

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontal disease occurs because of interactions between host inflammatory and immune systems and bacterial complexes [12]. These bacterial complexes are also found in periodontally healthy individuals, and disease occurs when the balance between host defense and bacterial complexes is disrupted [3]. The normal oral microbial flora contains more than 700 bacterial species, among which over 300 species can be cultured in periodontal pockets. In particular, red complex bacteria such as Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola are strongly related to periodontal disease [456].
Several studies have reported the prevalence of putative pathogens in healthy populations and periodontal diseases in different populations. Studies in children confirmed the presence of P. gingivalis, T. forsythia, and Aggregatibacter actinomycetemcomitans in the absence of obvious gingivitis [78]. It also has been reported that infants, children, adolescents, and adults with clinically healthy periodontal status have a relatively large number of periodontopathic bacteria [9101112]. Therefore, the presence of periodontal pathogenic bacteria is not the only factor affecting the development of periodontal disease.
Technological advances have led to the development of many methods for detecting and quantifying periodontal pathogens, including microbiological culture, enzymatic assays, DNA-DNA hybridization, immunoassays, and polymerase chain reaction (PCR) assays. However, most of these methods are time-consuming and cannot accurately quantify periodontal pathogens [1314]. In recent years, real-time PCR (also known as quantitative PCR [qPCR]) was developed to overcome these limitations, allowing for accurate quantification with higher sensitivity, specificity, simplicity, and rapidity [151617]. Thus, highly sensitive microbiological detection techniques such as real-time PCR can be used to identify and quantify oral bacteria in saliva samples [18]. Umeda et al. used saliva samples from subjects as an alternative way to detect subgingival periodontopathic bacteria because saliva contains periodontal pocket bacteria washed out from the gingival crevicular fluid, and identified the presence of periodontal pathogens in the saliva samples [19]. Saliva sampling is non-invasive, low-cost, and simple; additionally, the samples can be stored, making this method convenient for screening periodontal pathogens [20].
The analysis of oral microorganisms is important for diagnosing periodontitis and predicting disease risk. Thus, studies have been conducted in many countries to analyze oral bacteria in people with periodontal disease and in healthy people. These studies revealed differences in the mean proportions of subgingival species in samples from subjects with periodontitis and healthy subjects in different countries, which may be related to differences in diet, genetics, disease susceptibility, and manifestation [21]. However, no studies have analyzed oral microorganisms in periodontally healthy young Koreans.
The purposes of this study were to determine the prevalence and to quantify the DNA copy numbers of 9 major periodontal pathogens (A. actinomycetemcomitans, P. gingivalis, T. forsythia, T. denticola, Prevotella intermedia, Fusobacterium nucleatum, Campylobacter rectus, Peptostreptococcus anaerobius, and Eikenella corrodens) in saliva samples using real-time PCR assays in periodontally healthy Korean young adults under 35 years of age.
MATERIALS AND METHODS
Study subjects and clinical examination
This study population included 94 periodontally healthy subjects (49 male and 45 female subjects) who were 25–35 years old and visited the Department of Periodontics, Pusan National University Dental Hospital, between August 2016 and March 2017. The periodontal diagnosis of healthy patients followed the guidelines presented by the 1999 International Workshop for a Classification of Periodontal Diseases and Conditions of the American Academy of Periodontology. The exclusion criteria included: 1) any uncontrolled systemic disease that may have affected the patient's periodontal status; 2) periodontal therapy within the previous 6 months; 3) pregnancy or breastfeeding; 4) failure to sign an informed consent form; and 5) fewer than 20 teeth. The subjects received complete information on the purposes and procedures of this study and provided written informed consent. The study protocol was approved by the Institutional Review Board of Pusan National University Dental Hospital (PNUDH-2016-019).
The following clinical parameters were measured at baseline by an experienced periodontist: probing depth, clinical attachment level, plaque index, and gingival index. The clinical attachment level and probing depth were measured using a periodontal probe (PGF-W, Osung, Gwangmyeong, Korea). The plaque index is an indicator of oral hygiene management and was recorded by the O'Leary plaque index. Gingival index values were scored according to the Löe and Silness criteria.
Mouthwash sample collection and DNA isolation
Oral specimens were collected by rinsing the mouth with 12 mL of a solution (E-zen Gargle, JN Pharm, Pyeongtaek, Korea) for 30 seconds. Samples were labeled with the subject's ID and stored at 4°C. For analysis, 8 mL of the gargled solution was transferred to a 15-mL conical tube and then centrifuged at 3,900 rpm for 10 minutes. The supernatant was discarded, and the precipitate was completely resuspended in 200 µL of phosphate-buffered saline. The resuspended sample was transferred to an Eppendorf tube, and DNA was extracted using an DNA extraction kit (Exgene™ Clinic SV, GeneAll Biotechnology, Seoul, Korea) according to the manufacturer's instructions. DNA quality and quantity were evaluated using a spectrophotometer (Nanodrop, Thermo Fisher Scientific, Waltham, MA, USA).
Strains
The following strains were used: A. actinomycetemcomitans (Aa, KCCM 12227), P. gingivalis (Pg, KCTC 5352), T. forsythia (Tf, KCTC 5666), T. denticola (Td, KCTC 15104), P. intermedia (Pi, KCTC 5694), F. nucleatum (Fn, KCTC 2640), P. anaerobius (Pa, KCTC 5182), C. rectus (Cr, KCTC 5636), and E. corrodens (Ec, KCTC 15198). All stains were purchased from the Korean Collection for Type Cultures or Korean Culture Center of Microorganisms. Bacterial DNA was isolated from pure cultures using a DNA Purification Kit (LaboPass Plasmid Miniprep Kit, Cosmogenetech, Seoul, Korea).
Primers and probes for qPCR
Sequences of the primers and probes used for real-time PCR are shown in Table 1. All species-specific primers and probes targeted the variable regions of the 16S ribosomal RNA (rRNA) of the 9 strains. Additionally, the universal bacterial primer pair and probe were used to detect DNA from the total bacteria present in the saliva samples. The fluorescent dyes at the 5′ ends of the probe were FAM, VIC, ABY, and JUN. These dyes were optimized to perform multiplex experiments and used to detect up to 4 targets in a single reaction.
Table 1
Sequence of primers/probes used in real-time PCR

![]()
Standard curve and multiplex real-time PCR
To obtain a standard curve, the 16S rRNA region of each target bacteria was cloned using a PCR cloning vector system (pGEM®-T easy vector system, Promega, Madison, WI, USA). Plasmid DNA sequences were determined using the Sanger sequencing tool. The purified plasmids were quantified with the TaqMan® real-time PCR system. Standard curves were prepared by using serial 10-fold dilutions from 102 to 109 of plasmid DNA. Plasmid standards were run in triplicate, and the mean values were used to calculate the copy numbers of bacteria. For all but 2 strains, qPCR was performed in a total volume of 20 µL using qPCR kits (2× TaqMan Multiplex Master Mix, Applied Biosystems, Foster City, CA, USA), which contained 2 µL of template, 400 nM primers, and 100 nM probe. Except for the T. forsythia and P. intermedia strains, 900 nM primers and 100 nM probe were used. The qPCR conditions for the standard curves were as follows: denaturation at 95°C for 10 minutes, followed by 45 cycles of 95°C for 15 seconds, 50°C for 30 seconds, and 72°C for 30 seconds. A uracil-DNA glycosylase incubation step was performed before PCR cycling to prevent carryover contamination. qPCR was performed using a real-time PCR system (QuantStudio™ 6 Flex Real-Time PCR System, Thermo Fisher Scientific). The proper combination of primers and probes for the multiplex reaction was determined from the cycle threshold (Ct) values. Changes in Ct values between singleplex and multiplex reactions (ΔCt) were calculated and were <0.3. Finally, 3 multiplex reactions were generated per sample: total bacteria, A. actinomycetemcomitans, C. rectus, and E. corrodens in the first reaction; F. nucleatum, P. anaerobius, and P. gingivalis in the second reaction; and P. intermedia, T. forsythia, and T. denticola in the third reaction.
Data representation and statistical analysis
Values of demographic features and clinical parameters are presented as the mean±standard deviation (SD) or a percentage. The bacterial detection frequency in 94 subjects was calculated as a percentage. The DNA copy numbers of the 9 periodontal pathogens were displayed as a bar graph presenting the mean and SD of the detected numbers of 9 pathogens. Statistical analysis was performed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Comparative analysis of the differences among pathogens was performed using 1-way analysis of variance followed by the post hoc Scheffé test. Statistical significance was accepted at a level of P<0.01. The significance of differences between male and female participants in bacterial counts and prevalence was assessed using the t-test and the Pearson's χ2 test, respectively. Statistical significance was accepted at a level of P<0.05.
RESULTS
Demographic characteristics and clinical parameters
A total of 94 subjects were included in this study, including 49 men and 45 women with a mean age of 28.83±2.33 years (range, 20–35 years). Among these subjects, only 4.26% (4 male subjects) were light smokers. At baseline, the periodontal probing depth, clinical attachment level, plaque index, and gingival index were 2.41±0.29 mm, 2.43±0.29 mm, 17.25±13.49, and 0.07±0.13, respectively (Table 2).

Prevalence of the 9 periodontal pathogens in periodontal healthy subjects
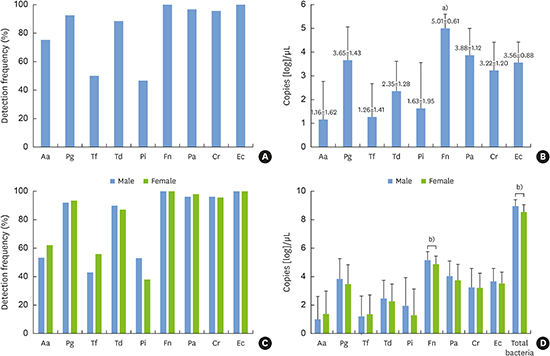
The detection frequency of the periodontal pathogens determined by real-time PCR is shown in Figure 1A. F. nucleatum and E. corrodens were detected in all subjects, while the numbers of positive samples containing the pathogen were 87 (92.6%), 91 (96.8%), and 90 (95.7%) for P. gingivalis, P. anaerobius, and C. rectus, respectively. A. actinomycetemcomitans, T. forsythia, T. denticola, and P. intermedia were present in 54 (75.5%), 46 (50.0%), 83 (88.3%), and 43 (46.8%) samples, respectively, indicating a lower prevalence than the 3 strains mentioned above.
 | Figure 1(A) Prevalence of 9 periodontal pathogens found in 94 periodontally healthy subjects. (B) DNA copy numbers of 9 periodontal pathogens. (C) Bacterial detection frequency in men and women. (D) Comparison of DNA copy numbers of 9 periodontal pathogens between men and women. The data are presented as mean±standard deviation (n=94).Aa: A. actinomycetemcomitans, Cr: C. rectus, Ec: E. corrodens, Fn: F. nucleatum, Pa: P. anaerobius, Pg: P. gingivalis, Pi: P. intermedia, Td: T. denticola, Tf: T. forsythia.
a)Statistically significant difference (P<0.001), b)Statistically significant difference (P<0.05).
|
Quantification of the DNA copy numbers of the 9 periodontal pathogens
The number of the 9 periodontal pathogens present in the saliva samples is shown in Figure 1B. The most abundant periodontal pathogen in the saliva samples was F. nucleatum, which showed a significant difference from all other bacteria (P<0.001), followed by P. anaerobius, P. gingivalis, E. corrodens, C. rectus, and T. denticola. The DNA copy numbers of P. intermedia, T. forsythia, and A. actinomycetemcomitans were significantly lower than those of the bacteria mentioned above (P<0.001).
DISCUSSION
Many studies have shown that periodontal disease progresses through the combined action of related pathogens [25]. These pathogens are also present in the oral cavity of healthy people and can cause disease if the balance among the pathogens is disrupted. Pathologic shifts in the microbiota may occur because of overgrowth of organisms normally present in low numbers, resulting in dysbiosis of the periodontal subgingival microbiota [322]. As the elderly population grows and disease rates increase, studies have been conducted to examine the distribution of periodontal pathogens by age and in periodontally diseased subjects [5182324]. However, few studies have examined the distribution of periodontal pathogens in the oral cavity among periodontally healthy young adults. In this study, we detected the presence of periodontal pathogens and quantified the levels of 9 pathogenic bacteria by real-time PCR using saliva samples from periodontally healthy Korean young adults under 35 years of age.
Because saliva contains periodontal pathogens washed out of the gingival crevicular fluid, saliva samples may useful for detecting bacteria [19]. In previous studies investigating the correlation between bacteria from periodontal pockets and saliva, the authors found no differences between microorganisms in subgingival plaque and saliva samples [2526]. Additionally, real-time PCR is a highly sensitive technique that enables accurate determination of the presence and numbers of pathogens present in saliva samples, despite the limitation that it can only be used for targeting known genes using species-specific primers. Therefore, saliva analysis using real-time PCR may be an effective method for large-scale diagnostic and detection studies to identify periodontal pathogens [20].
Periodontal pathogens are present not only in patients with periodontal disease, but also in apparently healthy subjects. Of the samples obtained from the 94 subjects, 9 major pathogens that cause periodontal disease were detected in most saliva samples. In particular, F. nucleatum was detected not only in the largest number of subjects, but also at the highest levels. F. nucleatum is an important microorganism in the development of dental biofilms; it can adhere to most plaque bacteria and is involved in linking early and late migratory microorganisms [27]. In a previous study, Arenas Rodrigues et al. [28] isolated F. nucleatum from individuals with both healthy periodontal status and periodontal disease, and Zhou et al. [29] found that 58.5% of healthy young adults were positive for this bacterium.
Additionally, red complex bacteria were detected at high frequencies in this study. Red complex bacteria are known to be dominant in the late stages of plaque development, are mainly found in adult cases of periodontitis, and are strongly associated with pocket depth and bleeding on probing [26]. Because P. gingivalis is present at a higher frequency and level in disease-active areas, we expected to detect lower frequencies and levels in our periodontally healthy population. However, P. gingivalis, a key pathogen in periodontal disease, was detected in 92.6% of periodontally healthy Korean young subjects, which agrees with the results of a previous study examining a Swedish population [30]. This finding is inconsistent with the results of other studies that reported that only 25% of the American healthy population and 36.8% of Japanese healthy population were positive for P. gingivalis [3132]. Other red complex bacteria, T. forsythia and T. denticola, were detected at frequencies of 50.0% and 88.3%, respectively, in the present study. In the study of the Swedish population, the prevalence of P. gingivalis, T. forsythia, and T. denticola in healthy subjects was 82%, 82%, and 94%, showing values similar to the prevalence of 95%, 97%, and 93% in periodontal disease patients, respectively [30]. The authors effectively distinguished between periodontitis patients and periodontally intact controls not based on the proportion of single bacterial species, but from a combined microbial colonization/antibody response profile. However, no correlation was found between the strains found (data not shown) in this study.
A. actinomycetemcomitans is responsible for aggressive periodontitis in young adolescents and adults; it was found to be present in the smallest proportion of the 9 pathogens in healthy subjects, although it was detected in as many as 75.5% of subjects. This prevalence is much higher than the rate of 25.9% found by Hyvärinen et al. [33]. Overall, the high prevalence of bacteria in this study compared to that in previous studies may be related to advances in bacterial detection technology [13]. Other factors potentially affecting these results include the genetic background, diet, socioeconomic status, and racial/ethnic or cultural background of the subjects [34]. The previous studies described above evaluated adults from a relatively wide age group, limiting the ability to compare the results with those of the young adults in the present study.
No significant difference was found in the prevalence of each bacterium between men and women. The DNA copy number of total bacteria was significantly higher in men than in women. These results are consistent with a recent study on the effect of sex on periodontal bacteria [35]. Furthermore, the DNA copy number of F. nucleatum was significantly higher in men than in women. These results could be considered meaningful, since severe periodontitis is more prevalent in men than in women.
It has been reported that the number of bacteria in the periodontal disease site, rather than the frequency of periodontal pathogens, is an important factor affecting the development of periodontal disease [36]. In the present study, despite the large number of A. actinomycetemcomitans-positive subjects, the subjects did not suffer from periodontal disease because the number of A. actinomycetemcomitans was not sufficient to cause disease. Consistent with the results of this study, it is generally accepted that potential pathogenic bacteria belong to the commensal oral microflora [37].
In addition to a microbial shift favoring pathogenic species, a suitable environment and ‘susceptible’ host are essential for periodontitis to manifest clinically [1]. Periodontitis is no longer regarded as an infectious disease caused by bacteria. Currently, the paradigm regarding the pathogenesis of periodontitis has shifted to understanding it as an inflammatory disease caused by the host immune system and bacterial complexes [38]. The results of this study confirm the high prevalence of major periodontal pathogens in the saliva of periodontally healthy Korean young adults. Therefore, periodontal disease may develop in periodontally healthy young people because of host susceptibility and an imbalance of pathogens and the host immune system, as periodontal pathogens are also present in periodontally healthy people.
Recent studies have focused on innate immunity in the pathogenesis of periodontitis [39]. The final immune response occurs at the local level and is crucial for regulation of the microbiota by stimulating microenvironmental changes, limiting the increase in periodontal pathogens and helping protective bacteria predominate, or by permitting the establishment of a more pathogenic microbial ecology [40]. Therefore, additional studies are required to examine the oral innate immunity of periodontally healthy people compared to periodontal patients in Koreans.
 XML Download
XML Download