

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peri-implantitis is an inflammatory process that affects tissues around osseointegrated implants, resulting in the loss of supporting bone [1]. It is caused by the same bacteriological factors as those involved in the onset of inflammatory periodontal disease [2]. Hultin et al. [3] reported that the proportions of periodontal pathogens, such as Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythia, and Treponema denticola, were highly elevated in peri-implantitis. Therefore, it has been proposed that the treatment of peri-implantitis should ultimately involve anti-bacterial treatment.
However, mechanical debridement alone cannot effectively eradicate these key pathogens due to the surface characteristics and topography of implant fixtures. Although the bleeding tendency showed a slight decrease in response to mechanical debridement, alone with carbon fiber curettes or with the Vector® system, a novel ultrasonic device, the probing pocket depth (PPD) was unchanged or aggravated [4]. Another study that compared titanium curettes and ultrasonic devices as tools for nonsurgical mechanical debridement reported a similar result [5]. Thus, it may be necessary to devise adjunctive therapies such as the local delivery or systemic administration of antibiotics and/or laser therapy.
Beneficial effects of the local delivery of antibiotics for the treatment of periodontitis or peri-implantitis have been reported [678910]. Minocycline ointment applied into the periodontal pocket improved clinical parameters associated with periodontitis and reduced the bacterial count in the periodontal pocket [6]. Mombelli et al. [7] reported that they were able to suppress pathogens such as T. forsythia, P. gingivalis, P. intermedia, and A. actinomycetemcomitans for up to 12 months after the topical application of tetracycline fibers in the management of peri-implantitis. In addition, several studies have reported similar clinical and microbiological improvements with the use of local delivery devices for the treatment of peri-implantitis [89]. However, studies evaluating clinical and radiographic outcomes after the combined use of topical antimicrobial agents are currently lacking.
Despite the high success rates of modern implant procedures, the rate of peri-implantitis–related morbidity is increasing, posing a challenge for most dental practitioners. Furthermore, the predictability of complete osseous regeneration around peri-implant intrabony defects appears to be quite low, while bone regeneration techniques may require an unrealistically high level of surgical expertise for general dentists.
The aim of the present study was to develop a simple and practical nonsurgical treatment modality suitable for most forms of intrabony defects around dental implants using combined intrasulcular delivery of chlorhexidine solution and minocycline hydrochloride (HCl).
Go to : 
MATERIALS AND METHODS
Study design
Patient inclusion criteria
The study recruited 20 patients (12 men and 8 women; mean age, 65.7 years) suffering from peri-implantitis in 45 osseointegrated implants diagnosed at the Department of Periodontology, Pusan National University Dental Hospital, from November 2015 to April 2017.
The inclusion criteria were good general health and a diagnosis of peri-implantitis. We diagnosed peri-implantitis based on the following 2 criteria: (a) peri-implant PPD ≥5 mm with concomitant bleeding on probing (BOP) at least 1 peri-implant site, and (b) radiographic evidence of ≥2 mm of bone loss.
The exclusion criteria were as follows: (a) peri-implant mucositis (absence of radiographic marginal bone loss), (b) uncontrolled periodontal conditions, (c) an allergy to tetracycline, or (d) pregnancy or lactation.
The study protocol was approved by the Institutional Review Board (IRB #PNUDH-2016-021-MS) of Pusan National University Dental Hospital. All patients received a detailed description of the proposed study protocol and provided written informed consent to participate in the study.
Nonsurgical treatment modality
The day when treatment started after the initial diagnosis of peri-implantitis was considered the baseline day. On the baseline day, clinical and radiographic examinations were performed after oral hygiene instruction followed by intrasulcular antiseptic irrigation using 0.1% chlorhexidine gluconate solution (Hexident® solution, Dongin-Dang Pharmaceuticals, Siheung, Korea) and topical application of minocycline HCl gel (Minocline®, DongKook Pharma, Seoul, Korea) into the peri-implant pockets. At the endpoint examination, which occurred 6 or 12 months after the baseline day, clinical and radiographic examinations were performed. Between the baseline day and the endpoint, patients were scheduled to visit the periodontal clinic every 2–4 weeks depending on the surface characteristics around the implant fixtures, and chlorhexidine irrigation and local delivery of minocycline HCl gel were performed at every visit. The visit schedule was adjusted from a 2-week to a 4-week interval when neither BOP nor exudate was observed upon gentle pressure.
Clinical assessments
At the baseline day and the endpoint, the following clinical parameters were measured at 6 locations for each implant (distobuccal, buccal, mesiobuccal, distolingual, lingual, and mesiolingual) using a periodontal probe (Periodontal probe PFG-W, OSUNG Co., Gimpo, Korea); 1) PPD, 2) clinical attachment level (CAL), and 3) BOP. In addition, the patient's history of guided bone regeneration (GBR), presence of premature contact, and the width of keratinized gingiva were also recorded at the baseline examination to assess additional contributing factors to peri-implantitis.
Radiographic assessments
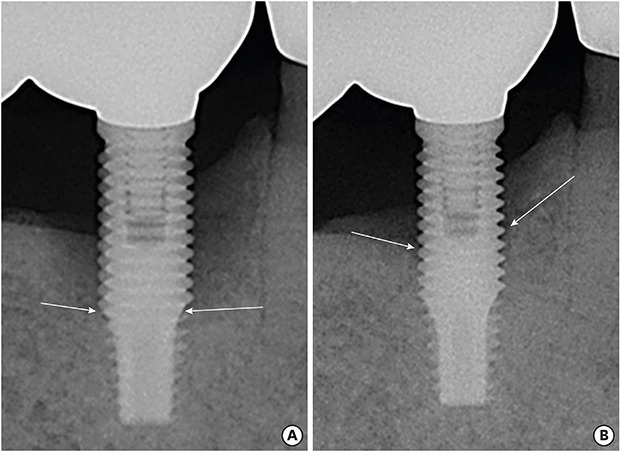
Standardized periapical intraoral radiographs using a long-cone paralleling device were obtained at the baseline day and the endpoint (Figure 1), as well as 6 months following nonsurgical treatment to assess the interproximal bone levels. Patients who showed continued bone absorption and persistent inflammation at 6 months were excluded from the study and a nonsurgical or surgical intervention based on cumulative interceptive supportive therapy (CIST) was attempted [11]. Three patients who demonstrated radiographic evidence of continued bone absorption or no bone gain dropped out of the study for further surgical intervention as necessary.
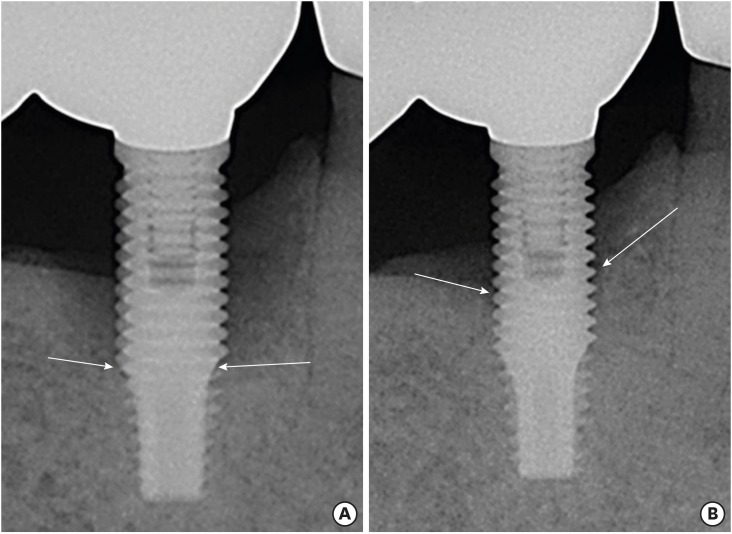
For a comparative analysis of bone changes according to the defect morphology, we subdivided the morphology of the peri-implant intraosseous defects by adapting the classification system of intrabony defect morphology for natural teeth, as follows [12]. Based on the baseline radiographic examination, the radiographic osseous defect morphology at the mesial or distal aspect of each implant was classified as 1) narrow (≤25°) or wide (≥37°), and 2) shallow (≤3 mm) or deep (≥4 mm). To assess linear height changes (in millimeters) at the interproximal alveolar bone crest between the baseline day and the endpoint, the distance from the implant shoulder to the most coronal bone-to-implant contact point (DIB) was determined at both the mesial and distal aspects of each implant (Figure 2). An image analysis software program (AxioVision; Carl Zeiss Co., Oberkochen, Germany) was used to analyze the radiographic intraosseous changes, after the numerical measurement values were standardized by compensating for the implant fixture length.
 | Figure 2The distance from the implant shoulder to the most coronal bone-to-implant contact point (DIB) was measured at the mesial and distal aspects of each implant: A, implant shoulder; B and B′, the most coronal bone-to-implant contact point; C, apex of the implant fixture; A–B, DIB at the distal aspect; A–B′, DIB at the mesial aspect; and A–C, length of the implant fixture (on radiographic view). Amount of actual marginal bone loss at the mesial and distal aspects (X′ and X) calculated follow as:X′=(A–B′)×fixture length (actual)/(A–C)
X=(A–B)×fixture length (actual)/(A–C)
|
Statistical analysis
Clinical parameters (PPD, CAL, and BOP) and DIB values at the baseline day and the endpoint were expressed as the mean values±standard deviation (SD). Levels of significance between the baseline day and the endpoint assessments were analyzed using the paired t-test for intragroup comparisons and the Student t-test for intergroup comparisons. All statistical analyses were performed using SPSS (version 18 for Windows; SPSS Inc., Chicago, IL, USA), and P values <0.05 were considered to indicate statistical significance. We chose the measurement number as 45 implants based on an expected attainable radiographic bone gain of 1.5 mm with an SD of 2 mm, and a level of significance of 0.05 using the 2-tailed test with power >99%.
Go to :
RESULTS
Clinical outcomes
The mean values (±SD) of the parameters of PPD (in mm), CAL (in mm), and BOP (percentage of positive sites) at the baseline day and the endpoint are summarized in Table 1. The PPD, CAL, and BOP decreased significantly at the endpoint compared with the baseline values (P<0.05). GBR was present at 26.7% of the peri-implantitis sites, and premature contact on the balancing side was present at 28.9%. The mean width of keratinized gingiva was 0.48 mm, and 36 (80%) of the 45 implants were surrounded by peri-implant mucosa alone.

Table 1
Mean values±SD of PPD (in mm), CAL (in mm), and BOP (percentage of positive sites) at the baseline day and the endpoint
PPD: probing pocket depth, CAL: clinical attachment level, BOP: bleeding on probing.
a)Statistically significant difference compared to the baseline day.
![]()
Radiographic outcomes
On the standardized radiographs, the DIB was measured on the mesial and distal aspects of the 45 implants. Of the 90 total sites, 79 were evaluated, and 11 were excluded due to the absence of an intrabony defect. Of the 79 sites, 33 sites were classified as narrow and 46 sites as wide. Forty-one sites were shallow, and 38 were deep. The mean DIB values on the baseline day and the endpoint are shown in Table 2. Regardless of defect morphology, the mean DIB values at the endpoint were significantly lower than on the baseline day (P<0.05). The greatest change in bone level was observed in the deep defects (∆DIB=1.81±0.94 mm). Table 2 compares the mean DIB changes among the groups. The mean DIB change in the deep defects (1.81±0.94 mm; range, 0.61–3.97 mm) was significantly greater than that in the shallow defects (0.93±0.47 mm; range, 0.31–2.44 mm). The mean DIB change in the narrow defects was 1.54±0.87 mm (range, 0.52–3.97 mm), and that in the wide defects was 1.22±0.83 mm (range, 0.31–3.49 mm). The mean bone gain was greater in the narrow defects; however, the difference was not statistically significant (P>0.05).

Table 2
Comparison between the DIB changes (∆DIB) of each defect type (mean±SD in mm)
DIB: distance from the implant shoulder to the most coronal bone-to-implant contact point, SD: standard deviation.
a)Statistically significant difference compared to the baseline day (P<0.001); b)Comparison between the ∆DIB of the narrow type and the wide type; the difference was not statistically significant; c)Comparison between the ∆DIB of the shallow type and the deep type; the difference was statistically significant.
![]()
Go to :
DISCUSSION
This study was devised to develop a simplified nonsurgical modality for the management of ongoing peri-implantitis by comparing the clinical and radiographic findings over the course of 6–12 months after repeated intrasulcular chlorhexidine irrigation and topical application of minocycline HCl, depending on the depth and morphology of the intrabony defects. Because complete restoration of the lost surrounding peri-implant bone structure is considered to be infeasible to achieve, the ultimate goal was to achieve a stable and sustainable bone level, with improvement to the horizontal defect type, through regular simple nonsurgical management that hampered progressive peri-implant disease.
Substantial improvements were observed in clinical and radiographic parameters in response to the nonsurgical treatment of peri-implantitis using chlorhexidine and minocycline HCl, which is consistent with previous studies that have reported clinical, radiographic, and microbiological improvements through the use of local delivery devices for the treatment of peri-implantitis [8910]. We investigated the associations of several predisposing factors with peri-implantitis. Even though the prevalence of a history of GBR (26.7%) and premature contact (28.9%) was relatively low, this factor should not be underestimated. Surprisingly, 80% of implants suffering from ongoing disease had no keratinized gingiva. Although there is skepticism regarding the necessity of keratinized gingiva around implants [131415], the present study revealed that peri-implantitis was closely associated with a deficiency in the zone of keratinized gingiva.
At the endpoint, the bone levels had increased in all intrabony defects, regardless of their morphology, although the deep defects showed the greatest bone gain. When the effect of defect dimensions on regeneration was evaluated after performing guided tissue regeneration on intrabony defects [16], deep and narrow intrabony defects were found to have greater potential for periodontal regeneration than wide and shallow defects. A multicenter, randomized, controlled clinical trial of the treatment of deep and shallow intrabony defects also demonstrated greater attachment gains in deep defects than in shallow defects [17]. Taken together, these findings further corroborate our results.
CIST has been recommended as an alternative treatment of peri-implantitis [11]. In this study, we proposed a simple nonsurgical treatment modality that is easily accessible and readily available for most dental practitioners. Mechanical debridement or decontamination procedures were excluded in the present study design because in most cases in this study, the implant was surrounded by thin and narrow friable mucosa only, without keratinized gingiva. This anatomical structure did not permit the introduction of mechanical devices into the friable sulcus. It was almost impossible to insert a physical instrument or perform surface cleansing using a motorized machine, because doing so would increase the risk of damage to the fixture threads. Therefore, irrigation of chlorhexidine solution using syringe needles with very narrow diameters for easy manipulation, combined with the topical application of minocycline gel, was considered to be the most realistic approach for biofilm decontamination. Indeed, nonsurgical mechanical debridement alone has been shown to be effective in the treatment of peri-implant mucositis [1819]. However, the results of this method in the treatment of peri-implantitis are currently limited [202122]. Persson et al. [22] claimed that mechanical debridement of the peri-implantitis site with a titanium curette or ultrasound device resulted in a temporary change in only some bacterial species, which returned to baseline levels after 6 months of treatment. Therefore, for the improvement of peri-implantitis, it seems that repetitive treatment is more important than the treatment modality itself.
A systematic review evaluating the efficacy of treatment for peri-implantitis, regardless of the treatment modality, reported recurrence of peri-implantitis in up to 100% of cases [23]. In another study, 42% of treated implants showed persistent peri-implantitis despite surgical intervention [24]. In this respect, supportive peri-implant therapy seems to be reasonable, as it is evident that any single treatment modality for peri-implantitis would not successfully yield long-term outcomes without treatment strategies to prevent reinfection. Even though the improvement in clinical and radiographic parameters obtained by the present approach showed sustainability throughout the observation period in this study, long-term maintenance of peri-implantitis may be have to be reinstituted using the same regimen. Conclusively, through a simplified nonsurgical treatment modality for the management of peri-implantitis using chlorhexidine and minocycline HCl, we report the successful management of intraosseous defects of all types. Our proposed approach was associated with significant and sustainable improvements in both clinical and radiographic parameters, and is readily available for general practitioners.
Go to :
 XML Download
XML Download