

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Due to the high success rate of dental implants [123], interest in reducing the duration of treatment by immediate or early loading is increasing among both dentists and patients. Many researchers have demonstrated the reliability of both the immediate and early loading of dental implants [456], and have stated that primary stability is an important prerequisite for the success of osseointegration and functional loading [67]. Moreover, primary stability is an important factor in determining the long-term success of implants [8], and establishing a high level of primary stability makes immediate and early loading slightly more reliable [9].
Following implantation, the primary mechanical stability provided by the macro-design of the implant is gradually replaced by the biological stability provided by osseointegration. At 2–4 weeks after implantation, primary stability declines and, unfortunately, secondary stability is not yet able to offset this decline, thereby resulting in a stability dip [10]. Since it is standard clinical protocol to load the implant after this stability dip [11], altering the timing of the stability dip would be beneficial for immediate or early loading. Efforts to overcome the stability dip have involved both primary and secondary methods. Primary methods are those that enhance the mechanical stability of the implant, such as using tapered implants [12], changing the shape of the implant thread [13], using under-drilling during implant insertion [12], and using implants with a microthread on the upper surface [14]. Secondary methods are those that increase biological stability by treating the implant surface in various ways; e.g., resorbable blasting media (RBM) [15], sandblasted, large-grit, and acid-etched (SLA) [16], and anodizing [17].
The objective and quantitative evaluation of implant stability is a key factor in determining the time to start loading. Currently, there are 2 methods for evaluating implant stability that are scientifically verified and commonly used. First, cutting torque resistance analysis is a one-time, invasive method implemented at the time of implantation that provides information about mechanical stability [18]. During the placing an implant, the torque (Ncm) is measured and displayed on the screen of an implant engine; typical measurements are in the range of 5–50 Ncm, and a torque of at least 30 Ncm is recommended for sufficient initial fixation [8]. Second, resonance frequency analysis (RFA) is evaluated by using a converter to measure the resonance frequency of an implant; this is a non-invasive method that can be used multiple times during and after installation [19]. Barewal et al. [20] reported that RFA was appropriate for examining changes in implant stability during the initial healing period, and that it was sensitive enough to detect changes in implant stability over time based on comparisons with peri-implant bone density. The Osstell® Mentor (Integration Diagnostics AB, Göteborg, Sweden) is a commercially available device that converts resonant frequencies of 3,500–8,500 Hz into an implant stability quotient (ISQ) graded from 0 to100. Although there are not yet any clear standards for the normal range of ISQ values of successfully osseointegrated implants, most studies have shown a range of 57–82 (mean, 69) [212223].
Many commercially available implants have been surface-treated by various methods to overcome the stability dip. However, considerable debate still exists about the optimal surface treatment method based on mechanisms of osseointegration [2425]. The primary objective of this study was to monitor the stability of SLA implants with different diameters during the early phases of healing by RFA. The secondary objective was to evaluate how the initial stability of implants varied depending on different surface modifications and other contributing factors.
Go to : 
MATERIALS AND METHODS
Materials and subjects
The subjects in this study were patients who visited the Department of Periodontology, Pusan National University Dental Hospital and underwent dental implant surgery between March 2013 and August 2014. Preoperative clinical and radiological examinations were used to select patients suitable for the study. Specifically, patients were selected who had sufficient bone width to support an implant of the required diameter. This study was conducted after receiving approval from the Pusan National University Dental Hospital Institutional Review Board (No. PNUDH-2013-002).
There were 20 subjects in total (male, 10; female, 10), with an average age of 54.95±24.95 years, and a total of 35 implants (SLA, 25; RBM, 10). Prior to implant surgery, all patients underwent the appropriate periodontal examinations and treatment according to their periodontal health status, including oral hygiene instruction, scaling and root planning, and surgical periodontal treatment.
The following exclusion criteria were defined: 1) poor oral hygiene (full mouth plaque score ≥15% [26]), 2) any uncontrolled systemic disease that could influence the outcome of implant therapy, 3) pregnancy, 4) smoking (≥20 cigarettes/day), 5) aggressive periodontitis, 6) anterior tooth implant, 7) requiring additional bone graft, and 8) being unable to receive 1-staged surgery due to a failure to ensure fixation with an final torque of ≥30 Ncm.
The implant fixtures were the Dio® UF HAS (Dio Co. Ltd., Busan, Korea) for the SLA implants, and the Osstem® USII plus system (Osstem Implant Co. Ltd., Seoul, Korea) for the RBM implants.
Surgical procedure
Following intraoral and extraoral sterilization, infiltration anesthesia was applied to the surgical site using 2% lidocaine HCl with 1:100,000 epinephrine (Yuhan Co. Ltd., Seoul, Korea). After making an incision in the alveolar ridge, a full-thickness flap was reflected and the osteotomy was performed under saline irrigation while increasing the drill diameter in accordance with the manufacturer's instructions. After confirming an implantation torque of at least 30 Ncm, a 1-stage method was selected, and the flap was sutured (Figure 1). For the first 3 postoperative days, patients were administered amoxicillin (Kymoxin®, Yuhan Co. Ltd.), acetaminophen (Tylenol®, Janssen Korea Ltd., Seoul, Korea), and pancreatic enzyme replacement (Bearse®, Daewoong Pharmaceutical Co. Ltd., Seoul, Korea), and were instructed to use a 0.12% chlorhexidine gluconate solution (Hexamedin®, Bukwang Pharmaceutical Co. Ltd., Seoul, Korea), until the sutures were removed. The sutures were removed on postoperative day 7. All patients showed good postoperative healing.
 | Figure 1Clinical photography of 1-stage implant surgery. (A) Preoperative view. (B) Flap was reflected via midcrestal incision. (C) The final osteotomy was performed according to the manufacturer's protocol. (D) After confirmation that the initial stability of the fixture was at least 30 Ncm, a healing abutment was connected. The overlying flap was repositioned using single interrupted sutures.
|
Evaluation of initial stability
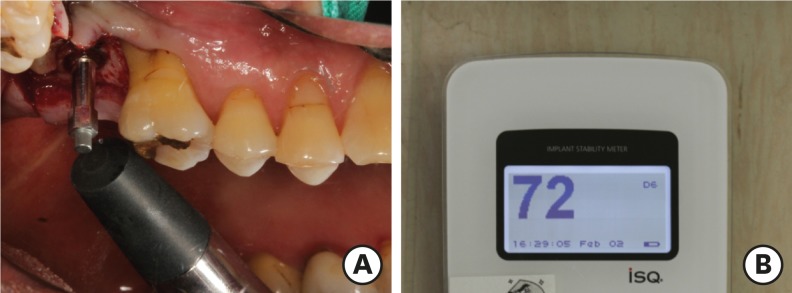
After attaching a magnetic peg (Smartpeg™, Osstell AB, Göteborg, Sweden) to the fixture, the Osstell® Mentor was used to measure the ISQ in both the buccal and lingual directions, and the mean of these measurements was then calculated (Figure 2). This method was used to evaluate initial stability at the time of implantation and at 1, 2, 3, 4, 6, and 10 weeks postoperatively. Changes in the mean ISQ and the magnitude of ISQ changes were analyzed according to several parameters (surface treatment method, implant diameter, dental arch, and sex) in order to examine their correlations with implant stability.
Statistical analysis
Intergroup comparisons were performed for various parameters using the ISQ values measured at each time point, including the ISQ value immediately after implantation. The Student's t-test was used to verify the statistical significance of intergroup differences by surface treatment, dental arch, and sex. One-way analysis of variance was performed to analyze differences by implant diameter. The Scheffé's test was chosen for post-hoc analysis. The significance level used for hypothesis testing was 0.05. All statistical analyses were performed using SPSS version 20 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
The distribution of subjects by surface treatment, diameter, and implant location is displayed in Table 1.

Comparison of initial stability by surface characteristics
Comparison of ISQ values at different time points
The RBM group showed a higher ISQ than the SLA group immediately after implantation (week 0), while the SLA group showed a higher ISQ than the RBM group at week 10, but these were not statistically significant differences. The stability dip occurred at week 1 for the SLA group and at week 2 for the RBM group. After the stability dip, both groups showed a gradual increase in the ISQ, and in weeks 4 and 6, the ISQ of the SLA group was significantly higher than that of the RBM group. The time at which the ISQ recovered to a level higher than week 0 was at week 2 for the SLA group and week 10 for the RBM group (Table 2).

Table 2
ISQ values at implant placement and examination time points according to the characteristics of the implant surface (mean±SD)
ISQ: implant stability quotient, SD: standard deviation, SLA: sandblasted, large-grit, and acid-etched, RBM: resorbable blasting media.
a)Statistically significant difference between the 2 groups (P<0.05).
![]()
Comparison of the change of the ISQ at different time points
In SLA group, which showed a stability dip at week 1, all the changes were positive except for the period from week 0 to week 1, and the change from week 1 to week 2 was the largest of the entire observation period. We observed a statistically significant difference in the changes between the groups from week 1 to week 2, corresponding to the fact that the stability dip took place at week 2 in the RBM group. The change in the ISQ from week 0 to week 10 was likewise significantly greater in the SLA group (Table 3).

Table 3
Changes of mean ISQ values according to the characteristics of the implant surface (mean±SD)
ISQ: implant stability quotient, SD: standard deviation, SLA: sandblasted, large-grit, and acid-etched, RBM: resorbable blasting media, W: week.
a)Statistically significant difference between the 2 groups (P<0.05).
![]()
Comparison of initial stability in the SLA group by diameters
Comparison of ISQ values at different time points
The 5-mm implants showed a significantly higher ISQ at each point except for weeks 6. In addition, the 4-mm implants showed a stability dip at week 2, unlike the SLA group as a whole or the 5-mm implants, which showed a stability dip at week 1 (Table 4).

Table 4
ISQ values at implant placement and examination time points according to the diameter of the implant in the SLA group (mean±SD)
ISQ: implant stability quotient, SD: standard deviation, SLA: sandblasted, large-grit, and acid-etched.
a)Statistically significant difference between the 2 groups (P<0.05).
![]()
Comparison of initial stability according to other variables
Mandibular implants showed a higher ISQ throughout the entire period, and the differences at weeks 2, 3, and 6 were statistically significant (Table 5). Male patients showed a higher ISQ throughout the period of the study, but the difference was statistically significant at week 10 (Table 6).


Table 5
ISQ values at implant placement and examination time points according to the location of the implant (mean±SD)
ISQ: implant stability quotient, SD: standard deviation.
a)Statistically significant difference between the 2 groups (P<0.05).
![]()
Table 6
ISQ values at implant placement and examination time points according to sex (mean±SD)
ISQ: implant stability quotient, SD: standard deviation.
a)Statistically significant difference between the 2 groups (P<0.05).
![]()
Go to :
DISCUSSION
ISQ measurement using the Osstell® Mentor is widely used in clinical practice because this method is non-invasive and replicable. However, unlike insertion torque, there are conflicting results as to whether ISQ is positively correlated with bone quality [202127], and it is not possible to directly compare ISQ values across different implant systems [8]. Huwiler et al. [28] reported that since there is no proven normal range for ISQ values, it is essential to make multiple measurements, rather than a single measurement, throughout the healing process in order to reliably evaluate implant stability. Thus, our analysis and observations focused on the range of ISQ values and patterns of change.
In a recent Cochrane review, immediate loading was defined as loading the implant within 1 week of insertion, and early loading was defined as loading the implant between 1 week and 2 months after insertion [29]. Testori et al. [22] and Lindeboom et al. [23] have suggested an ISQ threshold of ≥65 for immediate loading. In the present study, the mean ISQs at the time of implantation were over 80 in both groups, and the lowest ISQ value at the point of the stability dip was over 65. Therefore, both types of implants can be candidates for immediate or early loading, with their initial stability confirmed via the ISQ. However, based on the observations that the ISQ in the SLA implants was significantly higher than in the RBM implants at week 4 and week 6, the fact that the stability dip was 1 week earlier in the SLA implants, and the recovery to the initial ISQ was faster in the SLA implants, it can be concluded that the SLA surface is therefore more suitable for immediate loading (before 1 week).
Conflicting results have also been reported regarding the relationship between implant diameter and initial stability. Quesada-García et al. [30] reported that a larger implant diameter had a positive effect on initial stability, while Boronat López et al. [31] claimed that there was no association between implant diameter and stability. In our study, among SLA implants, the 5-mm implants had a significantly higher mean ISQ, suggesting that a larger implant diameter had a positive effect on initial stability. However, from a clinical perspective, our finding that the minimum ISQ of the 4-mm implants was far higher than the threshold ISQ [2223] is consistent with that of Ohta et al. [32], who reported that even if wider implants show a higher ISQ, the difference is not significant.
In 4-mm SLA implants, early loading is recommended to be performed after 2 weeks, as the stability dip was observed at week 2, unlike the SLA group as a whole. Because there was no 4-mm RBM group in this study, we compared the 4-mm SLA implants with the 5-mm RBM implants. At weeks 0, 1, and 2, the 4-mm SLA implants showed a lower ISQ than the 5-mm RBM implants, although the 2 groups had similar ISQ values at week 3. Subsequently, at weeks 4 and 6, the 4-mm SLA implants had a higher ISQ; at week 10, although the 5-mm RBM implants had a slightly higher mean ISQ, the difference between the groups was not significant. This tendency suggests that SLA surface treatment has a positive effect on initial implant stability, particularly after the stability dip, and that this could offset the effects of diameter. However, this conclusion requires additional research with a more appropriate design, including a control group with the same diameter.
When analyzing the change in the ISQ of the 4-mm SLA implants, the change from week 3 to week 4 was significantly larger than that of the 5-mm implants. We were unable to find any other papers providing evidence that could explain this phenomenon. However, one could consider the observations that greater changes in stability have been reported in less dense bone [1920], and that implants with a high initial ISQ have been found to show less significant changes during healing, while implants with a lower initial ISQ tend to show a greater rise in stability [333435]. This suggests that the 4-mm implants showed a more rapid increase in stability because they had a relatively lower initial stability.
With respect to differences in stability by implant location, stability has generally been reported to be lower for the maxilla than for the mandible because of differences in bone quality [3637]. In the present study, we observed similar results. However, since the ISQ for the maxillary implantation group also exceeded the threshold ISQ throughout the study period, it is thought that the difference in stability between the maxilla and the mandible does not have great clinical significance, as long as the final torque is confirmed to be at least 30 Ncm.
An analysis by sex showed a significantly higher ISQ in men at week 10. Studies in post-menopausal women have shown conflicting results regarding differences in ISQ according to sex. Zix et al. [27] studied women with a mean age of 32.1 years, and reported a significantly higher ISQ in men, similarly to our study. Conversely, Boronat López et al. [31] and Brochu et al. [38] reported a higher ISQ in women, in studies where the mean age of the subjects was around the 40s. As the mean age of the women in our study was 59 years, all were estimated to be of post-menopausal age. Taken together, these results suggest that the ISQ decreases after menopause, owing to the gradual decline in bone density. However, the mean ISQ value for women in our study was considerably higher than the threshold ISQ, meaning that the differences between genders in implant fixation are not of major clinical significance, as long as the final torque is established to be at least 30 Ncm.
The implant fixtures used in this study are all suitable for immediate or early loading under the right conditions, irrespective of surface treatment or diameter. In implants where an implantation torque of at least 30 Ncm was confirmed, larger implant diameter and SLA surface treatment showed a positive effect on initial implant stability.
Go to :
 XML Download
XML Download