

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
After tooth extraction, various techniques are used to remodel soft and hard tissue, which may lead to a reduced alveolar ridge contour [12]. The resorption processes that are responsible for dimensional changes following tooth extraction have been evaluated in previous studies [345]. Clinically, most of the resorption occurs during the first 3 months of healing, and this may reduce the buccolingual dimension of the alveolar ridge by approximately 50% [6]. Araújo and Lindhe [3] reported that the reduction of the buccal wall was more pronounced than that of the lingual wall because buccal bone is mostly comprised of bundle bone that loses its function after tooth removal and is resorbed by osteoclasts. These hard tissue alterations may significantly limit implant placement if additional bone grafting is not performed and may impair the aesthetic outcome of a prosthesis due to horizontal or vertical ridge deficiencies.
Ridge preservation techniques are designed to minimize dimensional changes of the edentulous ridge after tooth loss. Numerous surgical techniques involving a variety of bone grafts, barrier membranes, and soft tissue have been evaluated. However, none of the tested treatments completely preserved the buccal bone plate after tooth loss [789]. In contrast, placing biomaterials in the extraction sockets has been found to promote bone remodeling and to partially compensate for the ridge resorption in an animal model [10]. A technique involving both bone grafting and a resorbable membrane has shown the most favorable results, with the possibility for implant placement to occur between 4 and 6 months following a ridge preservation procedure [1112].
Covering the orifice of the extraction socket with a free gingival graft or membrane may reduce postoperative external contour shrinkage [13]. Using a manufactured barrier membrane is more convenient than using a soft tissue graft because a donor site is not required. The use of an occlusal membrane for a ridge preservation procedure also prevents particle loss and the migration of epithelial and connective tissue cells into the defect area [14].
The ideal barrier membrane should exhibit characteristics such as biocompatibility, dimensional stability, tissue integration at the defect site, and a barrier function that prevents soft tissue ingrowth [15]. Ensuring the correct time for resorption of the barrier membrane is also important, since resorption before new bone formation may cause loss of dimensional stability, dissipation of bone substitute, and impaired healing at the defect site. In addition, delayed resorption may cause poor healing due to the remainder of a non-functional barrier membrane. Most collagen membranes currently available in dental clinics are made with type I and type III collagen that are derived from porcine or bovine collagen. A chemically cross-linked collagen membrane seems to be safe and effective for controlling resorption time [16]. However, certain cross-linking chemical agents can induce unwanted inflammation and foreign-body reactions [17]. Therefore, as long as the resorption time can be controlled, a membrane without a chemical cross-linking agent may heal more favorably.
A new extracellular matrix (ECM)-based resorbable membrane (Lyso-Gide, Oscotec Inc., Seongnam, Korea) has been recently introduced. This membrane is derived from porcine pericardium, and its bilayer structure makes it particularly suitable for the guided bone regeneration procedure. The upper layer, which is very thin (<0.1 mm), has a high density and can act as a barrier to tissue invasion, while the bottom layer (>0.2 mm) has a microporous structure and can provide spaces for osteoblast homing. This membrane has a natural cross-linking structure that avoids the need for any additional cross-linking process [18].
The aim of this study was to radiographically and clinically compare the impact of ECM membranes on dimensional alterations of the alveolar ridge. A widely used ECM membrane (WEM; Bio-Gide, Geistlich Biomaterials, Wolhusen, Switzerland) and the newly developed ECM membrane (NEM) that was treated with acellular lyophilized porcine pericardium were applied during ridge preservation procedures in the control and treatment group, respectively.
MATERIALS AND METHODS
Study design
This study was a prospective, double-blind, controlled, randomized clinical investigation conducted in accordance with the Helsinki Protocol. The study protocol was approved by the Institutional Review Board at Seoul National University Dental Hospital (approval No. CGE14001) and registered as a clinical trial (http://cris.nih.go.kr, approval No. KCT0001815). The guidelines for reporting a randomized controlled trial according to the Consolidated Standards of Reporting Trials were followed. Informed consent was obtained from all patients prior to the commencement of the study. Block randomization with numbered containers was used to randomly assign treatment protocols.
Participants
A total of 66 patients who were admitted for tooth extraction to the Department of Periodontology or the Department of Oral and Maxillofacial Surgery at Seoul National University Dental Hospital in Seoul, Korea were enrolled in the study. Patients were recruited between April 2015 and September 2016. A total of 22 patients dropped out during screening, and 2 patients dropped out during the follow-up period (Figure 1).
 | Figure 1Flow diagram for the phases of the randomized controlled trial.
CBCT: cone-beam computed tomography, VAS: visual analog scale.
|
A ridge preservation procedure was performed in 42 patients. This included 22 men and 20 women who had a mean age of 60.3 years (range, 41–78 years). The patients were randomly assigned to the control group (n=21) or the treatment group (n=21). Their general characteristics are listed in Table 1. Only patients older than 20 years were included in this study. The indications for tooth extraction included dental caries, tooth fracture, and chronic periodontitis (loss of clinical attachment of more than 5 mm or degree 3 mobility).
Table 1
General characteristics of subjects

Values are presented as mean (standard deviation) or number (%).
a)Using the parametric independent t-test; b)Using the Pearson χ2 test.
![]()
Patients were excluded if they had any of the following conditions: 1) uncontrolled hypertension or diabetes mellitus; 2) history of malignant bone tumor; 3) severe cardiovascular disease, respiratory disease, kidney disease, liver disease, digestive disease, blood disease, nerve disease, or mental disease; 4) hyperthyroidism or hypothyroidism; 5) history of drug allergy; 6) severe depression or anxiety disorder; or 7) alcohol abuse within the previous year. Patients who were considered inappropriate by the researchers were also excluded.
Treatment
Four periodontists performed all of the ridge preservation procedures. The specialists were trained for a minimum of 10 hours by practicing the procedure under the same conditions to ensure that the study was highly reproducible. The tooth was carefully removed, and the inner granulation tissue was carefully eliminated with curettes. In both the treatment and control groups, deproteinized bovine bone mineral collagen (Bio-Oss Collagen, Geistlich Biomaterials) was placed in the fresh socket without flap elevation. The NEM and the WEM were applied in the treatment group and the control group, respectively, in a double-blind manner. The membrane was stabilized with 4-0 vicryl sutures (Ethicon, Somerville, NJ, USA). Amoxicillin or cefdinir was prescribed as antibiotics for 5 days. The sutures were removed after 7 to 10 days, and signs of complications were checked. Cone-beam computed tomography (CBCT) scans (Dinnova 3, HDX Corp., Seoul, Korea) were obtained (scan time of 7 seconds at 120 kV and 10 mA) before surgery, on the day of surgery, and 6 months after the ridge preservation procedure.
Evaluation of dimensional changes
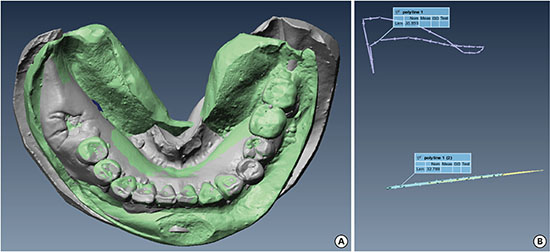
Master casts of each patient were made with dental stone (GC Fujirock EP, GC Corp., Tokyo, Japan) utilizing alginate impressions at 1 week and 6 months after the ridge preservation procedure. Computer-aided design software (DentalCAD, EGS, San Lazzaro, Italy) and an optical scanner (DScan version 1.1, EGS) were used to scan the casts.
The 1-week cast scans were matched with the corresponding 6-month cast scans using digital imaging software (Polyworks, Innovmetric, Quebec, Canada). The different scans were superimposed while using adjacent teeth as references to ensure precise alignment. A region of interest (ROI) was set in the scan of the 1-week cast from the upper-middle region of the gingiva to the mucogingival junction. The average surface vector was calculated for the ROI, and, afterwards, the ROI was projected onto a plane that was perpendicular to the average surface vector. Projections were made onto the scans of the 1-week and 6-month casts. Volumetric measurements were performed in the ROI and the projected area. The volumetric change was divided by the area of the projection and quantified as the displacement between the surfaces (Figure 2).

Quantity of bone tissue
Raw CBCT scans obtained on the day of surgery and 6 months after the ridge preservation procedure were merged and then resliced at a resolution of 0.3 mm using a software program (OnDemand3D, Cybermed Inc., Daejeon, Korea). The segmentation range of both scans was set to be equal. The 3-dimensional (3D) shape of the ridge preservation site was developed and the quantity of bone tissue was measured using the OnDemand3D program. The quantity of the initial total graft (Q2) was measured in a CBCT scan obtained on the day of surgery (V2). The quantity of mineralized new bone and residual graft (Q6) was also measured using CBCT 6 months after the ridge preservation procedure (V6). The performance of a membrane as a barrier was quantified as Q6/Q2×100.
Width and height changes
Changes in the width and height at the center of the extraction socket were evaluated in merged axial and sagittal views of V2 and V6 CBCT images using the OnDemand3D program (Figure 3).

Data analysis
A power calculation before the study commenced revealed that a sample size of 23 was needed to detect a 6 mm3 difference in ridge volume after 6 months, assuming a maximum standard deviation of 7.68 mm3, 80% power, a 0.05 cutoff for significance, and an increase in the sample size by 10% due to drop-out.
The primary outcome variables were dimensional changes in the residual ridge and quantity of bone tissue. The secondary outcome variables were changes in width and height.
The height conformed to a normal distribution (Shapiro-Wilk test, P>0.050), while the distributions of the dimensional change in the residual ridge, the quantity of bone tissue, and width did not (Shapiro-Wilk test, P<0.050). Gender, jaw position, and right/left proportions in the treatment and control groups were compared using the Pearson χ2 test.
Due to the characteristics of the distributions, the independent t-test was performed to compare differences in age and height between the treatment and control groups, while the nonparametric Mann-Whitney U test was performed to compare the difference in dimensional changes in the residual ridge, the quantity of mineralized tissue, and the width. SPSS version 23.0 (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, USA) was used for the analysis, and a significance cutoff of 0.05 was used for the type 1 error rate.
RESULTS
Evaluation of dimensional changes
The results for the dimensional changes in master casts are displayed in Table 2. The mean dimensional difference between the 1-week and 6-month casts was −0.98 mm in the treatment group and −1.01 mm in the control group (P≥0.050). The cast volume was lower at 6 months than at 1 week in both the treatment and control groups.
Table 2
Clinical and radiographic dimensional changes

Values are presented as mean (standard deviation).
CBCT: cone-beam computed tomography.
a)Using the parametric independent t-test; b)Using the nonparametric Mann-Whitney U test.
![]()
Quantity of bone tissue in CBCT
The results for the normalized quantity of bone tissue (Q6/Q2) in the CBCT data are presented in Table 2. The mean percentage was 91.6% in the treatment group and 91.5% in the control group (P≥0.050). There was less quantity of bone tissue at 6 months than at 1 week in both the treatment and control groups.
Changes in width and height in CBCT
The changes in the width of the center of the extraction socket in CBCT data are displayed in Table 2. The mean difference in width between the V2 and V6 images was −1.7 mm in the treatment group and −2.1 mm in the control group (P≥0.050).
The changes in the height of the extraction socket in CBCT data are shown in Table 2. The mean difference in height between the V2 and V6 images was −2.1 mm in the treatment group and −2.2 mm in the control group (P≥0.050).
DISCUSSION
Ridge preservation using a bone graft and resorbable membrane has been shown to improve ridge height and width dimensions more than tooth extraction alone [14]. The present randomized controlled trial compared the effectiveness of different membranes used for ridge preservation. Neither of the membranes could prevent ridge resorption entirely after tooth loss. This investigation found no significant differences between the treatment and control groups in changes in volume, width, or height of the extraction socket.
The volumetric change of the extraction socket in the master cast did not differ significantly between the treatment and control groups. This indicates that both types of membranes were equally useful in preventing the collapse of the socket volume during a ridge preservation procedure. Both membranes seemed to last long enough to prevent dissipation of bone graft particles and soft tissue growth into the extraction socket. The decrease in bone quantity in the study cast and CBCT from 1 week to 6 months was similar between the treatment and control groups, and the decrease was consistent with the results of previous studies [1319].
The clinicians determined that the membrane characteristics (operability, ability to be trimmed, and durability) were similar between the control and treatment groups. This was evaluated through a questionnaire with a visual analog scale. However, an analysis of this extensively collected data could not be included in this study. The treatment group also reported a slightly better ease of use of the membrane than the control group. However, 1 participant in the treatment group dropped out of the study during follow-up as a result of the membrane not being secured into the extraction socket.
Most existing studies have evaluated dimensional ridge alteration following a ridge preservation procedure with measurements of the buccolingual width and/or height [202122]. We evaluated this in 3 dimensions by superimposing data obtained through CBCT and a 3D scanner, which allowed changes in the edentulous ridge to be evaluated in greater detail.
It can be concluded that a ridge preservation procedure using a bone graft and resorbable membrane is effective in decreasing dimensional changes of the edentulous ridge. However, no differences between the different resorbable membranes were found in this study.
 XML Download
XML Download