

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Osteoporotic vertebral fractures (OVFs) are one of the common causes of disability. As of 2012, there were 2,018,236 persons with osteoporosis and 243,054 persons with OVF in Korea, which represented 3.94% and 0.48%, respectively, of the entire Korean population (51,169,141).1 The incidence of OVFs increases rapidly with age in both sexes.2 This imposes a very significant burden on society, which will increase markedly in the near future.3
The spine is considered to be in neutral sagittal alignment when a gravity plumb line extending from the center of the C7 vertebral body bisects the S1 endplate.4 Sagittal imbalance is a condition that occurs as a result of the loss of the normal lumbar lordosis or an increase in thoracic kyphosis, or both, resulting in the forward displacement of the head relative to the sacrum and pelvis.4 Sagittal imbalance can have a variety of causes; among them, degenerative sagittal imbalance5 and post-traumatic deformities6 are main causes which affect elderly patients. Sagittal imbalance can cause abnormal posture, gait disorder, and a high risk of falling.7 When OVFs happen, posttraumatic kyphosis develops and the C7 plumb line (C7PL) passes anteriorly to the sacrum, which is considered positive sagittal balance.8 People with positive sagittal balance try to restore a global sagittal balance by the compensatory changes in alignment at the levels above and/or below the deformity in the spinal column (cervical lordosis increases or thoracic kyphosis decreases, and lumbar lordosis increases), spinopelvic parameters (pelvic tilt is increased with a decreasing sacral slope), and lower extremity (knee flexion and ankle dorsiflexion) in order to gaze horizontally, to reduce pain and energy consumption from sagittal imbalance.9
Imagama et al.10 reported that sagittal balance was well maintained in subjects with both good spinal mobility and back muscle strength. Haenyeo, Korean traditional unassisted free-diving women, have more superior back muscle strength than the general population for characteristics of their work. Therefore, they are good candidates for studying compensatory mechanism after sagittal imbalance by OVF. To the author's knowledge, there is only one study about the bone mineral density (BMD) of Haenyeo,11 and there is no study about the sagittal imbalance and compensatory mechanism in Haenyeo population. The purpose of this study was to compare BMD and the compensatory mechanism after OVFs between woman divers and controls.
METHODS
Between January 2010 and December 2014, traditional woman divers, or Haenyeo, and non-diving women who visited our hospital for a routine health checkup, back pain, or osteoporosis were investigated. The inclusion criteria were 1) patients who had undergone a BMD scan; 2) patients who had undergone whole spine X-ray; and, 3) patients with more than 1 year of follow-up. The exclusion criteria were 1) any history of lumbar spinal surgery; 2) the presence of any other disease affecting secondary osteoporosis; and 3) pathologic fractures of the thoracolumbar spine. Overall, 63 patients met all the inclusion criteria.
BMD
BMD was performed after the time point of diagnosis of OVFs in the fractured patient group. In the non-fracture patient group, BMD was chosen at the nearest time point of whole spine X-ray. BMD (in g/cm2) was measured using dual-energy X-ray absorptiometry (DXA) (Hologic QDR-1500; Hologic Inc., Marlborough, MA, USA). BMD of the lumbar spine (L1–4) was measured in the standard anteroposterior projection. All evaluable vertebrae were used and vertebrae that were affected by local structural change or artifacts were excluded. Anatomically abnormal vertebrae may be excluded from the analysis if there was a more than 1.0 T-score difference between the vertebra in question and adjacent vertebrae. BMD of the femoral neck was also measured. The results are presented as BMD (g/cm2) and as T-scores. Comorbidities, which could affect bone mineral densities, were assessed by the Elixhauser Comorbidity Index.12
Global sagittal balance
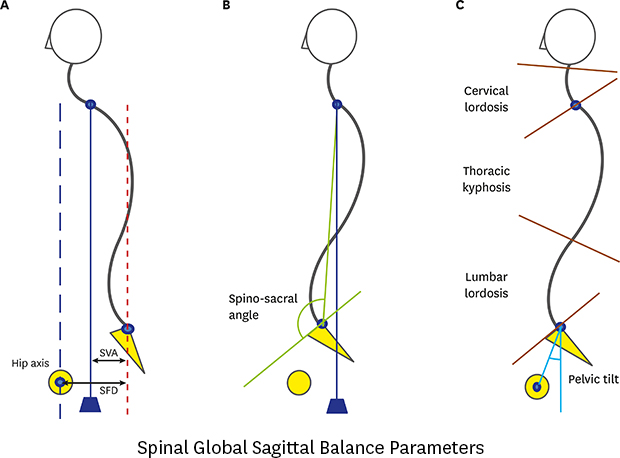
Plain radiographs of the thoracolumbar spine were taken using a standard tube-to-film distance of 1.8 m, for all patients, to maintain a constant magnification factor. Standing anteroposterior and lateral radiographs of the lumbar spine were obtained from all patients. Standing long cassette radiographs (14" × 36") are taken to include the entire spine from the base of the occiput to the distal sacrum and the femoral heads. The global spinal sagittal balance is determined using the C7PL dropped vertically from the center of the body of C7. For the radiological assessment, sagittal vertical axis (SVA) which is the offset from C7PL to the posterior superior corner of the first sacral vertebra was measured.13 The SVA to sacro-femoral distance (SFD) ratio (SVA/SFD)9 was calculated (Fig. 1A), and the spino-sacral angle9 was measured to evaluate global sagittal balance (Fig. 1B).
 | Fig. 1Parameters to evaluate global sagittal balances. (A) Three vertical lines from the vertical bicoxo-femoral axis (hip axis line), posterior of the sacrum (vertical sacral line), and center of the C7 body were drawn. The SVA is the distance from the vertical sacral line to the C7PL. The SFD is the horizontal distance between the vertical bicoxo-femoral axis and the vertical line passing through the posterior corner of the sacrum. The SVA/SFD ratio was then calculated. (B) The spino-sacral angle was measured between the parallel line of the sacral upper endplate and the line between the posterior corners of the sacrum to the center of C7. (C) Cervical lordosis was measured from the C2 lower endplate to the C7 upper endplate; thoracic kyphosis was from the T4 lower endplate to the T12 lower endplate, and lumbar lordosis was from the L1 upper endplate to the S1 endplate. Pelvic tilt was determined as the angle between a line from the hip center to the posterior superior corner of the sacral promontory and the vertical sacral line.SVA = sagittal vertical axis, C7PL = C7 plumb line, SFD = sacro-femoral distance.
|
Compensation mechanism
On whole spine standing X-ray, cervical lordosis from the C2 lower endplate to the C7 upper endplate, thoracic kyphosis from the T4 lower endplate to the T12 lower endplate, lumbar lordosis from the L1 upper endplate to the S1 endplate, and pelvic tilt were assessed as compensation parameters (Fig. 1C). These procedures were conducted at the initial visit and at 3, 6, and 12 months thereafter.
Statistical analysis
We calculated sample size based on the results of a previous study of Haenyeo.11 In that study, the mean ± standard deviation (SD) of ‘total hip’ BMD was 1.003 ± 0.113 g/cm2 in premenopausal Haenyeo and 0.864 ± 0.08 g/cm2 in a control group. The sample size calculated by a two-sample t-test with a two-sided alpha of 0.05, a power of 0.90, and a kappa of 1, which was used to compare mean group differences (as in the SAS system), was approximately 15 patients. Our study included more than 30 patients in each group. Two experienced spinal surgeons independently measured each parameter twice. The same reader, or a second reader blinded to patient identity, independently evaluated the plain radiographs and DXA scans. Test–retest and interobserver reliabilities for the various measurements were evaluated using a different dataset. Normality tests (Kolmogorov-Smirnov and Shapiro-Wilk) were performed to assess the distribution of our data and if data from at least one group did not normally distribute, we performed a non-parametric method. As parametric methods, the Student's t-test was performed. As non-parametric methods, Mann-Whitney test was executed to compare two groups, and correlation analysis (Kendall's tau b, Spearman's rho) were performed. In order to make comparisons across 2 groups (fractured vs. non-fractured) with 2 independent categorical variables (divers vs. non-divers), 2-way analysis of variance was performed. All statistical analyses were performed using the SPSS 14.0 statistical software package (IBM Corp., Armonk, NY, USA). Results are expressed as means ± SD. A P value < 0.05 was deemed to indicate statistical significance.
RESULTS
Thirty woman divers and thirty-three non-diving women were enrolled in this study. The demographic data of the patients were described in Table 1. The mean age of the woman divers was 72.1 ± 4.7 years and that of the controls was 72.7 ± 4.0 years (P = 0.61). The mean height was 1.51 ± 0.06 m in diver and 1.52 ± 0.06 m in controls (P = 0.49). The mean weight was 55.0 ± 10.2 kg in divers and 58.1 ± 7.4 kg in controls (P = 0.17). The mean body mass index (BMI) was 24.0 ± 3.7 kg/m2 in divers and 25.2 ± 2.9 kg/m2 in controls (P = 0.07). Fourteen divers and seventeen controls were found to have vertebral fractures. The mean number of fractured vertebrae was 1.9 ± 1.1 (range, 1–4) in the divers and 1.8 ± 0.8 (range, 1–3) in the controls. Test–retest evaluation of the radiographic variables indicated that the repeatability was excellent, with intraclass coefficients of 0.82 and 0.79 for the divers and non-divers, respectively; the interobserver values were also excellent, with intraclass coefficients of 0.78 and 0.85, respectively.
Table 1
Patient characteristics

Data are presented as means ± standard deviation (range) or number (%).
BMI = body mass index, DXA = dual-energy X-ray absorptiometry, BMD = bone mineral density, N/A = not applicable for statistical analysis, SERM = selective estrogen receptor modulator, BP =bisphosphonate.
aComorbidities from the Elixhauser comorbidity index.12
![]()
BMD
No statistical difference was found in BMD between the divers and controls (Table 2). In both the diver and control groups, there was no statistical subgroup difference between the fracture group and non-fracture group (Table 2). In the fracture subgroup, no statistical difference was found between the divers and controls (Table 3).
Table 2
Comparison between the fracture and non-fracture subgroups of the diver and control groups

Data are presented as means ± standard deviation (range) or number (%).
ANOVA = analysis of variance, BMI = body mass index, DXA = dual-energy X-ray absorptiometry, BMD = bone mineral density, SVA = sagittal vertical axis, SFD = sacro-femoral distance.
aMann-Whitney test was performed because the date of at least one group is not normally distributed.
![]()
Table 3
Comparison between divers and controls in terms of osteoporotic vertebral fracture

Data are presented as means ± standard deviation (range) or number (%).
BMI = body mass index, DXA = dual-energy X-ray absorptiometry, BMD = bone mineral density, SVA = sagittal vertical axis, SFD = sacro-femoral distance.
aMann-Whitney test was performed because data of at least one group is not normally distributed.
![]()
Global sagittal balance
Global sagittal balance was compared between the fracture and non-fracture subgroups in both the diver and control groups (Table 2). In the divers, SVA and SVA/SFD were statistically larger in the fracture group compared to the non-fracture group (P = 0.001 and P = 0.018, respectively). However, the spino-sacral angle showed no significant difference between the fracture group and non-fracture group. Within the fracture patients, SVA was statistically longer in the divers than in the controls (P = 0.008) (Table 3).
Compensatory mechanism
In divers, cervical lordosis and pelvic tilt were significantly increased in the fracture subgroup compared to the non-fracture subgroup (P = 0.028 and P = 0.008, respectively) (Table 2). SVA was statistically significantly correlated with cervical lordosis (Kendall's tau b R = 0.28, P = 0.03, Spearman's rho R = 0.41, P = 0.03), lumbar lordosis (Kendall's tau b R = −0.37, P = 0.004, Spearman's rho R = −0.49, P = 0.006), and pelvic tilt (Kendall's tau b R = 0.29, P = 0.02, Spearman's rho R = 0.46, P = 0.01) in divers. However, any sagittal parameter was not significantly correlated with SVA in control group (Fig. 2). Because thoracolumbar fracture is a main contributor of kyphosis and positive sagittal balance, we excluded lumbar lordosis in compensatory parameters. Therefore, cervical lordosis and pelvic tilt can act as a compensatory mechanism in divers but in control group, no compensatory mechanism acted against positive sagittal balance.
 | Fig. 2Scatter plot matrix of divers and controls. (A) SVA was significantly correlated with cervical lordosis (Kendall's tau b R = 0.28, P = 0.03, Spearman's rho R = 0.41, P = 0.03), lumbar lordosis (Kendall's tau b R = −0.37, P = 0.004, Spearman's rho R = −0.49, P = 0.006), and pelvic tilt (Kendall's tau b R = 0.29, P = 0.02, Spearman's rho R = 0.46, P = 0.01) in divers. (B) No sagittal parameter was significantly correlated with SVA in the control group.SVA = sagittal vertical axis.
|
DISCUSSION
Some physical exercises exert anabolic effects on bone through both gravity and joint reaction forces.1415 Underwater activities are subjected to stress from water pressure, from the forces generated when their muscles resist water pressure, and from weightlessness.1617 In response to the strain or deformation caused by forces from muscle contraction and/or impact, osteoclasts and osteoblasts are stimulated to remodel bone.1819 Water pressure exerts a load on bones and muscles during diving, with pressure increasing by one atmosphere for every 10 m of depth. Such loading helps bone to augment mineralization.1116 Instead, the weightlessness acts in opposition to the water pressure and joint reaction force.16 Studies in swimmers showed no positive effects of swimming on bone mineral densities.2021 However, in contrast to the swimmers or scuba divers, muscular contractions against the resistance of the water are thought to be much stronger in Haenyeo because tides and waves underwater behave in unpredictable ways. Studies in mice have demonstrated that high-impact, irregular, multiplanar loads and slower load-relax cycles are more effective at increasing bone mass than the lower-impact, repetitive, higher frequency, uniplanar loads characterized in endurance sports.1819 In addition, respiratory acidosis due to breath holding may have an additional consideration in their bone metabolism.
“Culture of Jeju Haenyeo” was inscribed on the representative list of the intangible cultural heritage of humanity by United Nations Educational, Scientific and Cultural Organization in 2016.22 Previous reports11 stated that they made 113–138 dives per day and remained in the water for a total of 170–200 minutes per day, of which only 52–63 minutes were spent diving submerged, with the remaining time spent at the surface. The average number of working days for these divers was 14.6 ± 5.3 days per month. The diving pattern of Korean woman divers was similar in both summer and winter. However, recently, such unassisted diving has been substituted by scuba diving and the number of new traditional divers is diminishing rapidly. The average age of woman divers is increasing, and they tend to suffer from osteoporosis and OVF. We hypothesized that the back muscle strength of Haenyeo is superior to that of women from the general population because their underwater lifestyle produces a higher demand for muscle strength. Even if the number of Haenyeo is decreasing, this study is thought to be very valuable because these days most urban people have a sedentary life style, especially when they are getting old. Haenyeo is a unique population who worked in the sea, which has extreme conditions, from their early life times. Therefore, we can further evaluate this population to investigate the importance of exercise to affect the muscle and bone. Back extensor strength has been shown to have a negative correlation with kyphosis 2324 and a positive correlation with the BMD of the spine.25 If Haenyeos suffer from OVF, the compensatory mechanism is activated to a much greater extent relative to women from the general population. In this study, cervical hyperlordosis and pelvic back tilt occurred in divers to compensate for posttraumatic kyphosis in OVF. However, this compensation mechanism was not present in the control group. We assumed that the reason for this difference was the superior spinal mobility and back muscle strength of the divers. This study proves exercise can help spinal mobility and balance even after vertebral fracture in old age.
A previous study reported that the BMD of Haenyeo was higher than that of controls in the total hip and femur neck region, but the BMD of the proximal femur in Haenyeo decreased more rapidly with age than that of the controls in all three areas of the proximal femur.11 In the present study, there was no difference between Haenyeo and the controls in terms of the BMD of both the spine and femur in the postmenopausal period. Divers are occasionally subjected to increased blood carbon dioxide levels, which is a weak stimulus for bone resorption in vitro,26 suggesting that this might be an alternative pathway for bone loss independent of the effect of weight-bearing. When Haenyeos hold their breath, they enter a temporal respiratory acidosis condition, even though this is recovered by physiologic compensation. Some experiments reported that metabolic, but not respiratory, acidosis favors osteoclastic bone resorption.27 The role of blood carbon dioxide in the bone metabolism of divers has not yet been elucidated. Pereira et al.17 reported that a group of professional scuba divers had a femoral neck BMD 4.6% lower than that of the control group. On the contrary, Wesolowska et al.16 reported that there were no significant differences in BMD or bone mineral content between two similar groups in terms of the entire skeleton, lumbar spine, and femoral neck. They suggested that diving does not appear to affect bone catabolism. However, the mean diving time in their study was shorter than that of Pereira et al.'s study.17
Our study had a number of limitations. First, this was a retrospective study. We focused on the BMD and spinal sagittal balance in this study. We could not measure back muscle strength. We could not survey each individual's diving pattern. In the future, we intend to investigate not only BMD, but also muscle mass, strength and physical performance (i.e., an evaluation of sarcopenia) in Haenyeo. Second, a small sample size represents a further limitation. The decreasing number of young, healthy Haenyeo presents a challenge. Third, the compensation mechanism in the lower extremities (e.g., hip, knee, ankle) could not be investigated. A full view of the entire skeleton of the human body has recently been made possible, and this may help in evaluations of spine and lower extremity compensation.
In conclusion, BMD was not significantly different between our woman divers and the control group. When osteoporotic spinal fractures developed, compensatory mechanisms, such as increased cervical lordosis and pelvic tilt, were activated more in the woman divers; this may be due to the superior back muscle strength of the diver group.
 XML Download
XML Download