

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontitis is a chronic inflammatory disease of the supporting tissues surrounding the teeth that results in destruction of the periodontal ligament, cementum, connective tissue, and alveolar bone [1]. Chronic periodontitis, which is the most common form of this condition and the main cause of tooth loss in adults, affects around 15% to 20% of Asians [2], while severe periodontitis affects approximately 5% to 15% of adults worldwide [3]. Periodontitis results from an ecological imbalance within the microbial community of the dental biofilm that promotes the growth of pathogenic bacteria [4].
Among the various bacterial species that are associated with the development of periodontitis, Porphyromonas gingivalis (P. gingivalis), a Gram-negative anaerobe, is implicated as a keystone pathogen in the etiology of chronic periodontitis [5]. P. gingivalis possesses an arsenal of specialized virulence factors that contribute to its pathogenicity, including lipopolysaccharide, hemolysin, fimbriae, hemagglutinin, and the Arg-X-(Rgp) and Lys-X-specific (Kgp) cysteine proteinases (gingipains) [6]. P. gingivalis can invade periodontal tissues and is able to evade host defense mechanisms. In doing so, it causes dysregulation of the host immune and inflammatory responses [7]. Therefore, therapeutic strategies targeting P. gingivalis may be useful to prevent its colonization in the subgingival area.
Nonsurgical periodontal treatment through scaling and root planing (SRP) remains the gold standard for managing chronic periodontitis, and allows the periodontal pockets to be sufficiently cleaned. However, in moderate and severe cases of chronic periodontitis, because of the deep periodontal pockets and the involvement of complicated anatomical features such as furcations, bacteria may be inaccessible to mechanical instruments. Therefore, antibiotics and various antimicrobial agents such as chlorhexidine mouthwash have been recommended as adjuncts to SRP. However, despite their reported clinical benefits, the emergence of antimicrobial resistance, which is currently posing a major global challenge, and the potential side effects of antibiotics have led to a reduction in the application of antibacterial therapy [89]. In addition, the use of chlorhexidine is associated with adverse effects such as hypersensitivity, tooth discoloration, and toxicity, and consequently is not recommended for long-term use [10].
Given those limitations, alternative therapies for biofilm control targeting bacterial strains such as P. gingivalis are urgently needed for the treatment of periodontal diseases. The use of specific egg yolk immunoglobulin (IgY) as a novel mode of immunotherapy to confer passive immunity has received increasing interest as a cost-effective and safe alternative to antibiotics in the management of periodontitis. The concept of passive immunity was first described in 1893 by Klemperer [11], who demonstrated that avian maternal antibodies are transferred from serum to egg yolk to protect the developing embryo from pathogens. Since 1996, the production and use of IgY (i.e., IgY technology) has become a globally accepted practice [12].
Previous in vitro studies have demonstrated that antigen-specific IgY was capable of inhibiting bacterial growth and adhesion [1314]. In addition, an in vivo study reported that periodontal disease progression was prevented in mice by specific IgY treatment through a decrease in the amount of alveolar bone loss [13]. Although numerous clinical studies have been conducted with antigen-specific IgY in humans to evaluate its efficacy in treating various diseases [151617], from a periodontal perspective, limited clinical research has been performed on the effectiveness of specific IgY against periodontal disease-causing P. gingivalis in the management of chronic periodontitis.
The aim of the present study was to evaluate the clinical and microbiological effects of egg yolk immunoglobulin against P. gingivalis (anti-P.g. IgY) in the form of subgingival irrigation and mouthwash as an adjunct to SRP in patients with moderate to severe chronic periodontitis.
Go to : 
MATERIALS AND METHODS
Subjects
The subjects were recruited from patients receiving care at the outpatient clinic of the Department of Periodontology, Stomatologic Hospital and College, Anhui Medical University, Hefei, China. Subject recruitment started in October 2015 and was completed in October 2016. Sixty patients, aged 18–65 years, with a mean age of 43.26 years, were included in this study. All 60 patients completed the study. The patients were diagnosed with moderate to severe chronic periodontitis, as determined using the case definition proposed by Armitage [18]. The following patients were included in the study: 1) male or female patients aged 18–65 years old, with 2) no systemic diseases, 3) no history of smoking, and 4) a minimum of 20 natural teeth. The exclusion criteria were; 1) the use of systemic or local antimicrobials and/or anti-inflammatory medication or steroids in the past 3 months, 2) surgical or non-surgical periodontal treatment in the previous 6 months, 3) being pregnant or lactating, 4) having orthodontic devices or removable appliances, and 5) having a history of sensitivity to any drugs, egg, or mouthwashes. The study received approval from the Biomedical Ethics Committee of Anhui Medical University (registration No. 20150265). The study was conducted in accordance with the ethical standards established in the 1964 Declaration of Helsinki [19] and good clinical practice. Written informed consent was obtained from all patients prior to the commencement of the study.
Sample size calculation
The mean clinical attachment level (CAL) was used to calculate the sample size. Assuming a mean difference of 1.2 mm in the CAL change from baseline between the 2 groups (anti-P.g. IgY and placebo), with equal variance of 1.2 mm, with a 2-sided type I error rate of 0.05, and 80% power, using the PASS software version 14.0 (NCSS, LLC., Kaysville, UT, USA), the sample size calculation service was provided by FMD K&L Ltd. (Fort Washington, PA, USA), and the number of patients needed for each treatment group was determined to be 16. Anticipating a drop-out rate of 20%, the study needed 40 patients (20 per group). A standard treatment group of chlorhexidine including 20 patients was also added, leading to a total sample size of 60 (20 patients in each group).
Study design and treatment
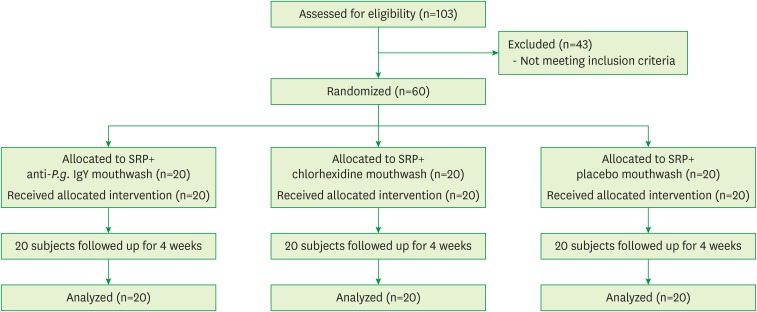
This study was designed as a randomized, double-blind, placebo-controlled parallel-design study. A flow diagram of the study progress is presented in Figure 1. The 60 patients were randomly assigned to 3 groups, each consisting of 20 participants, using a computer-generated randomization table. Group 1 (the test group) received anti-P.g. IgY mouthwash, group 2 (the positive control group) received 0.2% chlorhexidine mouthwash, and group 3 (the negative control group) received placebo mouthwash. A clinical examination and sample collection for microbiological analyses were performed at baseline in each subject. Subsequently, oral hygiene instructions were given, and full-mouth SRP was performed by 2 examiners, followed by full-mouth subgingival irrigation with the allocated mouthwash. Rinsing with mouthwash was initiated the day after the baseline visit (day 1 of the study) and ended on the 28th day. All patients were instructed to rinse with 15 mL of the allocated mouthwash 3 times a day for 1 minute, and not to drink anything or rinse their mouth with water for an hour. All participants were seen again at 7, 14, and 21 days after the baseline visit and underwent full-mouth subgingival irrigation with their allocated mouthwash. Oral hygiene instructions were re-emphasized. At 4 weeks (the end of the study), a clinical examination and sample collection for microbiological analyses were performed again.
The anti-P.g. IgY mouthwash was manufactured by Anhui Province Bioengineering Co. Ltd., Hefei, China. The product trade name is Anshujing, and had an antibody titer of 1:1,280. The composition of the mouthwash was as follows: purified anti-P.g. IgY, sterile water, glycerin, sorbitol, citric acid, and sodium citrate. Commercially-obtained 0.2% chlorhexidine mouthwash was used as a positive control. The placebo mouthwash contained sterile water, glycerin, sorbitol, citric acid, and sodium citrate. All the mouthwashes were put in white, opaque bottles, coded A, B, or C by an independent person. Neither the examiners nor subjects in the study knew which solutions were test or controls until end of the trial. No adverse effects were reported or observed in any of the groups.
Clinical measurements
Clinical measurements were performed in each subject at baseline and at 4 weeks by 2-blinded examiners. Full-mouth periodontal probing was performed at 6 sites of each tooth (disto-buccal, mid-buccal, mesio-buccal, disto-lingual, mid-lingual, and mesio-lingual) using a standardized pressure-sensitive probe (Florida Probe, Gainesville, FL, USA). The clinical parameters recorded were probing pocket depth (PPD), CAL, bleeding on probing (BOP), and the plaque index (PI) [20].
Microbiological examination
Sample collection
Subgingival plaque, saliva, and gingival crevicular fluid (GCF) samples were collected at day 0 (baseline) and at 4 weeks. The samples were pooled into an Eppendorf tube with sterile phosphate-buffered saline and stored at −80°C before analysis. To avoid bias, a different blinded investigator performed the microbiological analysis.
·Subgingival plaque collection: In each patient, the site with the deepest probing depth (PD) that bled on probing was selected. The site was then isolated with cotton rolls and air-dried, and supragingival plaque was removed with a curette to ensure that it was not contaminated when taking the samples. The subgingival plaque samples were collected with 2 #35 paper points.
·GCF sampling: Subjects thoroughly rinsed with sterile saline for 1 minute. GCF was collected from the deepest site. The selected site was isolated with cotton rolls and supragingival plaque was removed. The crevicular site was dried gently with an air syringe. A sterile dry filter paper (3M Whatman, 2×1 mm, Sigma-Aldrich, St. Louis, MO, USA) was gently inserted into the periodontal pocket until mild resistance was encountered and left in place for 1 minute. Care was taken to avoid mechanical injury. Strips contaminated with blood were discarded.
·Saliva sampling: Subjects thoroughly rinsed with sterile saline for 1 minute. Approximately 0.5–1 mL of unstimulated whole saliva was collected in a sterile Eppendorf tube, and vigorously shaken with a vortex mixer for 10–20 seconds to disperse the bacteria.
N-Benzoyl-DL-arginine-naphthylamide (BANA) test
The BANA test was used to determine changes in numbers of red complex bacteria (RCB). A stock solution of BANA was prepared by dissolving 44 mg of BANA (Sigma-Aldrich) in 1 mL of dimethyl sulfoxide and stored at 4°C. Before use, the BANA stock solution was diluted with a 1:100 by volume mixture of 15 mmol/L Tris-buffered saline at pH 8.5. The subgingival plaque, GCF, and saliva samples were removed from the freezer and thawed at room temperature for 30 seconds. Then, 100 μL of 1 mmol/L buffered BANA solution and 100 μL of test samples were added to the microplate well and allowed to incubate overnight at 37°C.The following day, 50 µL of 2.5 g/L Fast Black K was added to the microtiter plate well. Five minutes after observing the color change, readings were measured at 600 nm using a microplate reader. The BANA test results were assessed using numerical values, with A600>0.2 indicating a positive test result. Saline was used as a control.
DNA extraction and quantification of bacteria by real-time polymerase chain reaction (PCR)
Subgingival plaque samples were thawed at room temperature and centrifuged for 5 minutes at 12,000 rpm. Bacterial DNA was extracted using a TIANamp Bacteria DNA Kit according to the manufacturer's protocol. The extracted DNA was stored at −20°C before bacterial detection by real-time quantitative PCR.
P. gingivalis, Tannerella forsythia (T. forsythia), Treponema denticola (T. denticola), and universal plasmid DNA were synthesized by Shanghai Sangon Biotech Co. Ltd. (Shanghai, China). The remaining PCR products were sequenced by Shanghai Sangon Biotech Co. Ltd. after agarose gel electrophoresis. The PCR fragments derived from P. gingivalis and T. forsythia had 100% homology with P. gingivalis and T. forsythia gene sequences in the gene pool. The PCR fragment derived from T. denticola had 98.4% homology with the T. denticola gene sequence in the gene pool (an A base in GenBank was replaced by G, and a T base was replaced by C). The PCR fragment derived from the universal plasmid DNA had 98.1% homology with the universal gene sequence in the gene pool (GenBank; 2 G bases were substituted by A, and a C base was replaced by G), which showed that the plasmid synthesized in this experiment was consistent with the National Center for Biotechnology Information database. The plasmid standards were serially diluted from 1010 to 104 DNA copies, and amplified using the protocol described below. A standard curve was generated as a plot between the cycle number at the crossing point and the initial plasmid DNA copies. Using the standard curve, the absolute quantity of each target species was calculated as DNA copies per reaction.
The primers and probes applied in real-time PCR were synthesized by Shanghai Sangon Biotech Co. Ltd. (Table 1). Thermal cycling was performed in a PCR T100TM Thermal Cycler (BioRad, Hercules, CA, USA). According to the Premix Ex TaqTM instructions (Probe qPCR, Takara, Otsu, Japan), the following reaction system was established: 10.0 μL of Premix Ex Taq (Probe qPCR), 0.4 μL of each specific forward and reverse primer, 0.8 μL of Taqman Probe, 0.2 μL of ROX Reference Dye II, 2.0 μL of DNA template, with diethyl pyrocarbonate added to a volume of 20 μL. The quantitative PCR protocol included the following steps: initial denaturation at 95°C for 30 seconds, followed by 45 cycles of denaturation at 95°C for 5 seconds, annealing for 30 seconds (see Table 1 for the annealing temperatures), and a final extension at 72°C for 30 seconds.
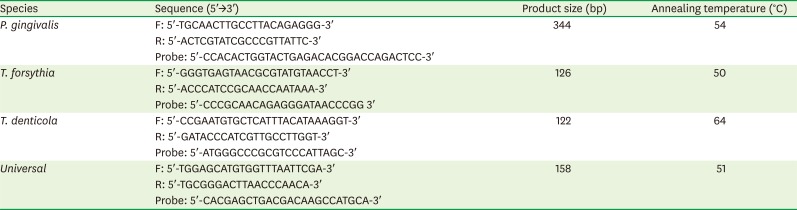
Table 1
Sequence of real-time PCR primers and probes, annealing temperatures, and expected product size
PCR: polymerase chain reaction, P. gingivalis: Porphyromonas gingivalis, T. forsythia: Tannerella forsythia, T. denticola: Treponema denticola.
![]()
Statistical analysis
The primary endpoints of this study were PD reduction, change in CAL, and changes in the proportions of P. gingivalis from baseline to the end of the study. The secondary outcomes included changes in 1) the PI, 2) the BOP 3), the numbers of RCB, and 4) the proportions of T. denticola and T. forsythia from baseline to end of the study. The significance of differences in clinical parameters and the number of RCB within the groups was evaluated using the paired t-test. Analysis of variance was used to analyze intergroup changes. The significance of within-group changes in the levels of P. gingivalis, T. denticola, and T. forsythia was evaluated with the Wilcoxon signed-rank test. The Kruskal-Wallis H test was used to evaluate differences between the groups. For multiple comparisons, the Mann-Whitney U test was used. A statistically significant difference was established at P<0.05. Statistical analyses were performed using SPSS version 16 (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
Clinical findings
Table 2 presents the mean changes in CAL, PPD, and percentage changes in BOP and PI between baseline and 4 weeks. In all groups, at 4 weeks, there was a significant gain in CAL and the PPD had significantly decreased compared to baseline (P<0.05). Multiple comparisons revealed that the difference in clinical attachment gain between the anti-P.g. IgY group and the chlorhexidine group was statistically significant (P<0.05), as was the difference between the anti-P.g. IgY and the placebo (P<0.01). The reduction in PPD was statistically significant within all the groups. BOP scores decreased in the anti-P.g. IgY and chlorhexidine groups, and the difference was statistically significant (P<0.05). A significant reduction in the PI took place within each group at 4 weeks compared to baseline (P<0.05). An intergroup analysis of all clinical parameters did not reveal any statistically significant differences.

Table 2
Comparison of clinical parameters at the baseline and 4-week examinations
Values are expressed as mean±SD or percentage±SD.
anti-P.g. IgY: egg yolk immunoglobulin against Porphyromonas gingivalis, CAL: clinical attachment level, BOP: bleeding on probing, PI: plaque index, PPD: probing pocket depth, SD: standard deviation.
a)Statistically significant intragroup difference compared to baseline; b)Statistically significant compared to chlorhexidine (P=0.025) and placebo (P=0.001), respectively.
![]()
Microbiological findings
Real-time PCR findings
Table 3 presents the changes in the median counts of P. gingivalis, T. forsythia, and T. denticola in the total bacterial load before and after treatment. Figure 2 shows the changes in the percentages of each periodontopathic bacterium in the total bacteria. The change in the proportion of P. gingivalis from baseline to 4 weeks was the primary end point. All agents decreased the proportion of P. gingivalis at 4 weeks compared to baseline to a statistically significant extent (P<0.05) (Table 3 and Figure 2A), but there were no statistically significant differences between the 3 groups. The proportion of T. forsythia in the total bacteria decreased in all 3 groups after treatment, and the difference was statistically significant (P<0.05) (Table 3 and Figure 2B). As with P. gingivalis, there were no statistically significant differences between the 3 groups. The proportion of T. denticola in the total bacteria decreased in all 3 groups after treatment, but the difference was statistically significant only in the chlorhexidine group (P<0.05) (Table 3 and Figure 2C). In addition, the differences between the 3 groups were not statistically significant.

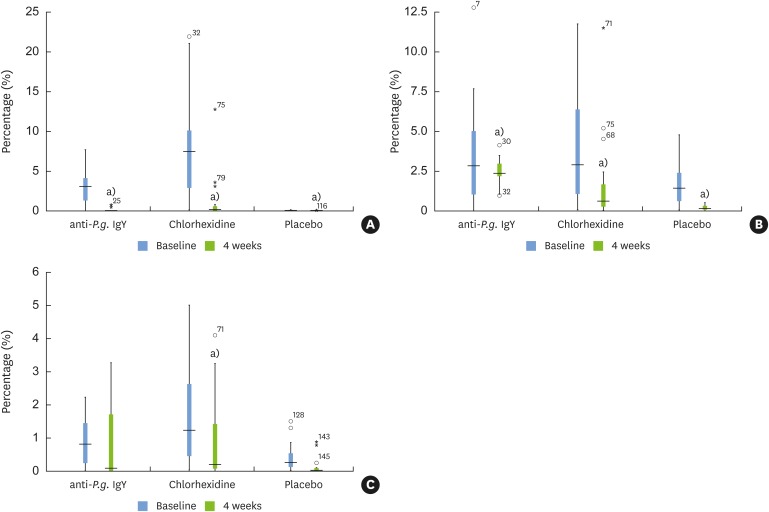 | Figure 2Box blots showing the percentages of each periodontopathic bacterium in the total bacteria at baseline and 4 weeks. (A) Porphyromonas gingivalis. (B) Tannerella forsythia. (C) Treponema denticola.
Anti-P.g. IgY: egg yolk immunoglobulin against Porphyromonas gingivalis.
a)Statistically significant intragroup difference compared to baseline (Wilcoxon signed-rank test).
|
Table 3
Comparison of the proportion of each periodontopathic bacterium in the total bacteria at baseline and 4 weeks
Values are expressed as the median changes in total bacterial counts and the upper and lower interquartile ranges (in parentheses).
Anti-P.g. IgY: egg yolk immunoglobulin against Porphyromonas gingivalis, P. gingivalis: Porphyromonas gingivalis, T. forsythia: Tannerella forsythia, T. denticola: Treponema denticola.
a)Statistically significant intragroup difference compared to baseline.
![]()
BANA test findings
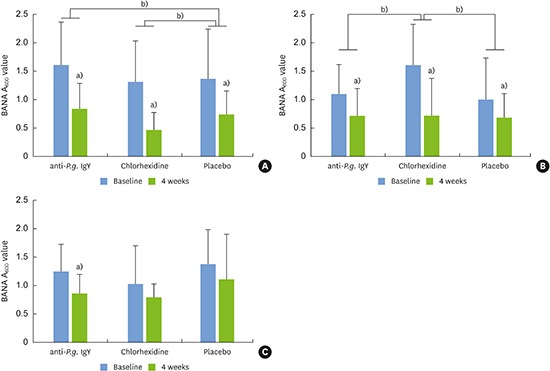
Figure 3A-C shows the changes in the number of RCB in the subgingival plaque, GCF, and saliva, respectively. The number of RCB in the subgingival plaque in all the experimental groups significantly decreased at 4 weeks when compared to baseline (P<0.001), but an intergroup analysis did not reveal any statistical significance. The RCB numbers in the GCF significantly decreased at 4 weeks in the anti-P.g. IgY and chlorhexidine groups (P<0.001), and in the placebo group (P<0.05). The reduction in RCB in the saliva was statistically significant only in the anti-P.g. IgY group at 4 weeks (P<0.01). For multiple comparisons, because the groups had different baseline values, we compared the difference between the baseline and 4-week values of each group to the corresponding values from different groups (i.e., the group 1 baseline values – group 1 values at 4 weeks were compared to the group 2 baseline values – group 2 values at 4 weeks, and so on). The difference in the decrease of RCB in the subgingival plaque between the anti-P.g. IgY and placebo groups was statistically significant (P<0.05), as was the difference between the chlorhexidine and placebo groups (P<0.001). However, the difference between anti-P.g. IgY and placebo regarding the change in the number of RCB in the subgingival fluid was not statistically significant. In addition, although only the anti-P.g. IgY group showed a statistically significant difference in the reduction of RCB in saliva, when compared to placebo, there was no statistical significance.
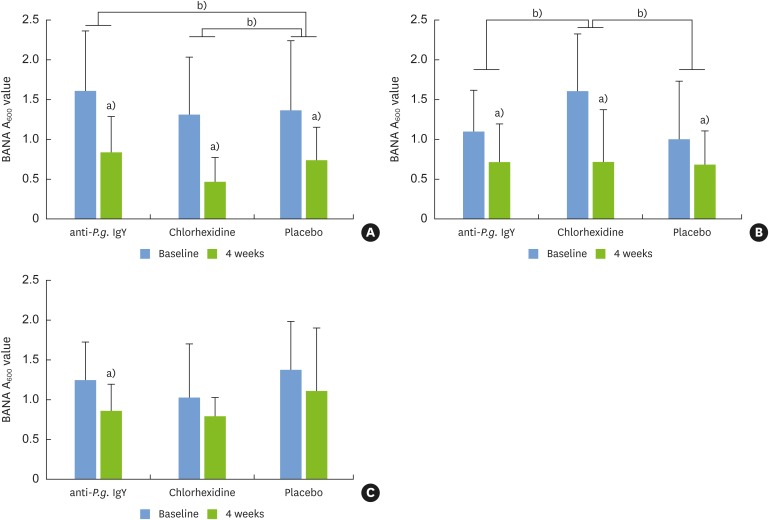 | Figure 3Comparison in the number of RCB at baseline and 4 weeks in (A) subgingival plaque, (B) gingival crevicular fluid, and (C) saliva.
RCB: red complex bacteria, anti-P.g. IgY: egg yolk immunoglobulin against Porphyromonas gingivalis, BANA: N-Benzoyl-DL-arginine-naphthylamide.
a)Statistically significant intragroup difference compared to baseline; b)Statistically significant difference between the different treatment groups.
|
Go to :
DISCUSSION
Periodontitis is one of the most prevalent oral polymicrobial infectious diseases, and there is a dire need for new, effective, safe, and financially viable therapeutic strategies to combat this disease. Over the last years, considerable interest has emerged in natural products with potential therapeutic uses in dentistry. Passive immunotherapy with egg yolk-derived IgY has been investigated in animal and human studies designed to explore new methods for periodontal disease treatment as an alternative to synthetic antimicrobials, based on its advantages, such as cost-effectiveness, biosafety, and the ability for large amounts of antibody preparations to be prepared without killing animals [21]. In the present study, passive immunization using egg yolk antibody against whole-cell P. gingivalis (anti-P.g. IgY) was used as an adjunct to SRP.
The present study aimed to test the clinical and microbiological effects of anti-P.g. IgY in the form of mouthwash and subgingival irrigation when used as an adjunct to SRP in patients with moderate to severe chronic periodontitis. To our knowledge, this is the first clinical study to test the effects of egg yolk antibody against whole-cell P. gingivalis on various parameters of periodontal disease.
In the present study, the adjunctive use of anti-P.g. IgY with SRP resulted in a significant decrease in PD and an increase in CAL. Our results are in line with those of Sugano [22] and Yokoyama et al. [23], who reported a significant reduction in PD when using anti-P. gingivalis gingipains (IGY-GP) lozenges and subgingival gel, respectively, as adjuncts to SRP. However, because in the present study we used a mouthwash with antibodies against whole-cell P. gingivalis, a direct comparison to those studies cannot be made. When compared to chlorhexidine and placebo, the test group showed a significantly greater gain in CAL. These positive therapeutic results could have been because of SRP [2425], with the results enhanced by anti-P.g. IgY. The shift in the composition of the subgingival microflora may have enabled the neutralization of enzymes that contribute to the pathogenic potential of P. gingivalis [26], thereby leading to periodontal tissue regeneration. A previous in vitro study on passive immunization evaluating the effectiveness of IgY against whole-cell F. nucleatum showed that specific IgY effectively inhibited biofilm formation. This was attributed to the high binding ability of specific IgY to cell surface components, which could prevent bacterial growth and adhesion [13].
In the present study, the adjunctive use of anti-P.g. IgY resulted in significant improvement in BOP and the PI. There was no difference between chlorhexidine and anti-P.g. IgY in terms of BOP and the PI. These results show that the effect of SRP as a standard means of controlling inflammation seemed to be enhanced by the adjunctive use of anti-P.g. IgY, suggesting that anti-P.g. IgY mouthwash played an effective role as an adjunct to SRP.
In the present study, subgingival levels of P. gingivalis significantly decreased in all groups. However, an intergroup comparison did not show any statistical significance. Moreover, no additional benefits were observed in the test group when compared to placebo regarding the reduction in the levels of P. gingivalis. Our results contrast to those of Yokoyama et al. [23], who reported a significant decrease in levels of P. gingivalis in the test group and an increase in the control group at 4 weeks after treatment with IGY-GP. However, the differences in the sample size, study design, and type of antibodies used (i.e., antibodies against P. gingivalis gingipains in that study versus whole-cell antigen of P. gingivalis in the present study) make direct comparisons rather difficult.
Nevertheless, 2 potential reasons may account for the lack of additional effects in our study. The first is related to the form and route of anti-P.g. IgY delivery. The limited penetration abilities of mouthwash and rapid clearance of the subgingivally delivered anti-P.g. IgY solution by GCF [27] may explain the lack of additional benefits in the test group regarding changes in the levels of P. gingivalis. The short duration of our study (4 weeks) may be the second reason. Studies with 3, 6, and 9 months of follow-up reported significant reductions in periodontal pathogens and lasting suppressive effects following SRP in patients with adult periodontitis [2829]. Therefore, a longer study might have yielded better findings in the test group. Thus, the form and route of anti-P.g. IgY delivery and the short duration of 4 weeks are limitations of this study. Nonetheless, the reduction in the levels of P. gingivalis observed in our study may have resulted from disruption of the subgingival microbial biofilm by SRP. The predominantly non-pathogenic early colonizers may have occupied the vacant habitat faster, resulting in reduced levels of P. gingivalis [28293031].
In the present study, we evaluated changes in numbers of RCB through the BANA test. Microorganisms in the subgingival environment do not exist in isolation, but rather as members of communities. A consortium of bacterial species designated as RCB, comprising P. gingivalis, T. forsythia, and T. denticola, has been found to have the closest association with periodontal disease severity, as measured by PD and BOP [32]. As a keystone pathogen, P. gingivalis engages in 2-way communication with accessory pathogens to disintegrate host immune surveillance and to elevate the pathogenicity of the entire microbial community [33]. In our study, anti-P.g. IgY significantly reduced the numbers of RCB in subgingival plaque, GCF, and saliva. When compared to placebo, anti-P.g. IgY showed a significantly greater reduction in RCB numbers in subgingival plaque. The reduction in RCB in our study may have resulted from SRP [2829], with additional benefits observed because anti-P.g. IgY reduced the microbial load. This could suggest that anti-P.g. IgY effectively controlled the periodontal microorganisms.
As in other human clinical trials, our clinical results may have been influenced by the Hawthorne effect, which is a positive change in the behavior of human subjects in an experiment due to their awareness of being observed [34]. The Hawthorne effect applied equally to all the experimental groups, but it should not have affected the differences between groups. In randomized controlled trials, the occurrence of adverse effects is one of the most important findings. No adverse reactions were reported among any of the subjects in the present study.
Passive immunization using egg yolk IgY is a promising development in the search for safe and cost-effective antimicrobials for periodontal therapy. Within the limitations of this study, we conclude that anti-P.g. IgY showed similar effects to chlorhexidine in the treatment of chronic periodontitis, by improving clinical indices and microbiological parameters regarding RCB. However, the use of anti-P.g. IgY provided no additional benefit over placebo regarding changes in the level of P. gingivalis. Nevertheless, the results of this study favor the promotion of anti-P.g. IgY mouthwash as an alternative to chlorhexidine in improving clinical parameters, as it is non-toxic and causes no undesirable side effects [35], making it suitable for long-term use in periodontitis patients, children, pregnant women, and the elderly. However, further studies in other populations, with longer follow-up, a larger sample size, and a more controlled or sustained subgingival delivery system are required to extend our findings.
Go to :
 XML Download
XML Download