

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Obesity has reached epidemic levels, not only in Caucasians but also in Asians.12 The prevalence of overweight people of Asian descent, as defined by the World Health Organization (WHO)'s criteria for Asians, has steadily increased from 31.7% in 2007 to 33.2% in 2015. This prevalence has especially increased in Korean men, from 36.2% to 39.7%.3 Obesity is strongly associated with the risk of diabetes mellitus, dyslipidemia, hypertension, and cardiovascular diseases.4 Furthermore, obesity can lead to atherosclerosis as a result of a disruption of endothelial function, as well as enhancing oxidative stress and pro-inflammatory status.5 Due to the increasing prevalence of obesity, cardiovascular disease and related mortality rates have also increased.6 Coronary artery bypass grafting (CABG) is one of the most common surgical procedures, and it was shown to improve the survival of patients with severe angina.7 An awareness of obesity should be raised in patients undergoing CABG because obesity may be related to poorer post-surgical outcomes.8
The proportion of obese patients undergoing CABG is rising.9 Currently, the incidence of post-surgical acute kidney injury (AKI) has significantly increased because patients undergoing CABG are now generally older at the time of surgery, they have more overall preoperative comorbidities, and a larger proportion of patients may be undergoing emergent surgery than before.10 In this regard, studies have suggested a relationship among obesity, AKI,1112 or mortality13141516 patients with heart disease, although these results were not uniform possibly because of the heterogeneous patient characteristics.14151718 To our knowledge, no studies have elucidated a direct relationship among the three factors in patients after CABG. In addition, the reason why we focused on obesity specifically for Asian patients who underwent CABG is that information on risk factors for cardiac surgery-associated acute kidney injury (CSA-AKI) comes from many retrospective observational studies192021222324 but there no studies have focused on the correlation between AKI and body mass index (BMI). Accordingly, the purpose of the present study was to address the relationship among obesity, AKI, and long-term mortality in a large cohort of patients who underwent CABG.
METHODS
Study population
Data on patients undergoing CABG were retrospectively obtained from the aforementioned tertiary referral centers. A total of 3,089 consecutive patients underwent CABG between January 2003 and December 2015. Patients who were administered renal replacement therapy before surgery (n = 62), those who underwent revision CABG (n = 8), and those who were younger than 18 years old (n = 1) were excluded. Ultimately, 3,018 patients were included in the present analysis.
Data collection and definitions
The clinical parameters investigated were age, sex, current smoking and drinking status, hypertension, diabetes mellitus, history of myocardial infarction (MI), stroke, and peripheral vascular disease (PVD), prescribed medications, such as angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers, β-blockers, diuretics, and statins, history of coronary angiography (CAG) within 1 week before surgery, intraoperative use of a cardiopulmonary bypass (CPB), and perioperative use of an intra-aortic balloon pump (IABP). The left ventricular ejection fractions were determined using Simpson's modified biplane method from apical two- and four-chamber views on preoperative echocardiography. The baseline blood test findings, such as creatinine, white blood cell count, hemoglobin, and albumin, were examined. The C-reactive protein levels, which have high sensitivity, were not available for all the patients, so these were additionally adjusted as part of a sensitivity analysis. BMI was calculated as the body weight (in kilograms) divided by the square of the body height (in meters). The WHO's classification of the weight status of Asian people25 was used to categorize the patients as follows: underweight, < 18.5 kg/m2; normal weight, 18.5–23.5 kg/m2; overweight-at-risk, 23.5–25 kg/m2; obese I, 25–30 kg/m2; and obese II, ≥ 30 kg/m2. The creatinine levels were measured until 48 hours after surgery. The estimated glomerular filtration rates were calculated using the creatinine equation developed by the Chronic Kidney Disease Epidemiology Collaboration.26 As per the Kidney Disease Improving Global Outcomes guideline, AKI was determined in patients with either an increase in the serum creatinine level by ≥ 0.3 mg/dL or ≥ 1.5 times from the baseline. The additional patient outcome was all-cause mortality after surgery. All patients, except for those who were death-censored, were followed up until April 2017. The mortality data were obtained from the national database of the Statistics Korea.
Statistical analysis
All statistical analyses were performed using SPSS (version 23.0.; IBM Corp., Chicago, IL, USA) and STATA (version 12.0; Stata Corp LP, College Station, TX, USA). We described the baseline characteristics, after stratifying them by BMI. The means and their standard deviations were calculated for all continuous variables, and all categorical variables were reported as the percentage of participants in each category. The χ2 test was used to compare categorical variables. Comparisons between continuous variables were performed using an analysis of variance or a post hoc analysis of least significant difference, based on the number of comparison groups. Non-linear relationships were explored with a restricted cubic spline analysis. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using a logistic regression model, with and without adjustment of multiple covariates (age; sex; current smoking and drinking status; hypertension; diabetes mellitus; history of MI, stroke, and PVD; prescribed medications, such as ACEi or angiotensin receptor blockers, β-blockers, diuretics, and statins; history of CAG within 1 week before surgery; intraoperative use of CPB; and perioperative use of an IAPB; left ventricular ejection fraction; and blood findings, such as creatinine, white blood cell count, hemoglobin, and albumin). To assess the relationship between BMI and mortality, we created a Cox proportional hazard ratio (HR) model to consider covariates (AKI plus the aforementioned covariates). A P value less than 0.05 was considered significant.
RESULTS
Baseline characteristics
The baseline characteristics of the patients are shown in Table 1. The study included 3,018 patients (73.7% men), with a mean age of 66 ± 9.8 years. Of these patients, 37.4%, 2.4%, 21.1%, 35.1%, and 4.0%, were normal weight, underweight, overweight-at-risk, obese I, and obese II, respectively. At baseline, patients in the underweight group were older and had a higher prevalence of chronic kidney disease than did those in the normal-weight group. More patients were diagnosed with hypertension in the overweight group, including those who were overweight-at-risk, obese I, and obese II than those in the normal-weight group. Patients in the obese II group took more ACEi or angiotensin receptor blockers than did those in the normal-weight group. In addition, length of stay (i.e., hospitalization period) based on BMI, was as follows; normal, 19.3 ± 18.0 days; underweight, 26.0 ± 19.0 days; overweight-at-risk, 16.4 ± 17.5 days; obese I, 17.3 ± 23.4 days and obese II, 17.1 ± 13.8 days (underweight and overweight-at-risk, P < 0.05 compared with normal weight group). The length of hospital stay was longer in the underweight group than that in normal weight group.
Table 1
Baseline characteristics of the study participants
Comparisons were evaluated using the χ2 test for categorical variables and analysis of variance for continuous variables (post hoc analysis of least significant difference between the two groups). The normal-weight group served as a reference for the comparison between the two groups.
MI = myocardial infarction, PVD = peripheral vascular disease, CKD = chronic kidney disease, ACEi = angiotensin-converting enzyme inhibitors, ARB = angiotensin II receptor blocker, CAG = coronary angiography, CPB = cardiopulmonary bypass, IABP = intra-aortic balloon pump, LV = left ventricle, eGFR = estimated glomerular filtration rate.
aP < 0.05; bP < 0.01; cP < 0.001.
![]()
Relationship between BMI and post-surgical AKI
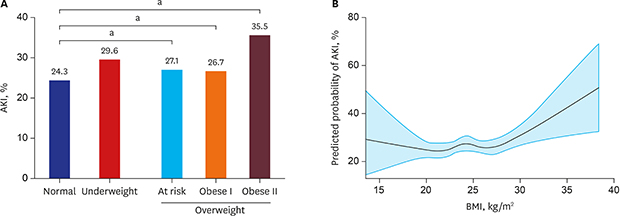
Post-surgical AKI developed in 799 patients (26.5%). The prevalence of AKI based on the BMI categories is presented in Fig. 1A. When a non-linear relationship was applied, the risk of AKI increased, depending on the increase in BMI (Fig. 1B). In the multivariate analysis, BMI ≥ 30 kg/m2 was associated with a higher OR for AKI (2.28; CI, 1.481–3.511) than was normal weight (Table 2). Although the C-reactive protein, which has high-sensitivity, was additionally adjusted in the multivariate model as a sensitivity analysis (n = 1,550), the relationship between obesity and AKI remained significant. Patients in the obese II group had a higher risk of AKI than did those in the normal weight group, with the following ORs: obese II, 2.31 (CI, 1.498–3.551), P < 0.001.
 | Fig. 1Prevalence of post-surgical AKI. (A) Proportions of post-surgical AKI according to the obesity categories. (B) Non-linear relationship between BMI and the risk of AKI.AKI = acute kidney injury, BMI = body mass index.
aP < 0.05.
|
Table 2
OR for post-surgical AKI by obesity classification

![]()
Effect of obesity on all-cause mortality after CABG
The relationship trend for mortality and obesity was different from that of the aforementioned relationship in post-surgical AKI. During the mean follow-up period of 74 ± 43.8 months (maximum: 13 years), 787 patients (26.1%) died. The mortality rate was 53.76 deaths per 1,000 person-years. The 5-year mortality rates for normal weight, underweight, overweight-at-risk, obese I, and obese II patients were 38.3%, 62.0%, 35.3%, 33.9%, and 38.8%, respectively (Fig. 2A), and their mortality rates were as follows: 31.4%, 62.0%, 20.4%, 22.0%, and 20.7%, respectively. The non-linear relationship analysis showed a similar pattern to these results (Fig. 2B).
 | Fig. 2Relationship between obesity and all-cause mortality. (A) Five-year survival rates based on the obesity categories. (B) Non-linear relationship between BMI and the 5-year survival rates.BMI = body mass index.
aP < 0.05.
|
Patients in the underweight group had a higher HR for mortality (2.85; CI, 2.085–3.905) than did those in the normal-weight group, whereas patients who were classified as overweight-at-risk, obese I, and obese II had lower HRs than did those in the normal-weight group, as follows: 0.60 (CI, 0.491–0.734), 0.61 (CI, 0.512–0.720), and 0.65 (CI, 0.436–0.981), respectively. In the multivariate analysis, patients in the underweight group tended to have poor survival, and those in the overweight and obese groups had better survival, remaining consistent (P for all, < 0.05) (Fig. 3 and Table 3). Additionally, the high-sensitivity C-reactive protein levels were adjusted in the multivariate model. The relationship between being underweight and high mortality was significant, with an HR of 2.15 (CI, 1.555–2.972) compared with that of normal-weight patients.
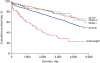
Table 3
HRs for all-cause mortality after surgery

![]()
AKI has been related with several morbidities as well as mortality in several pathologic conditions. Therefore, we analyzed the relationship between AKI and mortality, and obtained the statistically significant results with the following HRs; 1.51 (CI, 1.298–1.756). As a result, AKI was significantly associated with mortality.
DISCUSSION
The obesity epidemic has extended worldwide. Obesity is not only a risk factor for cardiovascular disease but also for several disease conditions, such as diabetes, fatty liver, and cancer, all of which can further contribute to the development of cardiovascular diseases.27 Recently, obesity was reported to be associated with various kidney diseases.28 Nevertheless, systematic attempts to understand the relationship between obesity and an acute worsening of kidney function have not been thoroughly performed in patients undergoing CABG. In the present cohort of Korean patients who underwent CABG, patients in the overweight groups (BMI > 23.5 kg/m2) showed a higher risk of post-surgical AKI, but these patients had a more favorable prognosis in terms of overall mortality. Although several mechanisms possibly underlie the observations, the relationship of obesity with AKI or mortality might depend on its clinical or subclinical features, such as inflammation or nutritional support.
The effects of obesity on post-surgical AKI have been explored in diverse clinical settings. According to a study that was based on patients with acute respiratory distress, obesity was highly associated with the development of AKI, but these patients had decreased mortality in the intensive care unit and more ventilator-free days.29 In another study of 14,986 intensive care unit patients, each 5 kg/m2 increment in BMI was associated with a 10% higher risk of AKI. With respect to in-hospital deaths, an increased BMI was associated with a decreasing trend of the OR.27 In elderly patients undergoing hip fracture surgery, obese patients were at an increased risk of AKI, but overweight and obesity were not observed to be associated with an increased risk of mortality compared to normal-weight patients.30 Notably, the relationships of BMI with AKI or mortality were similar to the present findings.
Some possible mechanisms of CSA-AKI include renal ischemia, reperfusion injury, oxidative stress, and inflammation.2 Obesity increases the levels of oxidative stress, endothelial dysfunction, and inflammation, although the effect of obesity in the setting of cardiac surgery has not been directly addressed.31 The current observations could be also explained by the effects of adiponectin. In addition to the fact that adiponectin regulates glucose and lipid metabolism, it was reported to confer protection against AKI in a renal ischemia reperfusion injury model.32 Additionally, it reduces renal inflammation and fibrosis by activating adenosine monophosphate protein kinase pathways, thus preventing albuminuria.233 However, the blood adiponectin level is lower in obese subjects than in their counterpart subjects,33 which may increase the risk of AKI in obese patients after CABG.
There is a paradoxical decrease in morbidity and mortality with an increase in BMI.13 A previous study on patients after cardiac surgery reported a protective effect of obesity in terms of hospital survival,15 although this trend was reduced in critically ill patients with AKI.27 Other studies have rebutted this paradox based on the fact that BMI does not completely reflect fat mass,3435 and obese people might be more aggressively treated with disease-modifying agents than their normal-weight counterparts.1436 Theoretically, the favorable survival of obese patients could be attributed to their high metabolic reserves.13 Because obese patients have a potential reservoir to secrete amino acids and adipokines, particularly in stressful conditions, this milieu would decrease the levels of B-type natriuretic peptide, oxidative stress, and inflammation.13 Obese patients receive sufficient nutritional support3738 after surgery, which may overwhelm the deleterious effects of obesity. The obese patients in this study were generally younger and had higher hemoglobin and albumin levels, which might reflect the ample nutritional status compared with the underweight patients. Nevertheless, obesity should be considered potentially harmful if patients maintain a nutritionally balanced diet.
Being underweight is directly and indirectly associated with high mortality.3940 The reason for the high mortality rate in the underweight group could be explained by a lower metabolic reserve and nutritional support in stressful situations. Even underweight patients had higher mortality than their obese counterparts, partly because they were older and had greater severity of certain illnesses.29
This study has some limitations. Firstly, because this study was based on Korean (i.e., Asian) patients, generalizing the study findings to Caucasian patients may be limited.12 Secondly, imbalanced baseline characteristics between groups could affect the statistical results (e.g., the longer hospitalization period and older age in underweight group could reflect the severity of medical status). Thirdly, as the study was retrospective, we could only obtain the information regarding whether or not the patients died or not, but the causes of mortality could not be determined. Furthermore, obesity was measured using BMI alone, and body compositions were not considered.
Obesity was related to a high risk of AKI, but not high mortality, whereas being underweight was associated with poor survival after CABG. These results suggest that obesity or BMI can be used to predict the outcomes of CABG and will form the basis of future studies regarding the underlying relationships between obesity and heart and kidney function.
 XML Download
XML Download