

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Implant therapy is considered a predictable treatment option rendering high implant and prosthesis survival rate when using fixed dental prostheses for replacing single- and multi-unit gaps [12]. These long-term favorable treatment outcomes have mostly been reported for implants placed in native bone or with only minor concomitant bone regenerative procedures and for implants with standard lengths and diameters. In the past years, implant lengths and diameters have continuously decreased. This shift was supported by the development of more favorable surface structures and more solid titanium alloys used for fabricating dental implants [345]. Moreover, patient demands for more minimally invasive surgical procedures, fewer complications, lower treatment costs, and less treatment time have resulted in a series of publications using dental implants with reduced dimensions, in terms of both diameter and length [678]. The primary goal following implant placement is to achieve osseointegration, a solid anchorage of the endosseous part of the implant within the bony envelope. Various methods have been developed to measure osseointegration and implant stability, including resonance frequency analysis (RFA) and histologic analyses [910]. On the basis of these outcome measures, bone formation and implant integration appear to follow a certain pattern that starts with the early phase of the bone resorption process [11], followed by a phase of bone apposition along the implant surface [12]. This results in dental implants demonstrating increasing RFA values and increasing bone-to-implant contact values over time [1314]. Thus far, threshold values for determining and predicting successful long-term outcomes have not been reported for either of these methods. One might, however, assume that an increase in the dimension of dental implants would result in clinically superior outcomes. However, this has not been documented thus far. In contrast, upon successful osseointegration and under healthy peri-implant conditions, attempts to break osseointegration have failed in preclinical experiments [1516]. These observations further support the decision to reduce implant dimensions and adapt them to the clinical situation. Therefore, the aim of the present narrative review is to describe treatment options in the posterior regions of the mandible and the maxilla, comparing short implants with long implants in augmented bone, and to propose a treatment concept based on current evidence.
SHORT DENTAL IMPLANTS
Short dental implants were defined as implants with an endosseous component of ≤8 mm [17]. These implants were predominantly introduced and clinically used for circumventing more extensive primary bone augmentation procedures such as lateral sinus augmentation [18]. However, the survival rates, according to the latter study, were lower than those of standard-length implants in identical clinical situations. Further, the development of new implant surfaces resulted in an increasing number of publications using short dental implants for a number of indications, thereby expanding the treatment options for fully and partially edentulous patients. From a clinical point of view and from a patient's perspective, short dental implants offer a number of clinical advantages: less skill necessary to perform the surgical intervention, less morbidity by avoiding more extensive bone augmentation procedures, easier removal in case of failure, and predominantly, an increased number of sites available for implant therapy. In contrast, clinicians might be worried about disadvantages including a high crown-to-implant ratio and a relatively high rate of biological and technical complications associated with potential overload. According to preclinical [192021] and clinical studies [22], as well as recent systematic reviews [72324252627], none of these possible limitations are clinically relevant. Exceptions include slightly increased failure rates of short implants in the posterior maxilla with soft bone present in comparison with the mandible [27] and a slightly higher rate of technical complications [28]. Moreover, longer-term studies have demonstrated that short implants exhibit implant survival rates and biological outcomes similar to those of long implants [293031].
SINUS ELEVATION
The maxillary posterior edentulous area presents a challenge to clinicians during the placement of dental implants because of the lack of bone height resulting from the resorption of the alveolar ridge and pneumatization of the maxillary sinus floor. This has led to the development of sinus augmentation techniques intended to increase the vertical bone dimension in the posterior maxilla in the cranial direction, allowing the placement of dental implants. Considering the residual ridge height, the most appropriate surgical technique and grafting protocol may be selected on the basis of the proposed treatment guidelines [32].
Sinus augmentation via a crestal or a lateral approach is routinely performed either primarily or simultaneously with implant placement, and is generally considered to result in predictable outcomes. Systematic reviews have demonstrated an overall implant survival rate well over 90% after sinus augmentation procedures [333435]. A recent systematic review reported that the implant survival rate after a minimum of 3 years of loading was 93.7% and 97.2% for sites augmented using lateral and crestal approaches, respectively [36]. Moreover, complication rates associated with sinus augmentation, such as membrane perforation, hemorrhage, and infection, were relatively low [37]. Despite successful outcomes, long healing periods needed to achieve an adequate level of new bone formation is a shortcoming for both clinicians and patients [3839].
VERTICAL AUGMENTATION
In case of a severely resorbed alveolar ridge in the posterior mandible, the available bone height for implant placement is often limited by the proximity of the inferior alveolar nerve. Vertical ridge augmentation could be an option for increasing the ridge dimension in order to place a standard-length implant. Moreover, this reduces the crown height of the implant prosthesis, which would otherwise result in an unfavorable crown-to-implant ratio, as well as the proximity of the restoration margin to the oral vestibulum, causing difficulties in maintaining proper oral hygiene [40].
Various surgical techniques have been developed for vertical ridge augmentation, including block bone grafting, distraction osteogenesis, and guided bone regeneration [41]. Among them, the autogenous block bone graft has been well documented and is still considered the gold standard [42]. A recent systematic review reported that the survival and success rates of implants placed in reconstructed ridges with autogenous bone blocks were similar to those of implants placed in native bone [43].
In contrast, unwanted volumetric resorption of an autogenous block bone graft is a concern for clinicians. The volume stability of the autogenous block bone remains controversial and has been reported to vary among clinical studies [444546]. These differences can be explained by the heterogeneity of the study designs, including different donor sites, different healing periods, different implantation times, and the use of barrier membranes. According to a review of studies with follow-up periods of at least 4 to 5 years, the resorption rate was the highest during the first year of grafting and appeared to stabilize afterwards [47]. As alternative candidates to the autogenous block bone, allogeneic or xenogeneic block grafts have been applied. However, scientific evidence for these materials is lacking, as the available data are limited to case series [48].
Alongside the many advantages of vertical augmentation, an increased rate of surgical complications and enhanced patient morbidity is associated with this type of procedure [49].
POSTERIOR MAXILLA: SHORT IMPLANTS VS. SINUS ELEVATION AND LONG IMPLANTS
In the posterior maxilla, a recent systematic review [50] included 8 clinical randomized controlled clinical trials (RCTs) with a follow-up period of up to 18 months after loading with final reconstructions. Based on the 5 studies reporting on long-term observation periods (16–18 months) [5152535455], a mean implant survival rate of 99.0% (95% confidence interval [CI], 96.4%–99.8%) for short implants and of 99.5% (95% CI, 97.6%–100.0%) for long implants in the augmented sinus was reported. Similar data were calculated with survival rates ranging between 97% and 100% for both groups on the restorative level. When discussing different treatment options with the patient, a clinician is confronted with challenges related to intraoperative, perioperative, and postoperative morbidity. On the basis of this information, a final decision is made to undergo a specific therapy. The most frequent technical complications included screw loosening in the reconstructions for both short and long implants, but few differences were found between the 2 treatment concepts. Further complications were predominantly observed because of the surgical interventions (i.e., membrane perforations). Short dental implants were responsible for 33% of the complications, whereas a sinus elevation procedure increased the risk of complications by 100%. This corresponds to as much as a 3 times higher risk of having an intraoperative complication when using long dental implants than when using short ones. These data are supported by observations that short dental implants offer further benefits in terms of less morbidity, lower costs, and a relatively short treatment time [555657]. At least on a short-term basis, short implants might be more appropriate, offering a variety of benefits in terms of patient-reported outcome measures, and still offer survival rates similar to those of long implants in the augmented sinus. A summary of the study characteristics is presented in Table 1.
Table 1
Summary of the RCTs comparing the treatment options of short implants vs. standard-length implants in combination with vertical bone augmentation procedures

| Region | Author | Year | Results |
|---|---|---|---|
| Maxilla | Esposito et al. [51] | 2011 | 5-mm short implants achieved similar if not better results to those of longer implants placed in an augmented bone. |
| Maxilla | Gulje et al. [52] | 2014 | 6-mm implants and 11-mm implants combined with sinus floor elevation surgery were equally successful. |
| Maxilla and mandible | Pistilli et al. [53] | 2013 | 6-mm long implants with a conventional diameter of 4 mm achieved similar if not better results than longer implants placed in an augmented bone. |
| Maxilla and mandible | Pistilli et al. [54] | 2013 | 5-mm implants achieved results similar to those of longer implants placed in an augmented bone. |
| Maxilla | Thoma et al. [55] | 2015 | Short implants may be more favorable in terms of short-term patient morbidity, treatment time, and treatment costs. |
| Maxilla and mandible | Esposito et al. [56] | 2012 | Short implants might be a preferable choice to bone augmentation, particularly in posterior mandibles. |
| Maxilla and mandible | Felice et al. [57] | 2009 | There was no statistically significant difference in patient preferences, as patients found both short and long implants acceptable. |
| Mandible | Esposito et al. [61] | 2014 | 5-mm short implants achieved results similar to those of longer implants in augmented bone. |
| Mandible | Felice et al. [62] | 2014 | The prognosis of short implants was as good as that of long implants placed vertically in augmented mandibles. |
![]()
POSTERIOR MANDIBLE: SHORT IMPLANTS VS. VERTICAL RIDGE AUGMENTATION AND LONG IMPLANTS
For the posterior mandible with a limited alveolar ridge height, 3 options exist: primary vertical ridge augmentation and subsequent implant installation, simultaneous implant placement with vertical ridge augmentation, and the use of short implants [57585960]. As in the case of the posterior maxilla, different treatment modalities were evaluated in recent RCTs [53546162]; however, the overall number of studies is limited. According to a recent systematic review [63], only 4 studies could be included, reporting on 135 patients who underwent restorations with 328 implants. The survival rates on the implant and prosthetic level have not been reported to be different in any study. However, an analysis of the rate of complications revealed certain differences. In the group with primary bone augmentation, even if some of the grafting procedures failed, all the short implants could be placed. This was reflected in a calculation of the overall number of complications in patients. In 56 out of 85 patients, complications were reported for the augmented group, whereas in the short dental implants group, only 18 patients were affected. The main complications included paresthesia of the mandibular nerve, predominantly in the augmented group [63]. Clinical recommendations favoring one procedure over the other have to be interpreted with caution, since the scientific evidence is based on few patients and research groups.
CURRENT TREATMENT CONCEPT
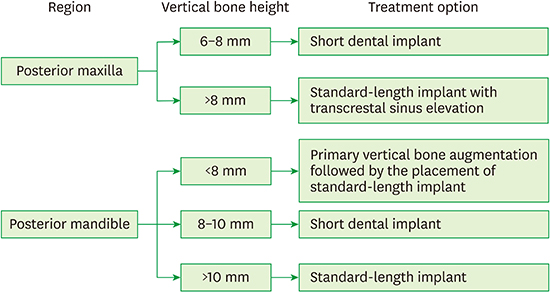
The clinical decision between these options (short dental implants or primary bone augmentation, followed by the placement of long dental implants) is based on a number of parameters. These parameters predominantly include scientific evidence, the surgical skill and experience of the surgeons and, increasingly, the patient's preferences. In order to support the clinician in the decision-making process and to inform the patient more extensively on the available treatment options, systematic reviews have summarized the available literature on high-level evidence from RCTs for the posterior mandible and maxilla (for an overview see: [5063]). For the posterior maxilla, short dental implants are the preferred option in cases with a vertical bone height of 6–8 mm (Figure 1). A transcrestal sinus elevation approach is chosen for a vertical ridge dimension exceeding 8 mm and if standard-length implants are the preferred option (Figure 2). In the posterior mandible, primary vertical bone augmentation using one of the abovementioned treatment options should be performed, followed by the placement of standard-length implants (Figure 3). Short dental implants are predominantly recommended in cases with a remaining ridge height of 8–10 mm, allowing the surgeon to place a 6-mm implant and including a safety distance to the alveolar nerve of 2 mm (Figure 4). In cases where more than 10 mm of the bone is available, standard-length implants are recommended (Figure 5). The decision-making process for the posterior maxilla and mandible is presented in Figure 6.
 | Figure 1(A) A treatment option for the posterior maxilla with a vertical bone height of 6–8 mm. (B, C) A short dental implant is recommended.
|
 | Figure 2(A) A treatment option for the posterior maxilla with a vertical bone height of more than 8 mm. (B, C) A transcrestal sinus elevation approach can be chosen for a vertical ridge dimension exceeding 8 mm and if standard-length implants are the preferred option.
|
 | Figure 3(A) A treatment option for the posterior mandible with a remaining ridge height of less than 8 mm. (B) Primary vertical bone augmentation should be performed, (C) followed by the placement of standard-length implants.
|
 | Figure 4(A) A treatment option for the posterior mandible with a remaining ridge height of 8–10 mm. (B, C) A short dental implant is recommended.
|


CONCLUSION
Short dental implants as well as standard-length implants in combination with vertical bone augmentation procedures appear to result in predictable outcomes in terms of implant survival rates. However, according to recent clinical studies comparing these therapeutic options, the use of short dental implants appears to have a number of advantages for the patients and the clinician.
 XML Download
XML Download