present study could be attributed to the selection process of the peri-implantitis groups. Most studies reporting the prevalence of peri-implantitis have used clinical assessments, including probing pocket depth and bleeding on probing, in addition to the radiographic assessment of bone loss at the implant to define cases of peri-implantitis, as in the CP group [10]. Due to the retrospective design of this study, not all implants that were included had clinical data for the implant. Therefore, implants showing obvious bone loss above the threshold used to define a case (bone loss >2.4 mm) were defined as impacts affected by peri-implantitis in the HP group. The peri-implantitis lesions of some patients in the HP group might have already been treated, and consequently the clinical signs of peri-implantitis were not observed at follow-up. This might why the prevalence of peri-implantitis in the HP group was greater than in the CP group.
The cumulative peri-implantitis rate estimated with the Kaplan-Meier method increased in an irregular pattern during the follow-up period (Figures 3 and 4). This finding is in accordance with a recent study showing a non-linear, accelerating pattern of bone loss at implants affected by peri-implantitis [8]. However, according to a different opinion, early bone loss caused by peri-implantitis can transition into a long-lasting state of bone stability, with only a few implants showing extensive bone resorption [19].
In comparison to patients receiving regular SPT, patients not receiving SPT showed 2.8 and 6.1 times higher chances of peri-implantitis in the HP and CP groups, respectively (Table 4). Furthermore, in the CP group, the prevalence of peri-implantitis in patients not receiving SPT showed a steeper increase than in patients with SPT over the follow-up period (Figure 4). In a recent meta-analysis that evaluated the influence of peri-implant maintenance therapy (PIMT) on peri-implant diseases, a minimum duration of 5 to 6 months for PIMT has been suggested to prevent peri-implantitis [17]. In addition, the incidence of implant loss was found to be significantly lower in patients who underwent a strict maintenance program compared to patients who did not [1720]. As mentioned earlier, almost half of the patients in the present study received SPT after completing active treatment, while the remaining patients did not receive SPT or were still receiving active periodontal treatment. Hence, patients not receiving SPT might be more susceptible to peri-implantitis due to the lack of regular SPT and untreated periodontal disease.
The univariate GEE analysis of implant-related risk variables in the HP group revealed that implants supporting FDP showed higher prevalence of peri-implantitis than single implants (OR, 1.93; P=0.018). The case definition for peri-implantitis in the HP group was based on the amount of peri-implant bone loss. Hence, the presence of adjacent natural teeth in single implants seemed to have positive influence on the bone level of the tooth-facing surface at single implants in comparison with the implant-facing surface of implants supporting FDP [21]. In addition, the narrow inter-implant distance between implants supporting FDP might result in bone loss due to difficulties in cleaning a small embrasure space [2223].
Implants with subjective discomfort showed a higher prevalence of peri-implantitis than those without subjective discomfort in the HP group (OR, 9.4; P<0.05) and the CP group (OR, 14.4; P<0.05) (Table 5). It is recommended to assess patient-based outcomes in clinical studies because patient-oriented evidence can improve the quality of studies [24]. Moreover, self-reported patient-related measures have been shown to perform well in certain populations, even though their precision for diagnosing the severity of periodontal disease varies across populations and self-reported measures [2526]. In the present study, a patient-reported measure (i.e., subjective discomfort, including pain, swelling, and pus discharge) was shown to be a strong indicator of peri-implantitis. In corroboration with this result, it has been suggested that the treatment of peri-implantitis should only be initiated when a clinical problem is present based on patient's symptoms. The treatment should aim to resolve infection, including removal of the implant [27].
Currently, no universal criteria for defining cases of peri-implantitis exist in relation to the amount of peri-implant bone loss. The prevalence of peri-implantitis ranges from 1% with a threshold of 5 mm of bone loss to 47% with a threshold of 0.4 mm of bone loss [2829]. It has been recommended that the amount of bone loss at the implant should be assessed from the baseline (i.e., loading of the implant-supported restoration) to the follow-up examination [10]. However, a threshold vertical distance from the expected marginal bone level following re-modeling after implant placement was utilized as an alternative, because radiographs at baseline were unavailable for the majority of patients in the present study due to its retrospective design [30]. Additionally, the bone level of the implant at the follow-up examination was assessed based on the pitch thread number in order to calibrate the distortion of radiographs for the convenience of measurement.
The mean follow-up period of implants in the present study was 5.9 years. It ranged widely, from 2 months to 19 years. However, the follow-up period did not significantly influence the occurrence of peri-implantitis in the univariate GEE analysis. Similarly, a recent study showed that the onset of peri-implantitis occurred mostly within 3 years of function, following a nonlinear accelerating pattern in patients with moderate or severe peri-implantitis over a 9-year period [8]. However, it is recommended that implants with a function time of more than 5 years should be included in studies analyzing the prevalence of peri-implantitis [11].
To overcome the risk of selection bias and limitations in external validity, large randomly selected population samples are needed to study the prevalence of peri-implant diseases [11]. In the present study, a convenience sample was selected from patients with periodontal disease who had been treated at the specialist clinic of a university hospital during a limited period. In addition, patients' implant-supported restorations were placed either at a private clinic or the university hospital. Hence, some implant-related risk variables, such as implant diameter, implant length, and bone graft, were not available for patients whose implants were placed at a private clinic. Although the prevalence of peri-implantitis between the 2 groups according to clinical setting was not significantly different, the prevalence of peri-implantitis in the present study should be cautiously interpreted when comparing it to results obtained from large randomly selected population samples. Furthermore, it should be emphasized that all patients in this study had been treated for periodontal disease, because the aim of this study was to evaluate the prevalence of peri-implantitis in patients with a history of periodontal disease.
To analyze the prevalence of peri-implantitis in future studies, consistent case definitions for peri-implantitis should be applied to large randomly selected population samples with adequate size and function time [1011].
Within the limitations of this study, it can be concluded that the prevalence of peri-implantitis in Korean patients with a history of periodontal disease was similar to that in other population samples. To prevent peri-implantitis, regular SPT is important. Single implants were found to be less susceptible to peri-implantitis than implants supporting FDP. Patients' subjective discomfort was found to be a strong risk indicator for peri-implantitis.
 XML Download
XML Download