

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Because chronic periodontitis is an infectious disease that is caused by bacteria, the treatment of periodontitis requires removal of the bacterial biofilm during the initial stages of treatment, as well as during periodontal maintenance care [12]. Traditionally, removal of the biofilm is performed via mechanical methods, using hand tools and ultrasonic instruments [3]. A typical mechanical method is scaling and root planing (SRP), which is considered to be the “gold standard” of periodontal treatment [4].
However, SRP using hand tools and ultrasonic instruments is time-consuming; moreover, it may cause irreversible dental hard tissue damage and should be performed with caution [56]. Even if SRP is performed by a well-trained practitioner, patients may experience discomfort during treatment and an increased tendency to experience pain, adversely affecting compliance after treatment [78]. Notably, SRP requires the dentist to accurately visualize residual calculus; as a result of anatomical factors and difficulties accessing the target teeth, the residual calculus ratio has been reported to be higher on the lingual side than on the buccal side after SRP [9]. Especially in the furcation area, residual subgingival calculus or incomplete root planing may occur [1011]. Moreover, Greenstein [12] concluded that the results of SRP vary according to the skill of the operator.
Therefore, if additional treatments can supplement an incomplete SRP treatment, such treatments may reduce variability in the outcomes of non-surgical periodontal treatment related to the operator, tooth morphology, and positional differences, thereby reducing the need for surgical treatment.
Air-polishing devices have been introduced to clean the root surface by spraying the tooth surface with compressed air containing abrasive particles and water. This method has been reported to be an efficient and convenient way to mechanically remove bacterial deposits such as biofilm and calculus [1314]. Abrasive sodium bicarbonate has generally been used in air-polishing devices to remove supragingival biofilms. However, since sodium bicarbonate can cause erosion of enamel, it must be used carefully on surfaces with demineralized enamel [15]; moreover, it occasionally causes corrosion on restorative materials such as amalgam, gold, or composite [16]. Thus, low-abrasive air-polishing powders, such as glycine, have been developed for the removal of subgingival biofilm. The abrasiveness of glycine is approximately 80% lower than the previously used bicarbonate air-polishing powder [17]. Glycine air-polishing devices cause less damage to the hard tissue than SRP and reduce bacterial colony formation in 3- to 5-mm deep periodontal pockets [18]. In addition, Flemmig et al. [19] reported that the use of an air-polishing device in cases of moderate-to-deep periodontitis was more effective than SRP in removing subgingival biofilm. However, Wennström et al. [20] reported no clinically or microbiologically significant differences between SRP and glycine air-polishing devices during maintenance therapy.
In recent years, erythritol powder has been introduced for use in a new air-polishing device [21]. Erythritol is a non-toxic, chemically neutral, water-soluble material that is used worldwide as a food additive and artificial sweetener [22]. Erythritol is suitable for the removal of gingival biofilm because of its relatively small particle size and stable chemical properties, relative to glycine [21]. Erythritol is also effective against some periodontal bacteria, including Porphyromonas gingivalis [23]. The use of an erythritol powder air-polishing device (EPAP) was found to be similar to SRP in terms of effectiveness in the removal of supragingival and subgingival biofilms when supportive periodontal therapy was performed. Importantly, the use of erythritol was more efficient in terms of comfort and time efficiency [24]. However, this determination was made following use in maintenance patients after the initial periodontal treatment. In contrast, no studies have analyzed the effects of EPAP use during active periodontal therapy.
In this study, we compared the clinical and microbiological effects of treatment with EPAP, as a supplement to conventional treatment using a hand curette and ultrasonic scaler for non-surgical periodontal treatment, in patients with moderate chronic periodontitis.
MATERIALS AND METHODS
Study design
Patients were enrolled in the study if they visited the Pusan National University Dental Hospital between March 2017 and August 2017 and expressed interest in participating voluntarily. The inclusion criteria for this study were as follows: 1) patients who ranged in age from 19 to 70 years old; 2) patients with moderate chronic periodontitis, who required removal of calculus and root planing treatment; 3) patients exhibiting at least 1 tooth with a probing pocket depth of 4–6 mm in any of the teeth from the incisor to the second molar on either side of the oral cavity. The exclusion criteria for this study were as follows: 1) patients with systemic disease; 2) patients who were pregnant or breastfeeding; 3) patients who received periodontal treatment or antibiotic treatment within 6 months prior to participating in the study.
A total of 21 patients were evaluated in this study. The inclusion of 21 patients (considering a risk of 10% drop-out) would allow the detection of a mean difference of 0.5 mm in pocket depth (PD) change between treatments with a study power of 0.80, an error of 0.05 and with a standard deviation of 0.7 mm. Two quadrants were chosen from each patient and assigned to the control and experimental groups, such that 21 control sites and 21 experimental sites were evaluated (1 control and 1 test site per patient). The experimental protocol was approved by the Ethics Committee of Pusan National University Dental Hospital (PNUDH-2017-006). This study was conducted by a well-trained periodontist in accordance with the Helsinki declaration, following the 2010 CONSORT guidelines (Korea Clinical Research Information Service registration number: KCT0002788).
Clinical procedures
In this study, the following clinical parameters were measured: 1) periodontal (PD; the distance from the margin of the free gingiva to the pocket base); 2) gingival recession (REC; the distance from the cementoenamel junction to the margin of the free gingiva); 3) clinical attachment level (CAL; the distance from the cementoenamel junction to the pocket base); 4) plaque index (PI; an index of oral hygiene, wherein no plaque attached to the tooth is scored as 0; plaque that is attached to the margin of the tooth and the free gingiva is scored as 1 and can only be confirmed by scratching the tooth surface with a periodontal probe; a large amount of plaque in the periodontal pocket and gingival margin that can be seen by the naked eye, but does not include plaque deposits in the proximal areas is scored as 2; and a large amount of plaque deposits including within the proximal area is scored as 3); and 5) bleeding on probing (BOP; if bleeding is observed within 30 seconds after periodontal probing, the percentage of the bleeding area is measured in relation to the whole area).
PI was measured at 4 sites per tooth (mesiobuccal, mid-buccal, distobuccal, and palatal/lingual); each of the other clinical parameters was measured at 6 sites per tooth (mesiobuccal, mid-buccal, distobuccal, mesiolingual, mid-lingual, and distolingual). All measurements were rounded to the nearest 1 mm, and were obtained using a periodontal probe (PGF-W, Osung, Gwangmyeong, Korea).
Clinical indices were measured by a well-trained periodontist at 3-time points: before treatment, 1 month after treatment, and 3 months after treatment.
Treatment procedures
Supragingival calculus was removed from all dentition and patients received oral hygiene education. Before the non-surgical treatment of a subgingival pocket, a randomized envelope specifying whether it was assigned to the test or control group was opened to determine which treatment would be performed.
In both the test and control groups, under local anesthesia, all periodontal pockets and root surfaces were treated with SRP, using Gracey curettes (Hu-Friedy, Chicago, IL, USA) until the operator felt smoothness and flattening of the root surface. In the test group, an EPAP with Perio-Flow System (EMS, Geneva, Switzerland) was applied to the tooth for 5 seconds per pocket. A nozzle tip designed specifically for the gingival sulcus was inserted into the periodontal pocket as directed by the manufacturer; then, slurry including erythritol powder was sprayed onto the root surface. All treatment procedures were performed by a single well-trained periodontist who was familiar with the use of the air-polishing device.
Collecting subgingival samples
Subgingival plaque samples were collected preoperatively, as well as 1 month and 3 months after treatment; teeth with the deepest probing depth were selected in each test and control group. The subgingival plaque sample was obtained by using gauze to isolate the selected tooth from saliva and blood, and then inserting a sterilized curette under the periodontal pocket. The samples were transferred to a 1.5-mL tube containing 500 μL of sterile 0.225% Ringer's solution, then stored at −20°C until analysis.
Microbiological analysis
The subgingival plaque samples were analyzed to quantify the amount of Aggregatibacter actinomycetemcomitans, Campylobacter rectus, Eikenella corrodens, Fusobacterium nucleatum spp., P. gingivalis, Prevotella intermedia, Treponema denticola, and Tannerella forsythia; the total bacterial count (TBC) was determined using the quantitative real-time polymerase chain reaction method (qRT-PCR). The PCR primers and product size are shown in Table 1. For analysis, each sample stored at −20°C was transferred to a 1.5-mL centrifuge tube containing 200 μL of phosphate-buffered saline (PBS), and the RNA was then extracted as follows, using the TRIzol reagent. After removing the PBS buffer, 200 μL of TRIzol and 40 μL of chloroform were added to the tubes to ensure that samples were completely homogenized. Then, the tube was put at 23°C–25°C for 15 minutes, followed by centrifugation at 4°C for 15 minutes. The supernatant was transferred to a new 1.5-mL tube, and 500 μL of isopropanol was added, followed by centrifugation at 4°C for 15 minutes. After the isopropanol was carefully removed from the pellet, the above procedure was repeated, and the pellet was dried at 23°C–25°C for 15 minutes. The dried RNA pellet was dissolved in 20 μL of RNase-free water, then heated at 60°C for 10 minutes to resuspend the RNA. cDNA was synthesized using Dyne reverse transcriptase (DyneBIO, Seoul, Korea), followed by quantitative determination of the extracted RNA concentration using a microplate reader (Synergy HTX Multi-Mode Reader, Biotek, Winooski, VT, USA).
Table 1
PCR primers and product size
![]()
qRT-PCR was performed using the ABI 7500 Fast thermocycler (Applied Biosystems, Foster City, CA, USA). A total of 1 μL of template DNA and 1 μL of primer were added to 10 μL of Dyne qRT-PCR 2X premix (SYBR Green with low ROX, DyneBIO), and the total volume was adjusted to 20 μL using diethyl pyrocarbonate. The first denaturation was performed at 95°C for 10 minutes, followed by amplification at 95°C for 15 seconds, at 58°C for 1 minute, and at 72°C for 1 minute for 55 cycles. During qRT-PCR, SYBR Green fluorescence was detected by binding of SYBR Green to the double-stranded DNA synthesized by PCR; this generated a fluorescent signal as the reaction proceeded, such that the amount of amplification product was measured by analyzing the fluorescent signal pattern associated with the target gene.
Statistical analysis
Clinical parameters and relative bacterial gene expression, before and after periodontal treatment, were compared between the test and control groups and expressed as mean and standard deviation. The relative bacterial gene expression level, measured by qRT-PCR analysis, was calculated using the comparative Δ-CT method, as described by Pfaffl [25]. The Kolmogorov-Smirnov test was used to test whether the measured values exhibited a normal distribution for all 21 samples in each group. Clinical parameters before treatment, as well as at 1 and 3 months after treatment, in each group were analyzed by repeated-measures analysis of variance. Comparisons of measurements between the test and control groups were analyzed using the paired t-test. The significance level was set at 0.05 for all analyses, and all statistical analyses were performed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
There were 152 treated teeth in the test group and 151 in the control group. In the test group, the number of teeth with a probing depth of >4 mm was 93, whereas it was 91 in the control group. Furthermore, the distributions of treated teeth were also similar between the test and control groups in each patient (Table 2).
Table 2
Distribution of tooth groups and pocket probing depths in the test and control groups in each patient
Values are presented as mean±standard deviation in each quadrant.
SRP: scaling and root planning, EPAP: erythritol powder air-polishing device, PD: probing depth.
![]()
Clinical results
In both the test and control groups, there was a significant decrease in PD, PI, and BOP, accompanied by an increase in REC and significant gain in CAL, when the conditions before treatment were compared with those after treatment. There was no significant difference in clinical parameter changes between the test and control groups. Clinical parameters showed improvements at 1 month compared to baseline; in contrast, the results at 3 months after treatment were worse than those at 1 month after treatment (Table 3).
Table 3
Clinical parameters at baseline, 1 month after treatment, and 3 months after treatment (n=21)

Values are presented as mean±standard deviation.
PI: plaque index, BOP: bleeding on probing, PD: probing depth, CAL: clinical attachment level, REC: gingival recession, SRP: scaling and root planning, EPAP: erythritol powder air-polishing device, 1MC: 1-month check, 3MC: 3-month check.
a)Statistically significant difference in clinical indices were found among the baseline, 1-month check, and 3-month checks, using repeated-measures analysis of variance (P<0.05); b)No significant differences in clinical parameters were found between the SRP and SRP+EPAP groups, using the paired t-test, from baseline to the 3-month check (P=0.05).
![]()
Microbiological results
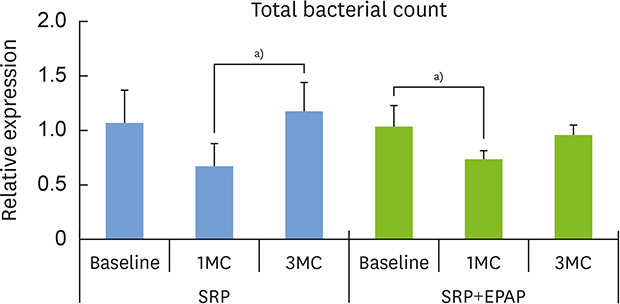
The TBC significantly (P<0.05) changed from baseline to 1 month after treatment and 3 months after treatment, in both the test and control groups. In the test group, the number of bacteria decreased significantly (P<0.05) between baseline and 1 month after treatment. In the control group, the number of bacteria increased significantly between 1 month and 3 months after treatment (P<0.05, Fig. 1).
 | Figure 1Total bacterial count at baseline, 1 month after treatment, and 3 months after treatment, compared between the test and control groups.SRP: scaling and root planning, EPAP: erythritol powder air-polishing device, 1MC: 1-month check, 3MC: 3-month check.
a)Statistically significant (P<0.05). Error bars indicate standard deviation.
|
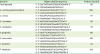
The relative expression levels of A. actinomycetemcomitans, C. rectus, E. corrodens, F. nucleatum, P. intermedia, T. denticola, and T. forsythia were not significantly different following treatment in either the test or control group. However, the relative expression level of P. gingivalis was significantly lowered between baseline and 1 month after treatment (P<0.05, Fig. 2).
 | Figure 2Relative levels of A. actinomycetemcomitans, C. rectus, E. corrodens, F. nucleatum spp., P. gingivalis, P. intermedia, T. denticola, and T. forsythia between test and control groups at baseline, 1 month after treatment, and 3 months after treatmentSRP: scaling and root planning, EPAP: erythritol powder air-polishing device, 1MC: 1-month check, 3MC: 3-month check.
a)Statistically significant (P<0.05). Error bars indicate standard deviation.
|
DISCUSSION
This study compared the clinical and microbiological results of conventional SRP alone with those of SRP combined with EPAP treatment. No significant difference was found in clinical improvements between the 2 treatment protocols before and after treatment. However, in both treatments, there was a significant decrease in PD, PI, and BOP, as well as increased REC and gains in CAL, from baseline to 1 month after treatment and 3 months after treatment. Our results are similar to the data reported by Hägi et al. [21], who compared SRP with EPAP during maintenance care following periodontal treatment. We found no side effects in either treatment; moreover, SRP combined with EPAP yielded similar short-term clinical effects to those obtained using SRP alone.
Microbiological analysis indicated that the TBC significantly changed from before treatment to 1 month after treatment and 3 months after treatment in both the test and control groups. Thus, SRP alone and SRP combined with EPAP were both effective for removing the subgingival biofilm in patients with moderate chronic periodontitis. Petersilka et al. [18] and Flemmig et al. [19] reported that the use of a glycine powder air-polishing device in patients with moderate periodontitis resulted in a significant reduction in the TBC compared with SRP treatment during maintenance care. Hägi et al. [24] conducted microbiological comparisons of SRP and EPAP treatment during maintenance care for up to 6 months. However, in both groups, only slight changes in microbiological composition were observed after treatment; there were no significant changes in A. actinomycetemcomitans, E. corrodens, P. gingivalis, T. forsythia or T. denticola. In our study, the TBC decreased significantly between baseline and 1 month after treatment in SRP with EPAP group.
However, the TBC increased significantly between 1 month and 3 months after treatment in the SRP-only group. This is consistent with the findings of Flemmig et al. [19], who demonstrated an increase in the TBC at 3 months after treatment with glycine in moderate and deep periodontal pockets. Therefore, maintenance therapy is important to prevent and control periodontal disease.
In our study, the level of P. gingivalis in the group that underwent SRP+EPAP was significantly lower than that of the control group at 1 month after treatment. This is consistent with the report by Hashino et al. [23] that erythritol had an antimicrobial effect, via alteration of the microstructure and metabolic profile of P. gingivalis biofilm in vitro. It is noteworthy that we clinically confirmed an antimicrobial effect against P. gingivalis, as this species is a member of the “red complex” of periodontal bacteria and is thus a keystone pathogen in the development of chronic periodontitis through dysbiosis of the periodontal microbiota [2627]. Evans et al. [28] and Persson et al. [29] reported that the in vivo reduction of P. gingivalis prevented alveolar bone loss; in most cases, the destruction of periodontal tissue was also reduced. Therefore, the decrease in P. gingivalis is important for decreasing the incidence of periodontal disease.
The use of an air-polishing device in the subgingival area carries a risk of emphysema, which usually resolves without treatment in healthy patients within 24–72 hours. In this study, no side-effects (e.g., emphysema) were found. A very low incidence of empyema has been reported after treatment with minimally abrasive powders, such as glycine and erythritol [30]. This indicates that subgingival areas are gently cleaned by particles with low abrasiveness, and there are no subsequent large collapses of periodontal tissue. Further, using nozzles specially designed for insertion into the subgingival pockets, the air jet is applied vertically to the root surface, thereby reducing the working pressure and likelihood of resultant emphysema.
In conclusion, this study suggests that both SRP and SRP combined with EPAP were clinically and microbiologically effective as non-surgical periodontal treatments. In particular, the SRP with EPAP group showed an antimicrobial effect on P. gingivalis, a keystone bacterium associated with the onset of chronic periodontitis, in a short-term period.
 XML Download
XML Download