

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intentional replantation refers to a surgical method in which a tooth is intentionally extracted and treated, and then repositioned in the original socket [1]. The indications for intentional replantation include failure of root canal treatment, anatomical limitations, accessibility issues, and complete dislocation by an accident [2]. However, intentional replantation cannot generally be performed for teeth with periodontitis [3] because of the lack of the periodontal ligament (PDL) and the insufficient regenerative ability of the residual PDL. However, in some cases in which it is difficult to use an implant or other prosthetic treatments after tooth extraction or when patients strongly refuse tooth extraction, intentional replantation is sometimes performed as the last treatment option for teeth with periodontitis, and it has been successful in a few cases.
Lu [4] reported that there were no clinical symptoms or functional problems for 32 months after intentional replantation of the mandibular first premolar in patients with periodontitis in whom root canal treatment was problematic. Demiralp et al. [5] reported that the size of the intrabony defects around the teeth had decreased 6 months after the intentional replantation of 15 incisors. However, these studies were case reports or case series, and a study based on a higher level of evidence is required.
The lack of the PDL and the insufficient regenerative ability of the residual PDL after replantation lead to failures in regeneration of the periodontal attachment, resulting in complications such as tooth ankylosis or root resorption. To prevent such complications, various growth factors have been used for periodontal regeneration. Wound healing is regulated by bioactive substances known as growth factors [6]. Growth factors, which are intercellular signaling molecules, promote cell proliferation, angiogenesis, chemotaxis, and differentiation. Platelet-derived growth factor (PDGF) promotes the formation of fibrillar connective tissue in the early stages of wound healing [78]. In addition, PDGF promotes cementogenesis through an increase in the biomineralization of cementoblasts and induction of the formation of Sharpey fibers [910]. Fibroblast growth factor-2 not only accelerates angiogenesis and fibroblast proliferation in wound healing, but also has chemotactic and proliferative effects on PDL cells [1112]. Transforming growth factor (TGF)-β1 plays important roles in the induction of fibroblastic differentiation of PDL cells and PDL precursor cells and maintenance of the PDL under physiological conditions [13]. A previous study showed that growth differentiation factor-5 was effective for periodontal wound healing and regeneration in the musculoskeletal system, including periodontal tissue, because it promoted osteogenesis and ligament formation [14].
Recently, blood-derived fractions have been reported to be a safe and convenient method for applying a high concentration of growth factors to periodontal wounds [1516]. Platelet-rich plasma (PRP) refers to plasma with concentrated platelets from centrifuged blood [17]. The α-granules within platelets contain various growth factors [18]. Representative growth factors within the α-granules include PDGF, insulin-like growth factor, TGF-β, endothelial growth factor, and vascular endothelial growth factor. To take advantage of such growth effects, PRP has been used for sinus lifting [1920], for intrabony defects using guided tissue regeneration [21], for root coverage [22], and to treat peri-implantitis [23], resulting in significantly beneficial outcomes.
The aim of this study was to evaluate the effects of PRP on periodontal healing of replanted root surfaces in dogs histologically and histomorphometrically.
MATERIALS AND METHODS
Experimental animals
The subjects were 6 mongrel dogs (10–15 kg) reared under the same conditions regardless of whether they were male or female, and they had desirable health conditions. The selection and management of the animals, surgical protocol, and preparation steps complied with the rules of the experimental animal room of Chosun University School of Dentistry. This study was approved by the Institutional Animal Care and Use Committee (CIACUC2015-S0008).
Treatments for the experimental animals
Positive control group (n=12)
After tooth extraction, the roots of the positive control group were exposed to air for 5 minutes. Root canal treatment was performed for 5 minutes, followed by soaking in 1.0 mL of sterilized saline solution for 5 minutes (Figure 1A). Each root canal was then filled with calcium hydroxide.

Negative control group (n=12)
After tooth extraction, the cement and PDL were removed from the roots of the negative control group with a curette while holding the crown with dental forceps for 5 minutes. Root canal treatment was performed for 5 minutes, followed by soaking in 1.0 mL of sterilized saline solution for 5 minutes (Figure 1B). The root canal was filled with calcium hydroxide.
Experimental group (n=12)
After tooth extraction, the cement and PDL were removed from the roots of the experimental group with a curette while holding the crown with dental forceps for 5 minutes. Root canal treatment was performed for 5 minutes, followed by soaking in 1.0 mL of PRP for 5 minutes (Figure 1C). The root canal was filled with calcium hydroxide.
Preparation of PRP
Ten milliliters of venous blood was collected from the dogs and centrifuged (MF 300®, Hanil, Incheon, Korea) in a plastic tube without additives at 2,000 rpm for 10 minutes. The centrifuged blood was separated into 3 layers: a top layer of platelet-deficient plasma, a middle layer of PRP, and a bottom layer of red blood cells. Then, 1.0 mL of blood was collected from the platelet-rich middle layer and transferred to an Eppendorf tube in which the roots of the experimental group were soaked.
Surgical procedures
All surgical procedures were performed under general anesthesia, for which acepromazine maleate (Sedaject®, Samu Median, Seoul, Korea; 0.2-0.3 mg/kg, intramuscular [IM]) and tiletamine-zolazepam (Zoletil 50®, Virbac, Carros, France; 7–10 mg/kg, IM) were used as a pre-anesthesia sedative and anesthetic inducer, respectively. Mandibular incisors or mandibular premolar were extracted. Six roots were obtained from each dog. The premolar teeth were divided using a fissure bur before extraction. Each root was dislocated using an elevator and extracted using forceps. Extraction was performed as atraumatically as possible. The 36 dental roots were divided among the 2 control groups and the experimental group.
The crown was removed from all the dental roots in the 3 groups after root surface and root canal treatment and replantation. The buccal flap was then coronally repositioned to cover all the roots, followed by vertical mattress sutures and interrupted sutures (Figure 2).
 | Figure 2The surgical procedure. (A) The crowns and furcation areas of the premolars were sectioned in the middle and parallel to the long axis of the root with a fissure bur. (B) The extractions were performed as atraumatically as possible. (C) The periodontal ligament and cementum were removed by scaling and root planing in the negative control and experimental groups. (D) The roots were soaked in 1.0 mL of platelet-rich plasma in the experimental group. (E) After replanting, the root canals were filled with calcium hydroxide, and the crowns were removed. (F) The roots were covered using a coronally repositioned flap.
|
After the surgical procedures, all the dogs were administered a broad-spectrum antibiotic (spiramycin [Spira-S], Han Dong, Yesan, Korea; 2–20 mg/kg, IM) for 2 weeks from the day of surgery twice daily. Surgical procedures were performed at 8 weeks (8-week groups, n=18) or 4 weeks (4-week groups, n=18) before sacrifice, and the dogs were sacrificed by administering an excessive amount of tiletamine-zolazepam (Zoletil 50®, Virbac; 10–15 mg/kg, IM).
Histological and histomorphometric evaluation
Specimens collected for histological evaluation were fixed in 10% buffered formalin and decalcified with 10% formic acid, followed by embedding in paraffin and sectioning. After hematoxylin-eosin staining, the specimens were observed under a light microscope (Leica DM750, Wetzlar, Hesse, Germany). Of the 12 roots in each group, 4 were sectioned longitudinally parallel to the long axis of the root to observe the histological patterns. The remaining 8 roots were cross-sectioned perpendicular to the long axis of the root for histomorphometric analysis. They were sectioned using a microtome (thickness, 7 μm). Longitudinal sections from the center of the root were used for the histomorphometric analysis.
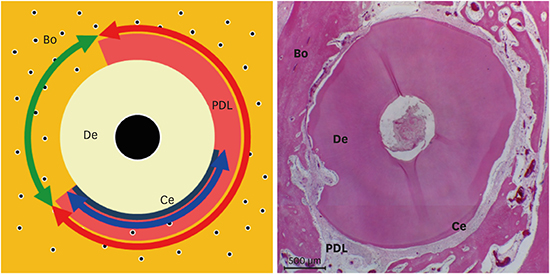
A light microscope (Leica DM750; Wetzlar) equipped with a digital camera (Leica ICC50, Wetzlar) was used to obtain images for all the measurements. The measurements were performed using an analysis program (IMT i-Solution Corporation, Burnaby, British Columbia, Canada) after processing with i-SOLUTION Lite® on a personal computer. Four cross-sections were randomly chosen from each root. The following parameters were measured (Figure 3):
 | Figure 3Schematic illustration representing the horizontal root plane for the histomorphometric analysis. Red, green, and blue arrows shown are periodontal ligament/newly formed periodontal ligament-like tissue, replacement resorption, and cementum/newly formed cementum-like tissue, respectively.Bo: alveolar bone, PDL: periodontal ligament, Ce: cementum, De: dentin.
|
Periodontal ligament/newly formed periodontal ligament-like tissue (PDL/NPDLT): Length of the connective tissue attached to the root surface
Replacement resorption (RR): Length of the part with ankylosis
Cementum/newly formed cementum-like tissue (C/NCeT): Length of the cementum or regenerated cementum on the root surface or the area with cementum-like apposition
PDL/NPDLT and RR were presented as the proportion (%) of the entire circumference of the root, and C/NCeT was presented as the proportion (%) of PDL/NPDLT. The results were calculated as mean±standard deviation.
Statistical analysis
Mean and standard deviation values for each measurement were calculated for each group. To determine if there was statistical significance among the 2 control groups and experimental group, the Kruskal-Wallis test was used. P values <0.05 were considered to indicate statistical significance. Subsequently, 3 sets of pairs were compared using the Mann-Whitney U test with the Bonferroni correction. P values <0.017 were considered to indicate statistical significance for these comparisons. The statistical analysis was conducted using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Clinical outcomes
In the 4-week groups, 1 root in the positive control group and 1 root in the negative control group were exposed without gingivitis at the upper part of the root. In the 8-week groups, 1 root in the positive control group and 1 root in the negative control group were partially exposed, with gingivitis accompanied by edema and rubefaction of the gingiva at the upper part of the root. The other roots in the 4- and 8-week groups healed with healthy gingiva.
Histological outcomes
At 4 weeks
In the positive control group, after 4 weeks of healing, the longitudinal sections of the PDL space showed regular thickness and the cementum became thicker near the root apex. The dentin was covered by the cementum, and no inflammatory response was observed at the cement surface (Figure 4A and D). In the cross-sections, ankylosis was observed on some root surfaces (Figure 5A and D). In the negative control group, periodontal ligament-like tissue and cementum-like tissue were rarely observed on the root surface, whereas ankylosis was found (Figures 4B, 4E, 5B, and 5E). In the experimental group, periodontal ligament-like tissue and cementum-like tissue were observed. However, the thickness of the PDL space was more irregular than in the positive control group, and the cementum-like tissue was found to have irregular thickness along with irregular resorption of dentin on the surface (Figures 4C, 4F, 5C, and 5F).
 | Figure 4Longitudinal sections of periodontal wound healing at 4 weeks after replantation (all samples were stained with hematoxylin and eosin). (A, D) PDL and cementum were observed around the dentin (positive control group). (B, E) Alveolar bone was in direct contact with the dentin (negative control group). (C, F) PDL-like tissue and cementum-like tissue were observed around the dentin (experimental group). However, the width of the PDL-like tissue space and cementum-like tissue was irregular in comparison to the positive control group.PDL: periodontal ligament, Bo: alveolar bone, Ce: cementum, De: dentin, NPDLT: newly formed periodontal ligament-like tissue, NCeT: newly formed cementum-like tissue.
|
 | Figure 5Horizontal sections of periodontal wound healing at 4 weeks after replantation (all samples were stained with hematoxylin and eosin). (A, D) PDL and cementum were observed almost around the dentin (positive control group). However, ankylosis and surface resorption were occasionally observed around the dentin. (B, E) Alveolar bone was in direct contact with the dentin (negative control group). (C, F) The width of the PDL-like tissue space was regular and PDL-like tissue was denser than in the positive control group (experimental group). However, cementum-like tissue was observed around the dentin.PDL: periodontal ligament, Bo: alveolar bone, Ce: cementum, De: dentin, NPDLT: newly formed periodontal ligament-like tissue, NCeT: newly formed cementum-like tissue.
|
At 8 weeks
In the positive control group, at 8 weeks of healing, regular thickness of the PDL space was observed and the cementum became thicker near the root apex. With respect to the cementum-covered dentin, no inflammatory response was observed in the cementum and dentin surface (Figures 6A, 6D, 7A, and 7D). In the negative control group, root resorption and ankylosis were observed in most cases. In addition, deep and broad dentin resorption was observed on the root surface, along with an inflammatory response in the root (Figures 6B, 6E, 7B, and 7E). In the experimental group, periodontal ligament-like tissue and cementum-like tissue were observed, and regular thickness of the cementum-like tissue was observed on the root surface without dentin resorption (Figures 6C, 6F, 7C, and 7F).
 | Figure 6Longitudinal sections of periodontal wound healing at 8 weeks after replantation (all samples were stained with hematoxylin and eosin). (A, D) PDL and cementum were observed around the dentin (positive control group). (B, E) Alveolar bone was in direct contact with the dentin (negative control group). Wide and deep inflammatory resorption was observed on the dentin surface. (C, F) PDL-like tissue and cementum-like tissue were observed around the dentin (experimental group). The cementum-like tissue was thinner than the cementum of the positive control group. However, the thickness of the cementum-like tissue was uniform, as in the positive control group.PDL: periodontal ligament, Bo: alveolar bone, PDL: periodontal ligament, Ce: cementum, De: dentin, NPDLT: newly formed periodontal ligament-like tissue, NCeT: newly formed cementum-like tissue.
|
 | Figure 7Horizontal sections of periodontal wound healing at 8 weeks after replantation (all samples were stained with hematoxylin and eosin). (A, D) PDL and cementum were observed around the dentin (positive control group). (B, E) Alveolar bone was in direct contact with the dentin (negative control group). (C, F) PDL-like tissue and cementum-like tissue were observed around the dentin (experimental group). Cementum-like tissue had formed in the area of surface resorption.PDL: periodontal ligament, Bo: alveolar bone, Ce: cementum, De: dentin, NPDLT: newly formed periodontal ligament-like tissue, NCeT: newly formed cementum-like tissue.
|
Histomorphometric outcomes
In the 4th week, the experimental group showed a lower ankylosis rate than the positive control group (P=0.020) and the negative control group (P=0.020). The experimental group showed a higher rate of formation of cementum-like tissue than the positive control group (P=0.018) and negative control group (P=0.034). Although there was a significant difference in the rate of ankylosis and formation of cementum-like tissue among the 3 groups (P<0.05), no statistical significance was observed between any pair of groups (P>0.017) (Table 1).
Table 1
Histomorphometric results of periodontal wound healing at 4 weeks after replantation

Values are presented as mean±standard deviation.
PDL/NPDLT: periodontal ligament/newly formed periodontal ligament-like tissue, RR: replacement resorption (ankylosis), C/NCeT: cementum/newly formed cementum-like tissue, Pos.: positive control roots, Neg.: negative control roots, PRP: platelet-rich plasma.
a)Statistically significant difference (P<0.05) (Kruskal-Wallis test).
![]()
In the 8th week, the experimental group displayed a lower ankylosis rate than the positive control group (P=0.564) and negative control group (P=0.021). The experimental group showed a higher rate of formation of cementum-like tissue than the positive control group (P=0.561) and the negative control group (P=0.271). Although there was a significant difference in the rate of ankylosis and formation of cementum-like tissue among the 3 groups (P<0.05), no statistical significance was observed between any pair of groups (P>0.017) (Table 2).
Table 2
Histomorphometric results of periodontal wound healing at 8 weeks after replantation

Values are presented as mean±standard deviation.
PDL/NPDLT: periodontal ligament/newly formed periodontal ligament-like tissue, RR: replacement resorption (ankylosis), C/NCeT: cementum/newly formed cementum-like tissue, Pos.: positive control roots, Neg.: negative control roots, PRP: platelet-rich plasma.
a)Statistically significant difference (P<0.05) (Kruskal-Wallis test).
![]()
DISCUSSION
Periodontal regeneration, which refers to regeneration of the alveolar bone, PDL, and cementum to create a new attachment to the root surface, is the ultimate goal of periodontal defect treatment [24]. The regeneration process of these 3 different tissues is complicated and requires various growth factors, so in some studies, 2 or more growth factors have been applied to promote periodontal regeneration [2526].
PRP is an extract from blood that contains various growth factors. It can be obtained by centrifugation after adding anticoagulant to blood, and is then coagulated with thrombin for use in clinical applications. Thrombin is a substance that converts water-soluble fibrinogen to insoluble fibrin to form a fibrin network, which promotes coagulation. Chan et al. [27] reported that thrombin activated cell growth and cell clustering of PDL fibroblasts, thereby preventing tooth ankylosis and promoting periodontal regeneration. Reichert da Silva Assunção et al. [28] compared the effects of platelet-poor plasma (PPP); calcium chloride-activated PRP (PRP/Ca); calcium chloride- and thrombin-activated PRP (PRP/Thr/Ca); and bone marrow mononuclear cells and PRP/Ca (BMMCs/PRP/Ca) on periodontal regeneration. As a result, only the group with thrombin showed no tooth ankylosis. However, because of the limited amount of thrombin in blood extract, thrombin extracted from cows is commercially available. PRP produced by the conventional method has additional costs due to the addition of anticoagulant and thrombin and has a risk of foreign body reaction. However, the PRP used in this study was centrifuged without additional additives. Furthermore, similarly to other studies, the experimental group showed a lower tooth ankylosis rate than the negative and positive control groups.
Recently, studies have investigated periodontal regeneration using stem cells collected from bone marrow or PDL. PDL stem cells (PDLSC) can be obtained when the third molar is extracted or teeth are extracted for orthodontic treatment. However, the amount is limited and an in vitro culture process is required for clinical use. Reichert da Silva Assunção et al. [28] demonstrated that a group treated with mesenchymal stem cells, instead of thrombin, showed a significantly higher tooth ankylosis rate. Zhao et al. [29] demonstrated that a group treated with both PDLSC and platelet-rich fibrin (PDLSC/PRF) and a group treated with PRF alone showed significantly lower tooth ankylosis rates than the control group after dental replantation. Although the PDLSC/PRF group had a lower tooth ankylosis rate than the PRF group, no significant difference was observed. The results of this study show that PRP alone can promote the regeneration of periodontal tissue in dental replantation.
In the studies of Reichert da Silva Assunção et al. [28] and Zhao et al. [29], replantation was performed without removal of the cementum and PDLs of the teeth, and the blood extract was applied directly to the original socket. In this study, unlike the other studies, the cementum and PDLs of the teeth were removed, and replantation was performed after PRP was applied for 5 minutes to the root surface without curettage of the socket. As a result, we observed a lower tooth ankylosis rate in the experimental group, similarly to other studies. Previous studies have reported that living cells on the root surface played an important role in periodontal regeneration [303132]. This study demonstrated that even if there are no living cells on the root surface, periodontal regeneration is possible even with only PRP and PDL cells present on the adjacent socket.
In this study, the tooth ankylosis rates in the 4-week positive control group and the negative control group were 61.83%±16.89% and 78.34%±19.55%, respectively, which were higher than in the experimental group. This suggests that the damage during in vitro retention after extraction may affect the PDL cells and cement cells that are present on the initial root surface. The tooth ankylosis rates in the experimental group were 7.88%±10.49% and 13.98%±14.38% at 4 and 8 weeks, respectively, which were lower than in all control groups. This suggests that PRP can improve the regeneration of damaged PDL and cementum by influencing the initial healing process. However, since the number of samples that underwent histomorphometric analysis was too small to confirm statistical significance, further studies on a larger number of specimens are needed.
In summary, this study showed that applying PRP to root surfaces during tooth replantation in dogs could reduce tooth ankylosis and increase periodontal ligament-like and cementum-like tissue formation. This suggests that PRP can improve periodontal regeneration and that PRP may be a treatment option in tooth replantation.
 XML Download
XML Download