

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dental implants are modern dentistry's best option for replacing missing teeth. As the demands for implant treatment continue to increase, there are many situations in which inadequate bone volume (BV) is present for the placement of dental implants. Guided bone regeneration (GBR) is the most widely used technique to regenerate and augment bone. A series of clinical studies [123] and animal experiments [456] have documented the effectiveness of GBR in augmenting bone. This procedure was derived from the biological principle of guided tissue regeneration (GTR) developed by Nyman et al. [78] in the early 1980s for regenerating periodontal tissue lost as a result of periodontal disease. According to the principle of GTR, the cells that first populate a wound area determine the type of tissue that ultimately occupies the space. Based on this principle, a technique utilizing barriers to prevent non-desirable epithelial cells from migrating into a wound was developed in the field of bone regeneration.
The sequence and the pattern of bone regeneration in GBR procedures have been investigated in few experimental studies. Yamada et al. [910] histologically studied rabbits with titanium caps on the calvarium. Histological observations confirmed the presence of trabecular bone, consisting of mineralized bone and an osteoid, bone marrow, and blood clots, in the occlusive space. Thus, they concluded that the newly generated tissue in the occlusive space was bone tissue augmented from the existing parietal bone. Schenk et al. [11] investigated surgically created, membrane-protected defects in the ridge in dogs. Their histological analysis showed that healing started with the formation of a blood clot, a connective tissue matrix replaced this blood clot, and then, the deposition of the woven bone was replaced by lamellar bone.
Even though augmented bone (AB) has been examined histologically in many studies, few studies have examined the biological potential and healing dynamics following the use of AB. Whether bone obtained from the GBR procedure possesses the same functions as the existing autogenous bone is uncertain. In particular, little attention has been paid to the regenerative ability of GBR bone.
Furthermore, it is difficult to obtain an adequate quantity of AB for implant placement. To overcome these limits, procedures using a bone substitute [1213] or bioactive molecules [1415] are used with the original GBR theory. Even if adequate BV is acquired successfully by the GBR procedure, a bony ridge in the desired shape is rarely obtained. In these cases, additional definitive osteoplasty is needed, and bony particles of the GBR bone are generated as byproducts. If the regenerative ability of the guided bone augmentation (GBA) bone is confirmed, the application of this bone can be widened and the bone can be reused.
Therefore, the present study histologically evaluated the regenerative capacity of AB in the occlusive space of a rat GBA model.
MATERIALS AND METHODS
Animals
Thirty 8-week-old male Fischer rats weighing 250–300 g were used. The animals were housed in an experimental animal room (22°C, 55% humidity, 12/12-hour light/dark cycle) and fed a standard laboratory diet and water. The Animal Experimentation Committee of the Nihon University School of Dentistry approved the present study (AP14D026).
Primary surgery
In the AB group, a rat GBA model reported and standardized previously by our group was applied by setting plastic caps on the rat calvaria [1213]. All operations were conducted under sterile conditions. The animals were premedicated by the inhalation of an isoflurane anesthetic and were subjected to general anesthesia by an intraperitoneal injection of a mixture of 0.15 mg/kg dexmedetomidine hydrochloride, 2.0 mg/kg midazolam, and 2.5 mg/kg butorphanol tartrate. An intraperitoneal injection of 0.5 mL of a 1:80,000 dilution of lidocaine (Xylocaine, Astra Zeneca, Osaka, Japan) was administered to control bleeding and provide additional anesthesia. Thirty rats were randomly divided into 3 groups. In 10 of the 30 rats (the AB group), a skin incision approximately 6.0 cm long was made over the linea media to raise the skin of the calvarium. A cutaneous flap was raised laterally by using a small sharp periosteal elevator, and then, the periosteum was incised and lifted to expose the calvarium. A circular groove was made on the right of the midsuture by using a trephine burr with an inner diameter of 5 mm under profuse irrigation with sterile saline. Five small holes were drilled with a No. 2 round burr to induce bleeding from the bone marrow space within each circle. The circular groove and the 5 holes were created carefully so as to not penetrate the dura. A cylindrical plastic cap was pressed into the circular groove and fixed in place with light-cured 4-methacryloxyethyl trimellitate anhydride (META) resin. In the other 20 rats (10 rats in the cortical bone group [CB group] and 10 rats in the control group), only the skin incision and the cutaneous flap elevation were done in the same way as in the AB group. Animals in both the CB and the control group were not treated with the GBA procedure. In all the animals, the skin was then carefully sutured with resorbable 4/0 polyglactin sutures.
Secondary surgery
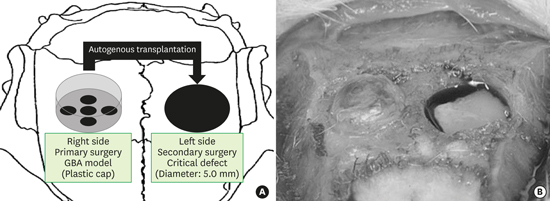
All animals were fed under normal conditions. Secondary surgery was done 12 weeks after the primary operation. In the secondary operation, anesthesia, incision, and flap elevation were done in the same way as in the primary operation. Then, in all the animals, a critical-sized calvarial bone defect (5.0 mm) was trephined into the dorsal bone on the right. Defects were created using a dental surgical drilling unit equipped with a trephine, which was cooled constantly with sterile saline. Then, the calvarial disk was carefully removed to avoid tearing the dura. In the AB group, plastic caps placed in the primary operation were carefully removed, and regenerated tissues generated inside of the caps were examined. Then, the regenerated bony tissue was harvested using a bone scraper (Safescraper, Osteogenics, Lubbock, TX, USA). In the CB group, the autogenous CB was harvested from the left lateral bone in the rat calvarium using a bone scraper. After thoroughly rinsing the calvarial defects with physiological saline to wash out any bone fragments, bone particles harvested using bone scrapers were filled into the defects. In all the animals, the skin was then carefully sutured in the same way as in the primary procedure. The procedure practiced in the AB group is schematically presented in Figure 1A, and a photograph of the secondary operation taken just after the removal of the plastic caps is presented in Figure 1B.

Micro-computed tomography (micro-CT) imaging analysis
Repeated micro-CT imaging was carried out using a micro-CT system (R_mCT2, Rigaku Co., Tokyo, Japan) at 0, 4, 8, and 12 weeks after the secondary surgery. Rats were anesthetized with an inhalation of isoflurane and placed on the stage. Images of the regions of interest (ROIs) were captured without euthanasia. ROIs were defined on the bone defects, each of which had a diameter of 5.0 mm and a height of 3.0 mm. The bone tissue in the ROI was analyzed under the same conditions at each time point. The amount of BV within each ROI was examined using BV measurement software (Kitasenjyu Radist Dental Clinic, I-View Image Center, Tokyo, Japan).
Histological analysis
Twelve weeks after the secondary surgery, the animals were sacrificed with excess CO2 gas inhalation. The skin was dissected, and the defect sites were removed, along with the surrounding bone and soft tissues. The calvaria were harvested, fixed in 10% formalin, decalcified with a formic acid-sodium citrate decalcification solution for 1 week, and embedded in paraffin wax. Then, coronal sections (thickness: 5 μm) through the center of the circular defects were prepared and processed for hematoxylin and eosin (H&E) staining. A histological examination was performed under a light microscope equipped with a morphometric system, which was connected to a personal computer. From the histological sections, defect closure rates (%) were calculated. The defect closure rate was determined by measuring the distance between the defect margins and was expressed as a percentage of the width of the total defect.
Sections were deparaffinized, and the endogenous peroxidase activity was quenched by incubation in 3% H2O2 in methanol at room temperature for 15 minutes. For the detection of osteoblasts, sections were incubated with human runt-related transcription factor 2 (Runx2) antibodies (MBL Co. Ltd., Tokyo, Japan) at room temperature for 1 hour. Secondary antibody staining was performed in accordance with the manufacturer's protocol. Immune complexes were visualized using 3'3'-diamibobenzidine tetrachloride (DAB, Merck, Darmstat, Germany). Serial sections were also stained for tartrate-resistant acid phosphatase (TRAP), a marker of osteoclasts and osteoclast-like cells, as described previously [16]. Boxes measuring 5,000 μm×700 μm were virtually set in the central part of each defect. The mean numbers of Runx2- and TRAP-positive cells in each box were counted in the central part of each defect.
Statistical analysis
One-way analysis of variance was performed to analyze BV, the closure rate, and the numbers of Runx2/TRAP-positive cells. Each group was compared using the Tukey post-hoc test when a significant result was observed. The statistical analyses were performed using GraphPad Prism 5.0 (GraphPad Software, La Jolla, CA, USA). The level of significance was set at 0.05.
RESULTS
Healing progressed in all animals and was free of complications. No signs of postoperative infection were observed in any experimental animal.
Vertical bone augmentation
In the AB group rats, micro-CT images were taken just before the removal of plastic caps 12 weeks after the primary operation. The mean BV inside the cap was 8.5±2.4 mm3; this was in accordance with previous research done by our research team [14]. A macroscopic evaluation following the removal of the plastic caps also confirmed sufficient bone-like newly augmented tissue on the left of the calvarium; it was sufficient to fill the defects placed on the right of the calvarium. Since we reused the AB for the transplant, a histological assessment of bone quality was not done in the present study. Our previous study histologically revealed the presence of well-mineralized tissue with small amounts of cells and vessels inside the plastic cap [14]. All rats were able to undergo the secondary operation following the abovementioned protocol.
Micro-CT imaging analysis
An analysis of the micro-CT images revealed BV results that indicated a gradual increase in the radiopacity contrast in a time-dependent manner in the control group. Otherwise, BV in both the AB and the CB groups had consistently been maintained at a much higher level than in the control group at 0 to 12 weeks. No statistically significant difference was seen between the AB and the CB groups (Table 1). Reossification was caused by the extension of growths from the bony rims at the lateral sides of bone defects in all groups. In the AB and CB groups, the turning point of the healing process was confirmed to be between 4 and 8 weeks after surgery. In the micro-CT images of the AB and CB groups obtained at 0 to 4 weeks, many tiny radiopaque figures were confirmed inside the defects. In the images taken at 8 to 12 weeks, the number of radiopaque figures implies that the number of transplanted bone particles decreased, and vigorous bone reossification at the edges of the bone defects was confirmed. Minimal new bone was observed in the control group (Figure 2).
Table 1
Results of BV in critical defects obtained from micro-CT (mean mm3±SD)

| Weeks | Control groupa) | AB groupb) | CB groupb) | P value |
|---|---|---|---|---|
| 0 | 0 | 11.0±1.3 | 9.9±3.5 | <0.001 |
| 4 | 0.7±1.7 | 9.2±3.0 | 8.9±4.3 | <0.001 |
| 8 | 1.7±2.0 | 10.0±3.5 | 10.1±4.6 | <0.001 |
| 12 | 2.8±2.4 | 10.7±4.2 | 10.5±5.4 | <0.001 |
BV: bone volume, micro-CT: micro-computed tomography, SD: standard deviation, AB: augmented bone, CB: cortical bone.
a,b)P<0.05. Different uppercase letters within the same line indicate statistical difference in Tukey post-hoc analysis.
![]()

Histological analysis
Figures 3 and 4 show the histological sections at 12 weeks. In the H&E staining, bone reossification and a tendency for defect closure were confirmed in both experimental groups. Reossification in the CB group was more vigorous than in the AB group (Figures 3A and 4A). The defect closure rate was higher in the CB group than in the AB group and the control group (Table 2). In both experimental groups, reossification was more vigorous on the dura side than on the periosteal site. In the immunohistology (for osteoblast detection) of the CB group, few Runx2-positive osteoblasts were confirmed. In contrast, in the AB group, scattered Runx2-positive osteoblasts were observed (Figures 3B, 3C, 4B, 4C, and Table 2). In the TRAP staining (for osteoclast detection) of the 2 experimental groups, the same tendency of positive cell arrangement was confirmed as was observed for Runx2 immunostaining (Figures 3D, 3E, 4D, 4E, and Table 2).
 | Figure 3Representative histological observations of the critical defects at 12 weeks in the AB group.
(A) H&E staining, (B) Immunohistochemistry for Runx2 at low magnification, (C) Immunohistochemistry for Runx2 at high magnification, (D) TRAP staining at low magnification, (E) TRAP staining at high magnification (arrows, positive reaction; arrow heads, edges of bone defects).
AB: augmented bone, H&E: hematoxylin and eosin, Runx2: runt-related transcription factor 2, TRAP: tartrate-resistant acid phosphatase, D: dura.
|
 | Figure 4Representative histological observations of the critical defects at 12 weeks in the CB group.
(A) H&E staining, (B) Immunohistochemistry for Runx2 at low magnification, (C) Immunohistochemistry for Runx2 at high magnification, (D) TRAP staining at low magnification, (E) TRAP staining at high magnification (arrows, positive reaction; arrow heads, edges of bone defects).
CB: cortical bone, H&E: hematoxylin and eosin, Runx2: runt-related transcription factor 2, TRAP: tartrate-resistant acid phosphatase, D: dura.
|
Table 2
Results of histological bone defect closure rate and positive cell counting

AB: augmented bone, CB: cortical bone, Runx2: runt-related transcription factor 2, TRAP: tartrate-resistant acid phosphatase.
a,b,c)P<0.05. Different uppercase letters within the same line indicate statistical difference in Tukey post-hoc analysis.
![]()
DISCUSSION
The in vivo micro-CT system used in the present study enabled the observation of microscopic bone structures in small living experimental animals within a short time, and seems to be promising for the quantification of bone formation inside bony defects. Quantification of radiopacity in the micro-CT analysis showed that the BV of both experimental groups was maintained at the same high level. Since both reossified tissue and transplanted particles had the same degree of radiolucency, it was difficult to distinguish newly generated tissue from other radiopaque fragments. This could be the reason why BV in both the AB and the CB groups was consistently maintained at a much higher level.
From the histological sections of the AB and CB groups, we concluded that not only autogenous CB particles but also AB particles had meaningful regenerative ability. Furthermore, the regeneration ability of AB was shown to be inferior to that of a CB particulate transplant.
Bone regeneration can be accomplished through 3 different mechanisms: osteogenesis, osteoinduction, and osteoconduction. We hypothesized that the bone obtained from augmentation could be more immature than the CB particles and have active osteogenetic capacity. Consequently, more osteoblast-like and osteoclast-like cells were confirmed in the AB group than in the CB group. Therefore, osteogenesis in the AB group at 12 weeks could be regarded as high. In terms of the other mechanisms, the GBA bone did not have sufficient osteoconductive capacity because of its noncalcification tendency. Such disequilibrium of the 3 regenerative components in the AB could be attributed to the biological background underlying the limits of GBR bone.
In the present study, a bone substitute was not used in accordance with the fundamental space-making theory of GBR. Oginuma et al. [13] used the same rat GBA model and compared the usage of hydroxyapatite plus autogenous particulated bone with autogenous particulated bone alone for GBA. The presence of more mineralized tissue was confirmed in the case of the autogenous particulated bone alone. Gruber et al. [17] investigated the potential of cells that had grown out of CB grafts obtained in a cylindrical form and ground in a bone mill or harvested via drilling and aspiration. In their study, the CB particulate was consistently found to have similar cell viability and cell capacity to respond to mitogenic and osteogenic stimuli as compared to other forms of bone graft. Urban et al. [1819] reported that anorganic bovine bone-derived mineral mixed with autogenous particulated bone may be a suitable material for both vertical and horizontal augmentations. Thus, the same analysis for an AB derived from a space created with several types of bone substitutes is required for future studies.
The major factor related to healing other than the 3 regenerative components is time. The healing period is very important and crucial for defect healing and bone regeneration. In the histological sections of the AB group, at 12 weeks, sufficient defect closure was not confirmed. Since cells were scattered in this section, bone healing and regeneration was considered to be still under way at 12 weeks, and the AB had active osteogenetic capacity. Thus, more advanced bone healing will be observed if the observation period is prolonged. Furthermore, the period between primary surgery and secondary surgery is a very important factor. If we spend a long time in the observation of the GBA bone, the 3 regenerative components will be well balanced. Further studies are required to demonstrate how these factors are related to the regenerative ability of the GBA bone.
Autogenous bone has been considered the gold standard because of its osteoinductive and conductive properties. However, autogenous transplantation suffers from the limited availability of samples and patient morbidity. Thus, GBR is an extremely useful treatment method to obtain sufficient BV to place a dental implant, and GBR bone is a precious resource. In the case of osteoplasty or drilling for the implant placement for a GBA bone, bone particles of GBA bone could be generated. This study suggests that GBA bone has meaningful regenerative ability and that GBA bone particles can be reused as regenerative objects.
In conclusion, the regenerative capacity of AB in the occlusive space of a rat GBA model was confirmed. Within the limitations of this study, the regenerative ability of the AB particulate transplant was found to be inferior to that of a CB particulate transplant.
 XML Download
XML Download