

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For decades, the innumerable teeth extracted due to periodontitis have been replaced with dental implants. Unfortunately, however, dental implants are vulnerable to peri-implantitis if plaque control is inadequate [1]. Several studies have shown associations between systemic disease and periodontitis [234]. Therefore, the role of proper plaque biofilm control in the prevention of systemic disease and periodontitis has received a greater emphasis than ever before.
Periodontitis is a chronic disease caused by intraoral biofilms harboring periodontal pathogenic microorganisms [56]. Peri-implantitis is a multifactorial disease with an etiology similar to that of periodontitis [7]. Gingivitis is a reversible disease that can be successfully treated with control of the supragingival biofilm [8]. Plaque control is a critical component in all aspects of both periodontal and peri-implant diseases. Serino and Strom [9] reported that peri-implant lesions were associated with inadequate plaque control at the implant sites and rarely occurred around implants when proper plaque control was ensured. More surprisingly, Aguirre-Zorzano et al. [10] found that the prevalence of mucositis and peri-implantitis in periodontitis patients, even with regular supportive periodontal treatment, was clinically significant, implying that these conditions will pose increasing therapeutic challenges. A recent systemic review [11] has shown that mechanical plaque control procedures effectively reduced plaque and gingivitis.
The importance of plaque control and oral hygiene education for preventing periodontitis and peri-implantitis is well recognized [1]. Many plaque index systems [12131415161718192021] have been used to help improve patients' oral hygiene. In addition, several more detailed and sensitive plaque indices [17192122] have been introduced in clinical studies. However, despite their advantages, these indices are not well known among dentists or even periodontists. Therefore, they are not commonly used for oral hygiene education in patients with periodontitis or peri-implantitis. A good index system for daily practice must be simple and versatile, so that it is easily understood by inexperienced examiners and can be reproduced by different clinicians [23]. The O'Leary plaque control record (PCR) has been used for oral hygiene instruction since it was first introduced in 1972 [15]. Although the PCR corresponds to these requirements, it is difficult to perform at every visit for several reasons. It takes approximately 5 minutes for examiners to evaluate the PCR. Some patients complain about the disclosing solution because it stains the entire dentition. In addition, the PCR system is unable to precisely evaluate the quantity of plaque. The Silness and Löe plaque index (PlI) system has also been used to evaluate patients' oral hygiene status [13]. The PlI system has several advantages. It consists of 3 grades that depend on the quantity of plaque. It requires fewer teeth than does the PCR. However, there is sometimes confusion regarding the teeth used in this plaque scoring system. In addition, the second molars, which are more difficult to clean than the other teeth, are not analyzed in this system. Therefore, we combined the 2 most familiar indices (the PCR and PlI) into the modified plaque score (MPS).
This study aimed to assess the validity of the MPS and to compare it to the PCR and PlI for the evaluation of tooth brushing instructions.
MATERIALS AND METHODS
Patient selection and experimental design
This study was designed as a parallel-group, randomized clinical trial. It was performed at the Department of Periodontology, Hanyang Medical Center, Seoul, Korea. Between 2012 and 2014, 124 patients with periodontitis were recruited. Patients were enrolled in this study if they met the following inclusion criteria: 1) age ≥20 years; 2) ≥20 natural teeth; and 3) presence of proximal attachment loss of ≥3 mm in ≥2 non-adjacent teeth [24]. The exclusion criteria were as follows: 1) age <20 years; 2) <20 natural teeth; 3) use of a powered toothbrush; 4) pregnancy; 5) acute or chronic immune disturbance; 6) gingival hyperplasia because of the use of immunosuppressive drugs or calcium-channel blockers; 7) the use of antibiotics, steroids, non-steroidal anti-inflammatory drugs, or anticoagulants at the beginning of the study or clinical examinations; and 8) cognitive impairment. The protocol for human subjects was reviewed and approved by the Institutional Review Board of Hanyang University Hospital (HYUN IRB No. 2012-19-019-001). The study was performed according to the Consort statement [25] and was registered on http://cris.nih.go.kr (No. PRE20170628-004).
Evaluation of tooth brushing instruction with 3 different plaque indices
The evaluation consisted of 5 visits over 8–12 weeks. All subjects received comprehensive periodontal treatment, including oral hygiene instruction, scaling, and a series of root planing.
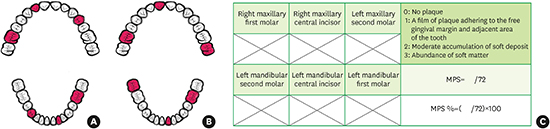
At the first visit, the clinician confirmed the absence of the exclusion criteria. The participants were also asked to provide informed written consent and to complete a questionnaire on sex, age, and brushing time and frequency. Any participants who did not meet the criteria for periodontitis based on radiographic and clinical criteria or refused to participate in this study were excluded (n=4). The participants were then randomly allocated either to the conventional tooth brushing instruction (C-TBI) group (n=60) or the professional intraoral tooth brushing instruction (P-TBI) group (n=60) (Figure 1). The randomization was performed using sequentially numbered, opaque, and sealed envelopes (P.S.H.). The clinical parameters, including probing pocket depth (PPD) and clinical attachment level (CAL), were evaluated by a blinded periodontist (C.S.H.). PPD was recorded to the nearest millimeter at 6 sites (mesiobuccal, mid-buccal, distobuccal, mesiolingual, mid-lingual, and distolingual) using a periodontal probe (Williams probe, Hu-Friedy, Chicago, IL, USA). The CAL was evaluated by measuring from the cementoenamel junction to the base of the periodontal pocket. Gingival inflammation was recorded according to the Löe and Silness gingival index (GI) [26], which was assessed at 4 sites (mesiobuccal, mid-buccal, distobuccal, and lingual) on 6 teeth (maxillary right first molar, maxillary right lateral incisor, maxillary left first premolar, mandibular right first premolar, mandibular left lateral incisor, and mandibular left first molar). The presence of plaque was recorded with the PlI [13], PCR [15], and MPS. After applying a disclosing solution to each tooth, the PlI, PCR, and MPS were evaluated at 4 sites (mesiobuccal, mid-buccal, distobuccal, and lingual). The PlI was evaluated on 6 teeth (maxillary right first molar, maxillary right lateral incisor, maxillary left first premolar, mandibular right first premolar, mandibular left lateral incisor, and mandibular left first molar). The PCR was determined by the percentage of total surfaces (4 aspects per tooth) with plaque [15]. The MPS was recorded on 6 teeth (maxillary right first molar, maxillary right central incisor, maxillary left second molar, mandibular right second molar, mandibular left central incisor, and mandibular left first molar) according to the criteria of the PlI (Figure 2). The MPS included the 2 second molars where the highest mean total counts of microbial species were found [27]. The MPS percentage was calculated according to the following formula:

 | Figure 1Flow chart of the participants in this study.
C-TBI: conventional tooth brushing instruction, P-TBI: professional intraoral tooth brushing instruction, PCR: O'Leary plaque control record, MPS: modified plaque score.
|
 | Figure 2Six teeth were evaluated to record the PlI (A) and the MPS (B). The MPS was assessed according to the criteria of the PlI using a disclosing solution (C).
PlI: Silness and Löe plaque index, MPS: modified plaque score.
|
After the clinical evaluation, scaling was performed to remove all supragingival plaque deposits and dental calculus. The participants in both groups were asked to clean their teeth to the best of their ability using their own oral hygiene devices. The participants in the professional tooth brushing instruction group were asked to bring their personal toothbrushes and interproximal brushes to the next visit.
At the second visit, the GI, PlI, PCR, and MPS were assessed. In the C-TBI group, the instructor (P.S.H.) demonstrated the required brushing technique using a dentiform model and a demonstration toothbrush. The participants in the professional tooth brushing instruction group were presented with the same information by the same instructor (P.S.H.). However, in the professional tooth brushing instruction group, the instructor showed the participant the uncleaned tooth surfaces after applying a disclosing solution. The instructor was aware of individual skill deficits, which were also reported to each participant. The instructor emphasized all information relevant to overcome these deficits at each respective site. If, for instance, a participant had neglected the lingual surfaces while the buccal surfaces were fairly clean, the intervention emphasized how to brush the lingual surfaces with the modified Bass technique. The instructor showed the participant how to brush uncleaned tooth surfaces directly using the participant's own toothbrush in the participant's mouth. In both groups, the instructions were designed to last approximately 10 minutes. All the participants were given the same manual toothbrush (Systema genki, Lion Co., Tokyo, Japan) and interproximal brush (Systema interdental brush, Lion Co., Tokyo, Japan) to minimize confounding factors depending on the toothbrush type. In addition, the instructor recommended the same brushing time (3 minutes) and brushing frequency (at least twice a day) to the participants in both groups. After oral hygiene instruction with the 2 different techniques, root planing was performed in both groups. Three visits for root planing procedures were completed before the re-evaluation.
After a series of root planing procedures, all participants were reevaluated using the GI, PlI, PCR, and MPS. Clinical parameters including the PPD and CAL were also evaluated. The participants were only aware of the general aim of the study in order to avoid the Hawthorne effect.
Convergent validity of the MPS
Several methods exist for proving the validity of a scoring system of plaque quantity. The most popular method of evaluating the correlation of a novel system with another index (that is already well established and considered to be standard) is to assess its convergent validity [21]. The PlI and PCR are widely used and considered to be standard plaque indices. Therefore, we used the PlI and PCR to assess the convergent validity of the MPS.
Comparison of evaluation time for the PCR and MPS
The evaluation time for the PCR and MPS was assessed in the patients who had complied with the 3-month recall system. To minimize inter-rater differences, a single experienced periodontist (C.S.H.) taught 40 students how to assess the PCR and MPS. In the first week, 40 students evaluated patients' oral hygiene status using the PCR and MPS. The evaluation time was measured using a stopwatch (Compact stop watch, Morning Glory Co., Seoul, Korea). After 2 weeks of training, the evaluation time for PCR and MPS by the same students was re-assessed. The evaluation time ratio (PCR/MPS) was calculated and compared between the first and third weeks.
Intraexaminer reliability
Scaling and a series of root planing procedures were performed by one periodontist (H.J.Y.). All clinical parameters, including the PPD and CAL, were measured by a blinded examiner (C.S.H.). The PlI and MPS were evaluated twice by the same examiner (C.S.H.). The reproducibility of the PlI and MPS measurements was assessed with Bland-Altman plots and intraclass correlation coefficients.
Statistical analysis
All statistical analyses were performed using a commercially available software program (SPSS version 21.0, IBM Corp., Armonk, NY, USA). Metric variables (e.g., age) were reported as means with standard deviations. Sample size was calculated with a test power of 0.8, considering a 10% dropout rate. Normality was assessed using the Kolmogorov-Smirnov test and the Shapiro-Wilk test. All clinical parameters were shown to correspond with the assumption of normal distribution. The differences between the C-TBI group and the professional tooth brushing instruction group were evaluated using the independent t-test. The differences in the clinical parameters at baseline, after scaling, and after a series of root planing for each group were evaluated using repeated-measures analysis of variance. The convergent validity of the MPS with the PCR and PlI was evaluated using the Pearson and Spearman correlations. The evaluation time for the PCR and MPS was evaluated with the Student's t-test to assess differences between the 2-time points. P values <0.05 were considered to indicate statistical significance.
RESULTS
Evaluation of tooth brushing instruction with 3 different plaque indices
The characteristics of the study group are presented in Table 1. The mean age was 53.84±10.55 years in the C-TBI group (n=56) and 56.05±11.02 years in the professional intraoral tooth brushing group (n=60). There were no statistically significant differences between the groups with regard to age, sex, brushing time, or brushing frequency. The mean brushing frequency of the entire study group was 2.51±0.70 times per day.
Table 1
Patient characteristics at baseline

Values are presented as mean±standard deviation.
C-TBI: conventional tooth brushing instruction, P-TBI: professional intraoral tooth brushing instruction.
![]()
There were no differences between the groups in the baseline mean GI, PlI, MPS, and PCR values (Table 2). At baseline, the mean PlI was 1.31±0.22 and the mean MPS was 1.58±0.37 in the C-TBI group. In the P-TBI group, the mean PlI was 1.37±0.44 and the mean MPS was 1.56±0.44 at baseline. In the C-TBI group, the mean MPS percentage was 52.58%±12.26% and the mean PCR was 30.4%±5.37% at baseline. At baseline, the mean MPS percentage was 51.92%±14.68% and the mean PCR was 30.16%±6.4% in the P-TBI group. After root planing, there were significant differences between the 2 groups in the mean PlI, PCR, and MPS values (P=0.031, P=0.017, and P=0.023, respectively) (Figure 3). The mean MPS percentage in the C-TBI group (37.59%±11.11%) was significantly greater than that in the P-TBI group (32.69%±10.19%) after root planing (P=0.023). After root planing, the mean PCR score was 20.09%±3.77% and 18.32%±3.79% in the C-TBI group and the P-TBI group, respectively. Statistically significant differences were found between the C-TBI group and the P-TBI group (P=0.031).
Table 2
Evaluation of tooth brushing instruction with 3 different plaque indices (mean±SD)

SD: standard deviation, C-TBI: conventional tooth brushing instruction, P-TBI: professional intraoral tooth brushing instruction, GI: Löe and Silness gingival index, PlI: Silness and Löe plaque index, MPS: modified plaque score, PCR: O'Leary plaque control record, CAL: clinical attachment level, PPD: probing pocket depth, NA: not assessed.
a)Statistically significant difference between the C-TBI and P-TBI groups (P<0.05).
![]()
 | Figure 3After scaling and root planing with 2 different oral hygiene instruction techniques, the mean PlI scores improved in both groups (A). Changes in the MPS (B) and the PCR (C) in the 2 groups. Improvements in oral hygiene status were significantly greater in the P-TBI group than the C-TBI group according to all 3 plaque indices.
PlI: Silness and Löe plaque index, MPS: modified plaque score, PCR: O'Leary plaque control record, P-TBI: professional intraoral tooth brushing instruction, C-TBI: conventional tooth brushing instruction.
a)Statistically significant difference (P<0.05).
|
Convergent validity
Table 3 shows the convergent validity of the MPS measurements with the other plaque scoring systems. The correlations between the MPS percentage and PCR were 0.855 (Pearson correlation coefficient) and 0.861 (Spearman correlation coefficient) after a series of root planing. The Pearson correlation coefficient and Spearman correlation coefficient for the MPS and PlI were 0.863 and 0.884, respectively. The MPS showed significant concurrence with the PCR and PlI in both groups.
Table 3
Correlations of MPS measurements with the PCR and PlI

Statistically significant for all values (P<0.01).
MPS: modified plaque score, PCR: O'Leary plaque control record, PlI: Silness and Löe plaque index, C-TBI: conventional tooth brushing instruction, P-TBI: professional intraoral tooth brushing instruction.
![]()
Comparison of evaluation time for the PCR and MPS
The mean time for PCR assessment was 361.51±75.61 seconds in the first week (Table 4). After 2 weeks of education and training, the mean time for PCR assessment decreased to 298.18±45.40 seconds in the same students. The mean time for MPS assessment was 142.90±32.57 seconds in the first week. The mean time for MPS assessment in the third week was 113.01±24.02 seconds. In the first week, the mean time for PCR assessment was 2.58±0.50 times longer than that for MPS assessment. After 2 weeks of training, the mean time for PCR assessment was 2.76±0.71 times longer than that for MPS assessment.
Table 4
Comparison of evaluation times for the PCR and MPS in the first and the third weeks (mean±SD)

![]()
DISCUSSION
This study sought to determine the efficacy of the MPS for the evaluation of oral hygiene status in periodontitis patients. It further assessed the convergent validity of the MPS with the PCR and PlI.
We evaluated the efficacy of the MPS in comparison with 2 different plaque indices in patients receiving tooth brushing instructions. The goal of self-performed mechanical plaque control is to establish optimal supragingival plaque control. This is based on the cooperation and confidence of both patients and clinicians. Clinicians must motivate their patients to change their established habits. Many studies have addressed the importance of the doctor-patient relationship in health outcomes [28-30]. Oral hygiene programs should include self-assessment, self-examination, self-monitoring, and self-instruction. To facilitate these behaviors, a disclosing solution was used to visualize dental plaque on the patients' teeth. The visualization of bleeding gingival sites and plaque with the disclosing solution may encourage patients to change their behavior. While PlI measurements were assessed without using a disclosing solution, we used a disclosing solution to visualize sites of plaque accumulation more prominently, which minimized inter-rater errors in recording the plaque indices. This solution also confirmed the effectiveness of tooth brushing techniques on plaque removal.
In this study, we evaluated the convergent validity of the MPS with the PCR and PlI. Both PCR and PlI measurements are internationally well-accepted and validated standard plaque indices. The correlation between the MPS percentage and PCR was statistically significant (P<0.01), and the correlation between the MPS and PlI showed statistically significant convergent validity (P<0.01). The MPS percentage values were higher than those of PCR in both groups at 3 different time points. This can be beneficial for motivating patients receiving oral hygiene education. In addition, the values of the MPS were higher than those of the PlI in both groups at 3 different time points. Both indices used the same number of teeth (n=6) and the same grading system (0, 1, 2, and 3). However, we evaluated 2 second molars in the MPS rather than 2 premolars in the PlI. Therefore, the motivation and education using the MPS enabled participants to improve their oral hygiene more efficiently. Several sensitive plaque indices [16192131] have been also introduced. A new method of plaque scoring [19] was reported to have less variability within and between examiners than the Turesky modification of the plaque index by Quigley and Hein [12]. The new marginal plaque index [21] showed a high sensitivity to marginal plaque accumulation. Even though these plaque indices are sensitive and beneficial for clinical research, it is difficult to put these plaque indices to use in daily practice for several reasons. The criteria of these indices are rather complicated and sometimes confuse examiners who are accustomed to another plaque index system.
To minimize confounding factors, participants in both groups were given the same toothbrushes and interdental brushes after 2 different sessions of tooth brushing instructions. In addition, we recommended the same brushing time and frequency to the participants in both groups. As shown by van der Weijden et al. [32], an optimal result is achievable after 3 minutes of manual brushing. A recent systemic review [33] suggested that brushing for 2 minutes or longer should be encouraged, regardless of the brush type. In Korea, people are taught (from kindergarten) to brush their teeth for 3 minutes after meals, 3 times a day. A recent clinical study [34] suggested that self-performed mechanical plaque control at 12- or 24-hour intervals was sufficient to maintain periodontal health in patients with no or limited clinical attachment loss. Therefore, we recommended that the participants brush at least twice a day.
A previous study of tooth brushing instructional methods concluded that individual direct instructional methods (using a dentiform model and a toothbrush) had little effect during a 2-week period and no effect after 2 weeks [35]. Harnacke et al. [36] showed similar results to that study [35]. They found that a single computer-based training session had limited effects that waned after 12 weeks. Repetitive training might be needed to habituate patients to the required brushing technique. Although the proper use of a plaque index system can facilitate efficient tooth brushing instruction, we hesitate to use any of them because of the time and effort required. In the present study, P-TBI using several plaque indices contributed to improvements in patients' oral hygiene compared to the results obtained using a C-TBI technique. Repetitive training with easily accessible plaque index systems will produce more efficient and more successful oral hygiene programs. We compared the evaluation time of PCR and MPS according to the examiner's proficiency. After 2 weeks of education, previously untrained examiners could use the MPS to assess a patient's oral hygiene status in one-third of the evaluation time of PCR measurements.
The primary strength of this study is that we compared 2 different tooth brushing instruction techniques for evaluating the efficacy of the MPS compared with the PlI and PCR. In addition, most studies [343637] of mechanical plaque control have been conducted in adults with gingivitis. However, this study was performed in periodontitis patients, which enabled periodontists to educate patients about oral hygiene more effectively using the new plaque scoring system (MPS). A limitation of this study is that it focused on short-term changes in oral hygiene following an educational program. Future long-term studies are needed to investigate the maintenance of oral hygiene behavior after P-TBI using the MPS.
This study showed the efficacy of the MPS in tooth brushing instruction in periodontitis patients. The MPS showed good concurrence with the PlI and PCR. Therefore, we believe that the MPS can be used as a plaque scoring system like the PlI and PCR in oral hygiene education. In addition, the MPS seems to be useful for repetitive oral hygiene education, as it requires less time. The MPS measurements are practical and can be easily applied in clinical settings, regardless of the examiner's experience. Therefore, it is suggested that repetitive oral hygiene education using the MPS will promote patients' periodontal health during supportive periodontal treatment, as well as during the active treatment of periodontitis and peri-implantitis.
 XML Download
XML Download