

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The alveolar process is a tooth-dependent tissue that develops in conjunction with the eruption of the teeth, and its volume and shape are determined by the presence of the teeth [1]. Following extraction, the socket and residual bone undergo significant bone remodeling, which has been extensively studied in both preclinical [12], and clinical models [34]. Systematic reviews have shown that postextraction resorption of the alveolar ridge as much as 2.6–4.6 mm horizontally and 0.4–3.9 mm vertically occurs following tooth extraction [5]. These dimensional changes can cause various aesthetic and clinical problems. In order to overcome these obstacles, clinicians use various surgical or prosthodontic options. Guided bone regeneration (GBR) can be reliably utilized to restore the ideal alveolar ridge [6]. However, it is not an attractive option for patients, due to morbidity and complications such as swelling or hemorrhage following surgery [78]. Immediate or early implant placements can also be considered [910], but they may pose significant risks for aesthetic complications such as mucosal recession and lack of primary stability [1112], as well as involving high technique sensitivity.
Alveolar ridge preservation (ARP) is another treatment option for preventing postextraction dimensional changes [1314]. Systematic reviews and meta-analyses have evaluated the efficacy of ARP, and they have confirmed the occurrence of significantly less vertical and horizontal contraction at the alveolar bone crest following ARP [51516]. However, the scientific evidence is still insufficient for providing clear surgical guidelines for ARP [17]. In particular, there is little consensus on the degree of compressive force that should be placed on the grafting materials. For conventional GBR, a previous study reported that the degree of compressive force on the grafting materials crucially affected the amount of grafted bone particles within a defined space and hence also the rate of osteogenesis [18]. On the contrary, it is sometimes recommended to avoid overly intense compressive forces on the bone substitute particles in order to allow the in-growth of vascular elements, blood flow, and revascularization of the grafting materials [19]. Very recently, a report has described beneficial effects of compressive force during ARP in a preclinical model [20], but to the best of our knowledge, no such study has been performed in a clinical model.
Therefore, the aim of this study was to utilize radiographic, histomorphometric, and clinical analyses to compare 2 different compressive forces (5 N and 30 N) during ARP with deproteinized bovine bone mineral (DBBM) with 10% porcine collagen (DBBM-C) covered by a resorbable collagen membrane.
MATERIALS AND METHODS
Subjects
Patients were enrolled from August 2015 to March 2016 in the Department of Periodontology, Dankook University Dental Hospital. Twenty-four subjects (14 females and 10 males mean aged 55.3±8.9 years; age range, 37–72 years) who required the extraction of a single maxillary or mandibular molar tooth were enrolled in this study. The reasons for tooth extraction were periodontal lesions, dental caries, or fracture. Each residual extraction socket involved bone loss of less than 50% in all dimensions [21]. The exclusion criteria were pregnancy or lactation, a history of radiotherapy or chemotherapy for a malignancy in the past 5 years, autoimmune diseases, allergy to collagen, a history of systemic diseases that would contraindicate surgical treatment, long-term nonsteroidal anti-inflammatory drug therapy, requiring antibiotic prophylaxis, heavy smoking (>10 cigarettes per day), uncontrolled or untreated periodontal disease, and inability to provide consent for participation in the study or to accept the proposed treatment plan. The research protocol was approved by the ethical committee of Dankook University Dental Hospital, Korea (Approval No. H-1412/012/002).
Surgical procedure
All of the surgical procedures were performed by 1 specialist in periodontology (Jung Chul Park). Following the administration of local anesthesia (2% lidocaine with epinephrine at 1:80,000), the tooth was carefully extracted using luxators and extraction forceps to minimize trauma to the alveolar bone without flap elevation. The roots were separated in multirooted teeth with a high-speed handpiece and diamond bur if necessary. Meticulous debridement was performed with a surgical curette inside the extraction socket. The socket was irrigated with sterile normal saline solution.
Each extraction site was randomly assigned to 1 of 2 groups using a computerized randomization program (n=12 per group). In both groups, the sockets were grafted with 250 mg of DBBM-C (Bio-Oss® Collagen, Geistlich Pharma, Wolhusen, Switzerland) following tooth extraction. The DBBM-C was trimmed into 12 small pieces, and carefully packed into the extraction socket piece by piece. In the test group, 30 N of compressive force was applied for each compaction of biomaterials, and 5 N of force was applied in the control group. To control the applied force, a digital force gauge (Model DS2-50 N, Imada, Tokyo, Japan) with an A-6 extension shaft (6 mm in diameter) was utilized throughout the grafting procedure (Figure 1).
 | Figure 1Digital force gauge (Model DS2-50 N, Imada, Tokyo, Japan) (left) and extension shaft (right), (unit=mm).
|
After grafting, the grafting materials in both groups were covered with a resorbable collagen membrane (13×25 mm, Bio-Gide®, Geistlich Pharma) in a double-layered fashion [2223]. The hidden X suture technique was utilized (Ethilon 4-0, Ethicon, Cincinnati, OH, USA) and secondary healing was obtained [21]. Immediately after the surgery, a cone-beam computed tomography (CBCT) scan was performed with a resolution of 1 mm (scan time of 17 seconds, exposure time of 17 seconds, 80 kV, 7 mA; Alphard 3030, Asahi Roentgen Industries, Kyoto, Japan). The patients were prescribed antibiotics (Sultamox, Keunhwa, Seoul, Korea) and analgesics (Somalgen, Keunhwa) for 5 days and instructed about specific oral-hygiene methods. The sutures were removed after 10–14 days.
Harvesting of the tissue specimens and implantation
Approximately 4 months later, CBCT images were taken with the same settings as in the first scan. Before the placing the incision, bone and soft tissue biopsy samples were retrieved with a trephine bur (2.3×10.0 mm; Genoss, Seoul, Korea) along the original root axis of the extraction socket. A periosteal flap was elevated and implants (CMI IS active, Neobiotech, Seoul, Korea) were placed. In order to maximize the initial stability, the final drill was 1 size smaller than the final drill. Additional GBR was performed using the DBBM and a resorbable collagen membrane (Bio-Oss® and Bio-Gide®, Geistlich Pharma) if the residual buccal thickness was less than 1 mm or the thread of the fixture was exposed. Healing abutments were connected in all of the implants. The Periotest value (PTV) was measured at the buccal surface of the healing abutment using a Periotest M device (Medizintechnik Gulden, Modautal, Germany). The patients then received the same medications described above.
Radiographic analysis
The CBCT scans performed at baseline and at 4 months were used for radiographic measurements. The data were processed in the Digital Imaging and Communications in Medicine format. Superimposition of 2 scans was performed using stable reference points (e.g., the cranial base for the maxilla or the inferior border for the mandible, respectively), and an additional manual correction was performed for the best-matched cuts. Subsequently, CBCT measurements were made at baseline and 4 months from the cross-sectional images using the same reference points and lines [2124].
The measurement parameters were as follows (Figure 2):
 | Figure 2The measurement parameters of horizontal and vertical changes in radiographic images.
HW1, change in horizontal ridge width 1 mm; HW3, change in horizontal ridge width 3 mm; HW5, change in horizontal ridge width 5 mm; VHB, change in ridge height at the buccal crest; VMC, change in the vertical height measured at the mid-crestal area; VHL, change in ridge height at the lingual crest.
|
Histologic and histomorphometric analysis
All samples were fixed in individual containers with 10% buffered neutral formalin (Sigma Aldrich, St. Louis, MO, USA) for 2 weeks. After fixation, the specimens were processed with CalciClear Rapid (National Diagnostics, Atlanta, GA, USA) followed by thorough rinsing in running water. Specimens were processed with a tissue processor (ASP300S, Leica, Wetzlar, Germany) and then embedded in paraffin using an embedding center (Shandon Histocentre 3, Thermo Scientific, Waltham, MA, USA). Each specimen was cut into 4-µm-thick sections using a microtome (Model 2255, Leica), and the serial sections were stained with Masson trichrome or hematoxylin-eosin staining. Images of the sections were analyzed with the aid of an optical microscope (BX51, Olympus, Tokyo, Japan) equipped with a charge-coupled device digital camera (SPOT Insight 2Mp, Diagnostic Instruments, Sterling Heights, MI, USA) with an adapter (U-CMA3, Olympus). Photoshop version CS6 (Adobe Systems, San Jose, CA, USA) was used for image analysis. Each histologic structure was differentiated by a single researcher (Hyun Seung Shin) using a touch-pen and touch-screen system (Model DTF 720, Wacom Technology Corporation, Kazo, Japan) into 3 histological components: the residual graft, newly formed bone, and provisional matrix. The areas were measured and converted into percentages.
Statistical analysis
For sample size calculation, the percentage of newly formed bone (the primary outcome) in the study of Lindhe et al. [25] was used as the expected value in the control group, and it was assumed that the test group would have a 2-fold increase in the percentage of newly formed bone compared to the control group. To obtain 80% power with an alpha level of 0.05, the sample size required for the present trial was 8 patients per group. In the present authors' experience, it was expected that a high percentage of patients would drop out in a trial regarding implant therapy. The dropout rate was expected to be approximately 50%. Considering that projected dropout rate, the aim was set to enroll 12 patients per group (total number of patients=24).
For demographic analysis, the χ2 test was performed by gender, mandible/maxilla, and reasons for extraction. The independent t-test was performed for age. The data were presented as mean±standard deviation. The Shapiro-Wilk test was used as a test for normality. In the radiographic analysis, the data for HW3, HW5, VHB, VHL, and VMC were not normally distributed (P<0.05), whereas the other parameters were normally distributed (P>0.05). The Mann-Whitney U test was used to assess statistical significance for HW3, HW5, VHB, VHL, and VMC, and the independent t-test was used for other parameters. All analyses were performed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at P<0.05.
RESULTS
Twenty-four patients were initially enrolled, but 4 patients dropped out during the study due to loss of contact (Table 1). Consequently, 20 patients finished the study. All patients who completed the study were referred for prosthodontic treatment thereafter.
Table 1
Demographic information

![]()
Clinical observations
All the surgical sites showed uneventful healing without infection, inflammation, or other complications. At the time of implantation, all of the extraction sockets were covered with intact soft tissue, which had sufficient keratinized mucosa (Figure 3). No collagen membrane was present when the periosteal flap was reflected. Most of the sites exhibited satisfactory bone quantity and quality for implant insertion, with the exception of 2 surgical sites that needed an additional GBR procedure (1 from each group).
 | Figure 3Clinical photographs showing the procedures from extraction to implantation. The clinical procedures were identical in the 2 groups except for the magnitude of the compressive force used in bone grafting. (A) Preoperative; (B) Extraction; (C) Bone grafting; (D) Double-layered membrane; (E) Hidden X suture; (F) Stitch-out; (G) 1 month; (H) 3 months; (I) Biopsy and flap elevation; (J) Implantation and suture; (K) 2 weeks; (L) 2 months.
|
Radiographic analysis
The measurement of dimensional changes to the alveolar ridge after ARP using CBCT images revealed that the application of compressive force during ARP did not make a significant difference in the preservation of horizontal or vertical dimensions in comparison to the control group in which minimal compressive force was applied (Table 2, Figure 4). The vertical measurements showed that the height reductions at the buccal and lingual crests were −1.35±1.74 mm and −0.76±1.08 mm, respectively, in the control group, and −1.07±0.93 mm and −1.09±0.88 mm, respectively, in the test group. No statistically significant difference was found between the 2 groups (P>0.05).
Table 2
Horizontal and vertical changes of alveolar ridge dimensions

Values are presented as mean±SD.
HW1, change in horizontal ridge width 1 mm; HW3, change in horizontal ridge width 3 mm; HW5, change in horizontal ridge width 5 mm; VHB, change in ridge height at the buccal crest; VHL, change in ridge height at the lingual crest; VMC, change in the vertical height measured at the mid-crestal area; SD, standard deviation.
![]()
 | Figure 4Comparison of radiographic images taken after the ridge preservation (baseline) and after 4 months of healing before the implantation. (A) Baseline, test group; (B) 4 months later, test group; (C) Baseline, control group; (D) 4 months later, control group. White arrows indicate the apical boundary of the extraction socket. The graft materials are well impacted in the test group (30 N of compressive force), whereas an area of radiolucency can be observed along the boundary in the control group (5 N of compressive force), (scale bar=1 cm).
|
The horizontal measurements showed that the changes in the ridge width at 1 mm, 3 mm, and 5 mm below the ridge crest were −1.11±0.98 mm, −0.37±0.53 mm, and −0.27±0.86 mm, respectively, in the control group. In the test group, the changes in ridge width at 1 mm, 3 mm, and 5 mm below the ridge crest were −1.84±1.52 mm, −1.20±1.28 mm, and −0.38±0.50 mm, but no statistically significant difference was found between the groups (P>0.05).
Histological observations
A minimal inflammatory reaction was observed in 20 tissue biopsy samples obtained from the ARP sites. In both groups, the thick layer of keratinized mucosa was covered by the connective tissue, and a few loose particles were encapsulated inside the soft tissue. Many of the DBBM-C particles were surrounded by newly formed bone with close contact. In some specimens, the provisional matrix was observed along the surface of DBBM-C particles with little newly formed bone, and these were usually observed in the coronal portion. Interestingly, there was a number of DBBM-C particles clustered in the apical areas of the specimens in the test group. These small particles and other DBBM-C particles were interconnected by a newly formed bony bridge. In addition, finger-like bony projections from the native bone were observed in some areas of the specimens, and the newly formed bone showed a number of osteocytes.
Histomorphometric measurements
The results of the histomorphometric analysis are presented in Table 3, Figures 5, and 6. The area of residual DBBM-C particles was higher in the test group (28.26%±7.13%) than in the control group (22.14%±7.48%), but this difference was not statistically significant (P>0.05). However, the percentage of newly formed bone was nearly 2-fold higher in the test group (13.58%±5.59%) than in the control group (6.74%±7.01%), which was a statistically significant difference (P=0.033).
Table 3
Results of the histomorphometric measurements (in %) of specimens 4 months after ARP

Values are presented as mean±SD.
ARP, alveolar ridge preservation; DBBM-C, deproteinized bovine bone mineral with 10% porcine collagen; SD, standard deviation.
a)Statistically significant difference (P<0.05).
![]()
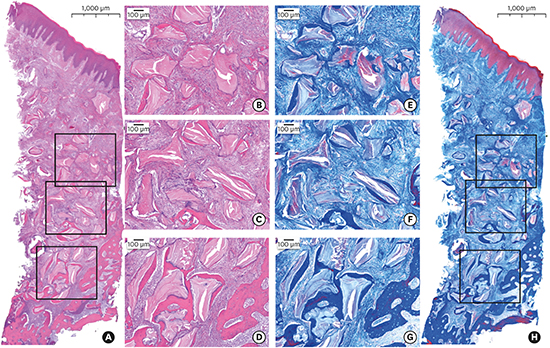
 | Figure 5Representative image of histologic specimens of the test group (30 N of compressive force). Hematoxylin and eosin (left panels, A, B, C, D) and Masson trichrome (right panels, E, F, G, H) staining. The inset boxes in the less magnified image indicate the relevant areas in the more magnified images.
|
 | Figure 6Representative image of histologic specimens from the control group (5 N of compressive force). Hematoxylin and eosin (left panels, A, B, C, D) and Masson trichrome (right panels, E, F, G, H) staining. The inset boxes in the less magnified image indicate the relevant areas in the more magnified images.
|
Initial stability analysis
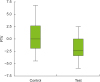
Implants were placed 4 months after ARP, and the initial stability of the implants as assessed using PTVs (Table 4). The average of the PTVs did not differ significantly between the test group (−1.78±2.52) and the control group (0.50±3.84) (P>0.05). The box plot with whiskers is presented in Figure 7.

DISCUSSION
In the present study, the comparison of the compressive force applied on the grafting materials during ARP was performed by radiographic, histomorphometric, and clinical analyses. In this study, primary closure following ARP was not intended at all and the sockets were left to heal. In conventional GBR procedures [8], the primary principle is that graft materials must be sealed by soft tissue [23]. However, interestingly, ARP without primary flap closure has also been shown to have satisfying results [14212627]. Additionally, the resorbable membrane exposed intentionally during ARP offers the advantages of preserving the surrounding keratinized tissue and decreasing chair time.
The compressive force was chosen based on the clinical experiences of the expert surgeons. The minimum force was determined by multiple reiterations of graft packing forces using the force gauge, and was determined to be 5 N. Meanwhile, the maximum compressive force was determined by applying the maximal force until the patients felt discomfort or pain, and was later determined to be 30 N. DBBM particles are known to be able to withstand a pressure of 35 MPa [28]. In previous studies [1820], 10 g, 20 g, and 100 g of force or 4.1 g and 8.2 g of force were applied in preclinical models, however, the defect shape and dimensions in these studies were sharply distinct from human molar tooth sockets, and a direct comparison was precluded.
The CBCT analyses performed in this study did not reveal any significant differences between the 2 groups. It was therefore assumed that the application of the compressive force did not interfere with the preservation of dimensions of the alveolar ridge. The mean horizontal and vertical changes in both groups were comparable to those reported in previous studies [21]; however, the quality of the augmented alveolar ridge should be histologically and clinically assessed as well. Therefore, in the present study, we additionally included the histological and clinical evaluations.
In the histologic evaluations, the biopsy samples of the 2 groups generally appeared similar at lower magnifications. In some areas of the specimens in the test group, finger-like newly formed bony projections with abundant osteocytes were observed, and new bone formation along the surface of particles was frequently observed. It seems that the microfractured small DBBM particles contributed to the production of new bone, helping the construction of the bony bridge. These specific histologic features were observed much more frequently in the test group, and they seem to be reflected in the histomorphometric observations of a higher percentage of newly formed bone formation. This is consistent with the findings of a preclinical ARP study using compressive forces [20]. It was assumed that the application of the compressive force accelerated the new bone formation due to stimulatory effects on angiogenesis and the higher expression of genes related to cell proliferation [31]. In addition, piezoelectric stimulation of osteoblastic activity was considered to be a possible mechanism [29]. Although the underlying mechanism has not been fully elucidated, the authors of the present study assume that the compressive force provided closer contacts between the particles for easier bony bridging, and also that the impaction of particles stabilized them [20]. Further studies are warranted to clarify the underlying mechanism.
The ratio of newly formed bone has varied over a wide range in previous studies; for example, Carmagnola et al. [30] reported 34.4% of lamella and woven bone, Zitzmann et al. [31] reported 22.6%, Araújo et al. [34] reported 14.7%, Cardaropoli et al. [14] reported 26.34%, and Park et al. [33] reported 9.88%. However, the exact compressive forces applied to the grafting materials were not reported in these studies, and the present authors therefore assume that the variability in these percentages could have been at least partly due to the application of uncontrolled compressive forces during the grafting procedure. Therefore, standard guidelines on the application of compressive force on graft materials should be immediately prepared for clinical applications and academic research.
PTV and resonance frequency analysis are 2 objective measurement methods currently used to assess the clinical stability of implants without damaging the implant-bone interface [34]. In this study, PTVs were measured, and the differences were not statistically significant between groups. However, from a clinical point of view, the operator reported that the compressed bone was felt to be much more rigid during site preparations. The impaction of bone particles may have reduced the space between particles and resulted in increased density, which has been previously demonstrated in the field of orthopedics [35]. It is expected that the application of compressive force during ARP would provide better mechanical strength for the implant placement. However, insufficient evidence exists regarding the impact of compressive force on the osseointegration of the implants. Further studies are required.
Within the limitations of this study, applying a greater compressive force to the grafting materials showed positive effects on new bone formation while preserving the alveolar ridge dimensions. The findings of this study could be used to develop guidelines for ARP procedures. However, further studies are needed to determine the most effective amount of compressive force.
 XML Download
XML Download