

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
On July 1, 2013, the Korean government implemented an initiative to improve access to dental care, focused on adults. In this large step forward in the attempt to achieve universal healthcare coverage, dental scaling benefit coverage was provided under the Korean National Health Insurance (KNHI), in the form of once-yearly plaque and calculus removal for all adults ages 20 years and older [1].
This governmental initiative was designed to improve the prevention of periodontal disease, as it provided coverage for all Korean adults, including large swathes of the population previously not covered by public insurance. Furthermore, it was directly related to national health policy, as it sought to reduce financial barriers to access for dental care for all citizens, irrespective of their socioeconomic background and/or residential location [2]. Such a large commitment required the KNHI system to increase access to dental services by substantially lowering cost-sharing at the time of service [34].
Previous studies have confirmed that this national intervention to increase the provision of dental care positively impacted access to dental care within the Korean population. Jang et al. [5] showed that the dental scaling rate increased nationally over a recent 6-year period, particularly in 2014; this was likely a result of changes in the national health coverage of dental scaling. Park et al. [3] examined the impact of changes in coverage for KNHI dental benefits, including scaling. After the new policy was implemented, a nationwide analysis revealed a decrease in the prevalence of unmet dental care needs, and an increase in the likelihood of preventive dental care utilization (e.g., simple scaling, sealant, and fluoride treatment) over the course of a year after the intervention compared with the same measures in the period before coverage expansion. Conversely, Lee et al. [6] reported an increase in total periodontal treatments (periodontal flap operations, bone grafts for alveolar bone defects, and guided tissue regeneration) for patients covered by the KNHI, highlighting that the expansion of public health insurance for dental treatment might increase the number of patients diagnosed with periodontal disease.
However, even though a before-after comparison has demonstrated an increase in dental visits, this increase may not be attributable to these specific changes in dental health policy, so those results may be misleading. Additionally, the design of that comparison did not control or adjust for underlying secular trends, so it may have failed to adequately capture policy trends [789]. Finally, it was not able to minimize threats to internal validity, including random fluctuations, history, and maturation; these extraneous events and changes over time may have impacted the results. Therefore, the real effects of recent Korean dental policy changes remain an important empirical question.
This study drew on KNHI claims data over a 6-year period to evaluate the immediate and lasting impacts of expanded dental insurance coverage, including scaling, on dental care utilization. This study utilized a strong quasi-experimental design to test the hypothesis that implementation of this new health policy increased the usage of dental outpatient services.
MATERIALS AND METHODS
Data and study population
A database of KNHI claims was obtained from the Health Insurance Review and Assessment (HIRA) office, which also approved the analysis protocol. This study was granted an exemption by the Institutional Review Board of Korea University, Seoul, Korea (KU-IRB-15-EX-252-A-1). The KNHI claims database includes information about both principal and additional diagnoses, as well as hospitalization/outpatient treatment, examination dates, medical fees, medical services provided, prescribed medications, hospital codes, and patient demographics (age and sex). All data are arranged according to the claims made by medical institutions, based on the contents of the patient's examinations.
We included data filed by tertiary hospitals, secondary hospitals, general dental hospitals, and primary dental clinics, and restricted the analysis to outpatients with health insurance, aged 35–64 years (n=65,562,198), from June 2010 through November 2015. The pre- and post-policy intervention periods were from July 1, 2010 through June 30, 2013 and from July 1, 2013 through November 30, 2015, respectively.
When a patient visits a dental clinic for scaling, a general or specialized dentist must designate a primary diagnosis of periodontitis (K05) based on the Korean Classification of Disease, sixth edition, which is a modified version of the International Classification of Disease, tenth revision that is used by the KNHI. The primary diagnoses were further stratified according to criteria proposed by the American Academy of Periodontology [10]: acute gingivitis (K05.0), chronic gingivitis (K05.1), acute periodontitis (K05.2), chronic periodontitis (K05.3), periodontosis (K05.4), other periodontal disease (K05.5), and unspecified periodontal disease (K05.6). Importantly, multiple claims data records are generated when a patient is examined at several different hospitals, or is examined at a single hospital for multiple conditions. We identified medical records based on individual patients, using a KNHI-designed structured identification code to identify individual patients. Next, we defined study patients as those with a diagnosis of gingivitis (K05.0, K05.1) or advanced periodontitis (K05.2–K05.6) who received dental scaling. Using this approach, we analyzed the aggregated monthly data for a total of 45,650,000 outpatients throughout the entire analysis period.
Study variables
Data on age, sex, and residence area were collected for each study subject. Areas of residence were categorized as either a ‘metropolis’ (Seoul, Gyeonggi, Incheon, Daejeon, Daegu, Gwangju, Busan, and Ulsan) or a ‘small or medium-sized city’ (Gangwon, Gyeongnam, Gyeongbuk, Jeonnam, Jeonbuk, Chungnam, Chungbuk, and Jeju). The dependent variable describing dental service utilization was defined as the total outpatient cost for dental services, with the exception of prescription drug expenditures. The total dental cost was calculated as the sum of the total dental outpatient costs. All dental costs were adjusted for inflation, relative to the level of medical costs in 2010.
Statistical analysis
Data were analyzed at a secure location inside the HIRA to ensure strict confidentiality, after de-identification of the data for our analyses. A segmented regression analysis of interrupted time-series was performed to analyze time-series trends in dental costs before and after policy implementation, as well as immediate changes in dental costs [911]. This approach utilized a statistical test to assess the effects of the policy intervention, based on noticeable changes under the policy, as follows:
Here, Yit is an analysis-dependent variable (i.e., total outpatient dental costs) during a time period t for uniti, which changes on a monthly basis between July 2010 and November 2015. The coefficient (β1×time) measures a continuous variable, beginning with the value of 1 for July 2010 and increasing by 1 each month; this represents a monthly time-series trend. The coefficient (β2×policy change) is a binary indicator representing policy implementation in July 2013, possessing the value of 0 before July 2013 and 1 beginning in July 2013. It represents the immediate change in dental costs after policy implementation. The coefficient (β3×time after policy changed) is a continuous variable, beginning with the value of 0 and increasing by 1 each month; its non-zero values begin in July 2013, and it represents a time-series trend after policy promulgation. Xit λ accounts for the independent variables (i.e., age, sex and residence area). The term uit is the error term.
To detect seasonality, 4 season indicators were applied, using dummy variables where appropriate. The Durbin-Watson statistic was calculated to test for serial autocorrelation of the error terms; if necessary, the estimation models were used to adjust the autocorrelation. Values close to 2.00 indicated no serial autocorrelation [9]. All analyses were conducted using SAS 9.3 software (SAS Institute Inc., Cary, NC, USA); test results with P values <0.05 were regarded as statistically significant.
RESULTS
Descriptive results
The general characteristics of the patients and the results of the analysis are summarized in Table 1. From a database of 45,650,000 dental outpatients who were diagnosed with periodontal disease and received dental scaling, there were 8,046,685 patients with gingivitis and 37,602,621 patients with advanced periodontitis. These patients were 47.1% male and 52.9% female; their age (mean±standard deviation) was 49.4±11.8 years. The proportion of outpatients who received dental scaling during the observational period was highest in the 45 to 54-year-old age group.
Table 1
General characteristics of the study subjects over the 6-year analysis period (July 2010 through November 2015)

a)Patients with a primary diagnosis of periodontitis (K05) who received scaling; b)Classified as metropolises: Seoul, Gyeonggi, Incheon, Daejeon, Daegu, Gwangju, Busan, and Ulsan; c)Classified as small and medium-sized cities: Gangwon, Gyeongnam, Gyeongbuk, Jeonnam, Jeonbuk, Chungnam, Chungbuk, and Jeju.
Table 2 displays the number of patients and average medical cost per capita, distributed across 3 age groups, before and after the expansion of dental scaling coverage. Relative to the pre-policy period, the number of patients with either gingivitis or advanced periodontitis, and the average dental cost per capita, increased in all age groups.
Table 2
Comparison of the number of outpatients and total dental costs by age group in the pre- and post-policy intervention periods

Results for dental outpatient utilization trends
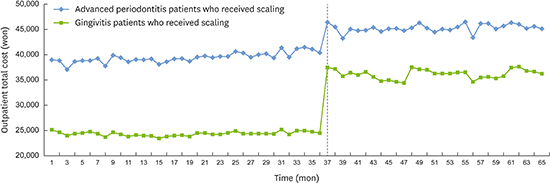
There were changes in the monthly average total cost per dental outpatient between July 2010 and November 2015. The total medical cost increased gradually following the introduction of the new policy (Figure 1). The numbers of patients with gingivitis or advanced periodontitis who received dental scaling per outpatient utilization are shown in Figure 2. Beginning in July 2013, the total medical cost increased immediately in both outpatient groups.
Figure 1
Trends in the total average dental cost per month over the period of the study (July 2010 through November 2015). The dashed line indicates the implementation of the new health policy.

Figure 2
Trends in the average dental costs per month by patient diagnosis, including advanced periodontitis patients who received scaling and gingivitis patients who received scaling, over the period of the study (July 2010 through November 2015). The dashed line indicates the implementation of the new health policy.

Results of the segmented regression analysis of interrupted time-series
Policy changes were assessed to identify their effects on dental cost per patient, using segmented regression analysis of an interrupted time-series (Table 3). After the policy change was implemented, there was an immediate statistically significant change in the observed total dental cost per patient, which increased by 18% after adjustment for age, sex, and residence area. Although there was a slight decrease in the time after policy changed variable following the introduction of the policy, there was an upward trend in the time factor during the analysis period.
Table 3
Segmented regression of the interrupted time-series analysis of dental cost during the period of the study

Both the gingivitis and advanced periodontitis outpatient groups exhibited an increase in total costs following policy implementation. We found that the dental costs for gingivitis outpatients increased immediately by nearly 47% following policy implantation, compared with an increase of 15% in the costs for advanced periodontitis outpatients. There was a statistically significant upward trend in the overall time variable.
DISCUSSION
In this study, we assessed the impact of public health insurance changes on the utilization of dental services in a large database of Korean patients, and accounted for the long-term effects of the policy, including a 36-month pre-intervention period and a 29-month post-intervention period. To our knowledge, no previous study has measured the temporal impact of compulsory dental care coverage benefits for adults. Our analysis allows a deeper understanding of the long-term trends triggered by this change in policy, rather than simply evaluating short-term trends, as was done in previous studies.
Our results suggest that this policy change led to an immediate increase in dental service visits for scaling treatment, indicating that the policy made significant advancements toward the policy objective of improving accessibility by eliminating barriers to access to dental care. Additionally, the trends we observed in this study indicate constant movement in a positive direction during the period of analysis; this impact is on-going.
Our study is broadly consistent with previous research suggesting that decreased co-payments are associated with improved utilization of dental services. A recent study carried out in the United States (US) yielded findings similar to our own, thereby highlighting the importance of dental care coverage expansion within a broader healthcare policy; this would increase the number of yearly dental visits [12]. Other studies have linked reductions in out-of-pocket payments for dental services (under public insurance) with increased access to preventive dental care services. In the US, Medicaid adult dental coverage has been associated with a significant increase in the likelihood of undergoing an annual dental visit, compared with states where residents do not receive public insurance dental coverage [13]. Nasseh and Vujicic [14] found that the newly-introduced State Children's Health Insurance Program significantly increased the rate of dental care use in children from low-income families; similarly, avoidance of necessary dental care due to financial reasons declined, likely due to lower prices.
Further, we analyzed pre- and post-policy dental costs and stratified the costs according to diagnosis, focusing on patients with gingivitis and advanced periodontitis who received dental scaling. Implementation of the policy increased the use of dental outpatient services by 47% and 15% in patients with gingivitis and advanced periodontitis, respectively; this policy effect appears to be sustainable. Importantly, the advanced periodontitis patients who received dental scaling may have experienced a remarkably positive effect. Thus, improving treatment accessibility for potential periodontal disease patients may facilitate appropriate disease management.
The impact of the expansion of preventive dental services benefits on dental use is a major concern for policy-makers because of the prevalence of periodontal disease, which is a chronic inflammatory disease in which periodontal tissues are destroyed due to dental plaque formation on the tooth surface [1516]. The prevalence of periodontal disease has increased each year in Korea [17]. When teeth are lost due to periodontal disease, patients experience serious problems, including reduced speech capacity and social communication, which may negatively affect both health and quality of life [181920]. Therefore, it is critical to identify effective policies for addressing periodontal disease.
Routine dental care, scaling, and consistent supportive periodontal therapy following periodontal treatment have all been strongly emphasized as effective approaches to reduce the incidence of tooth loss and periodontal disease. Notably, it is necessary to maintain periodontal health through continuous professional oral care, rather than one-time management of severe disease [2122]. Therefore, it would be beneficial to gradually expand this policy to provide preventive dental treatment benefits for a variety of oral diseases.
We acknowledge that there are limitations to our study. First, an analysis of the effects of a policy intervention requires control groups to compare differences between the pre- and post-intervention periods; however, the current study contains no control group, allowing for confounding effects from other factors. Dental costs reflect a variety of factors, including income level, health behaviors, health status, and market environment/competition [23], that were not considered in this study. Second, we cannot examine the details of non-reimbursable treatments received by patients who were diagnosed with gingivitis prior to July 2013 because the data we analyzed did not contain these details. Importantly, before the implementation of the new dental policy, the cost of medical treatment for patients with gingivitis was not covered by insurance; this coverage only became a standard benefit after the implementation of the policy. This study only included dental costs, ignoring the behaviors of the dentists providing treatment. The increased use of dental care services by patients may be driven by incentive demand within the medical provider community [11]. Since Korea utilizes a fee-for-service system, reimbursements for KNHI-covered dental benefits received by dentists can affect the outpatient care rates. Finally, we only considered patients who received scaling with the diagnosis of periodontitis. In future studies, it will be necessary to accurately evaluate dental outpatient treatment with the addition of detailed prescription codes.
This study demonstrated the importance of policy-based dental scaling coverage expansion. The introduction of the new policy provided both immediate and long-term impacts on the outpatient utilization of dental scaling treatments in Korea. While the policy was intended to entice patients to prevent periodontal disease, thus benefiting the insurance system, our results show that it also increased treatment accessibility for potential periodontal disease patients. When developing new dental healthcare policies intended to expand public health insurance, policy-makers should consider the effects of the policy on patient monitoring and follow-up. Additionally, the comprehensive effects of policy implementation should be more extensively evaluated, including those that affect the longer-term oral health of the nation.
 XML Download
XML Download