

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic hepatitis B virus (HBV) infection remains one of the most significant burdens to health worldwide.12 Despite effective vaccination programs, chronic hepatitis B (CHB) may develop perinatally or during the first year of life. Pediatric HBV infection is typically asymptomatic in childhood. However, these patients have a high risk of chronicity and may develop severe long-term complications such as liver cirrhosis or hepatocellular carcinoma (HCC).1345 For these reasons, treatment of CHB in children and adolescents is important. Nonetheless, treatment of this patient population remains controversial due to the risk of resistance and undesirable effects while in an immune-tolerant state.26789
The goal of pediatric CHB treatment is to prevent liver cirrhosis, liver failure, and HCC. The Food and Drug Administration has approved drugs for the treatment of HBV in children including interferon-α (IFN-α), lamivudine (LAM), adefovir, entecavir (ETV), and tenofovir.29 However, each of these medications for pediatric CHB has several limitations. For instance, IFN-α is costly, requires injections and causes frequent side effects.29 LAM is an oral pyrimidine nucleoside analog that suppresses HBV replication by inhibiting viral reverse transcriptase; this drug improves liver histology and liver enzyme normalization but also carries a high risk of drug resistance.691011 Furthermore, adefovir is no more effective than placebo in children aged 2–11 years and is associated with a high rate of resistance.912 Tenofovir shows few side effects but is not approved for children under 12 years of age.9 ETV is a potent, safe nucleoside analog that has demonstrated superiority to LAM in hepatitis B e antigen (HBeAg)-positive CHB adult patients in terms of the rates of histologic, virologic and biochemical improvement.13 In children, Jonas et al.14 reported superior antiviral outcomes of ETV treatment compared with placebo with a favorable safety profile. Several studies have shown similar results in pediatric CHB,111415161718 although no reports have compared ETV and LAM in children.
The aim of this study was to compare the long-term efficacy of ETV and LAM therapy in children with CHB who had not received nucleoside analogue treatment.
Go to : 
METHODS
We performed a retrospective non-concurrent comparative study including ETV-treated and LAM-treated pediatric CHB patients as historical control who were naïve to nucleos(t)ides. We included pediatric CHB patients, most of whom acquired HBV infection perinatally or during early childhood, who received treatment for at least 12 months from the Department of Pediatrics, Seoul National University Hospital, Seoul National University Bundang Hospital, Kyungpook National University Hospital, and University of Ulsan University Asan Medical Center. These patients underwent long-term follow up at each clinics. The median follow-up duration was 51 months in the ETV group.
Patients were excluded from the present study if they had concomitant infection with hepatitis C, hepatitis D or the human immunodeficiency virus or had decompensated liver disease or other chronic liver disease. Patients older than 20 years at the time of treatment or who received liver transplantation were also excluded from this study.
All patients were seen every 1 to 3 months. The importance of compliance was emphasized before and during the course of therapy. At each visit, the patients underwent clinical evaluation and biochemical testing, such as alanine aminotransferase (ALT) measurement and HBV serologic examination, including hepatitis B surface antigen (HBsAg), anti-HBe and virologic assessment (HBV DNA titer). We performed retrospective chart reviews with respect to biochemical and virologic responses and adverse events. HBeAg seroconversion was checked in patients who were HBeAg-positive at baseline.
Virologic suppression was defined as HBV DNA at undetectable levels assessed using real-time polymerase chain reaction (< 20 IU/mL) as well as ALT normalization, defined as ALT activity < 40 IU/L. Virological breakthrough was defined as either a > 10-fold increase in HBV DNA titer from the nadir for detectable HBV DNA or HBV DNA > 200 IU/mL after virologic suppression.16
The results were presented as medians with ranges and relative frequencies. The differences between categorical variables were calculated using the χ2 test and Fisher's exact test. Continuous variables were tested using the Mann-Whitney U test. The Kaplan-Meier method was used to assess the cumulative rates of virological suppression, HBeAg seroconversion, virologic breakthrough and genotypic mutation. The difference of cumulative rates between two groups was calculated using the log-rank test. To evaluate the factors associated with HBeAg seroconversion, loss of HBeAg, virologic suppression and ALT normalization, we used a logistic regression model with a logit link. Initial HBeAg status, HBV titer, ALT level, sex, treatment duration and age at initiation of treatment were included in the model as covariates. The results were considered statistically significant if the P value was less than 0.05. We used the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) for statistical analyses.
Ethics statement
The Seoul National University Hospital, Kyungpook National University Hospital, Seoul National University Bundang Hospital, and Asan Medical Center Children's Hospital Institutional Review Boards; approved this study (IRB No. 1612-069-81, 2017-10-003, B-1702-382-103, and 2017-1201). Informed consent was waived by the board.
Go to :
RESULTS
The baseline characteristics of the ETV (n = 15) and LAM (n = 23) groups are compared in Table 1. The median treatment duration was 51 months (range, 17–81) in the ETV group and 37 months (14–75) in the LAM group. There were 33 patients who were initially HBeAg (+) in this study (13 in the ETV group, 20 in the LAM group).
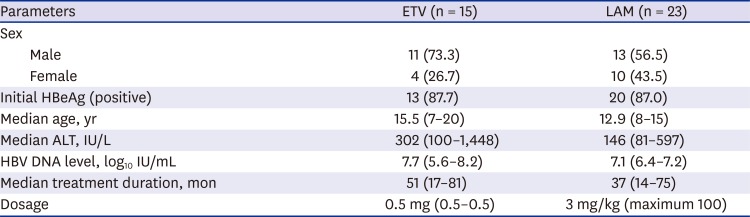
Table 1
Baseline characteristics of the ETV- and LAM-treated groups
Values are presented as number of patients (%) or median (range).
ETV = entecavir, LAM = lamivudine, HBeAg = hepatitis B e antigen, ALT = alanine aminotransferase.
![]()
Eight of 15 patients (53.3%) and 11 of 14 patients (78.6%) showed virologic suppression after 1- and 2-year of ETV treatment, in contrast to 0 and 3 (17.4%) of 23 LAM-treated patients. This difference was statistically significant (P < 0.001, Table 2). However, there were no significant differences between the groups in terms of the rates of HBV DNA > 2 log10 IU/mL decrement, ALT normalization and HBeAg seroconversion after 1- and 2-year of treatment. ALT normalization was achieved in 14 patients (93.3%) of the ETV group and 23 patients (100.0%) of the LAM group (P = 0.395) after 1-year of treatment.

Table 2
Biochemical, serologic and virologic responses after 1- and 2-year of treatment
Values are presented as number of patients (%).
ETV = entecavir, LAM = lamivudine, ALT = alanine aminotransferase, HBeAg = hepatitis B e antigen.
aDNA < 20 IU/mL.
![]()
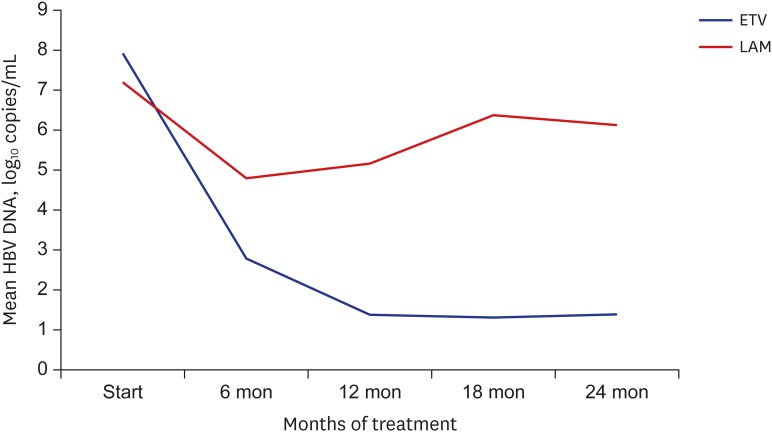
The rates of virologic suppression after 3 and 6 months of treatment were similarly low in both groups (6.7% and 0%, respectively). However, after 12 months of treatment, the virologic suppression rate increased to 53.3% in the ETV group. The mean HBV DNA level reduction at 24 months was also greater in the ETV group (6.5 log copies per milliliter) than in the LAM group (1.0 log copies per milliliter) (Fig. 1).
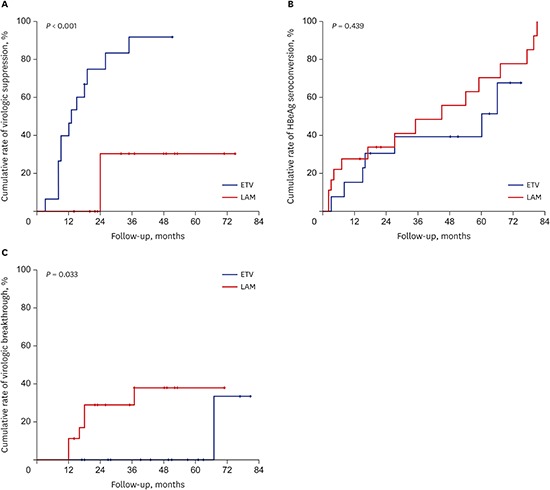
The final cumulative rates of virologic suppression were 75% at 2 years and 91.7% at 3 years for ETV treatment compared to 30.8% at 2 years of LAM treatment, resulting in a significantly higher cumulative rate of virologic suppression in the ETV group versus the LAM group (P < 0.001, Fig. 2A).
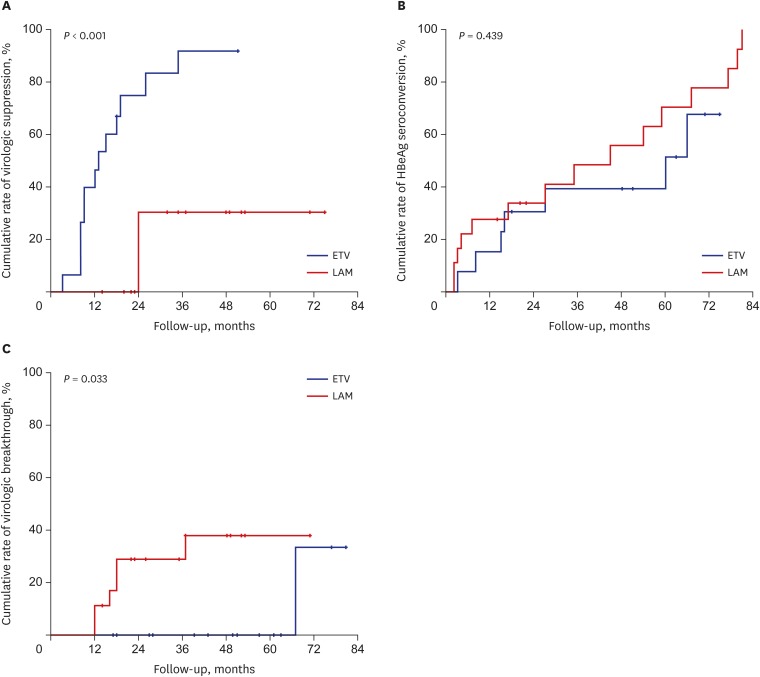 | Fig. 2Cumulative rates of virologic suppression, HBeAg seroconversion, virologic breakthrough, and genotypic mutation. (A) The cumulative virologic suppression rate is statistically higher in the ETV group compared to the LAM group (P < 0.001). (B) The cumulative HBeAg seroconversion rates are not significantly different between the ETV group and the LAM group (P = 0.439). (C) The cumulative virologic breakthrough rate is significantly higher in the LAM group than that in the ETV group (P = 0.033).
HBeAg = hepatitis B e antigen, ETV = entecavir, LAM = lamivudine.
|
The rates of > 2 log10 IU/mL decrement in HBV DNA titers at 3 and 6 months of therapy were 93.3% and 91.3% in both groups (P = 0.299). However, after 12 months of treatment, the rate of > 2 log10 IU/mL HBV DNA titer decrement fell to 82.6% in the LAM group versus 100% in the ETV group.
The mean duration of treatment before virologic suppression was significantly shorter in the ETV group (14.1 months) versus the LAM group (24 months) (P = 0.040). HBeAg seroconversion occurred at 27.9 months (3–66) in the ETV group vs. 37.3 months (2–81) in the LAM group (P = 0.647). Mean virologic breakthrough occurred at 51 months in the ETV group vs. 18.8 months (12–37) in the LAM group (P = 0.127).
The cumulative HBeAg seroconversion rates were 30.8%, 39.4%, and 51.5% at 2, 3, and 5 years for the ETV group in contrast to 33.8%, 48.5%, and 70.6% for the LAM group, respectively. The cumulative HBeAg seroconversion rate was not significantly different between the two groups (P = 0.439, Fig. 2B).
Virologic breakthrough developed in one patient (6.7%) after 67 months in the ETV group. This patient also developed a genotypic mutation. In the LAM group, 6 of 23 patients (26.1%) developed virologic breakthrough after 12 to 37 months of treatment. The LAM group showed a higher cumulative rate of virological breakthrough than the ETV group, and this difference was statistically significant (P = 0.033, Fig. 2C). The final cumulative rates of virologic breakthrough were 33.3% for the ETV group at 6 years compared with 11.1% at 1 year and 37.8% at 4 years for the LAM group.
A genotypic mutation was found in one patient (6.7%) after 67 months of ETV treatment and 11 patients (47.8%) after 14 to 53 months of LAM treatment. One patient in the ETV group had a genotypic mutation at positions rt169, rt184, rt202, rt204, and rt250. Eleven patients in the LAM group had rtM204I or rtM204V mutations with/without an rtL180M mutation. The patient who developed an ETV mutation was changed from ETV to tenofovir therapy. The cumulative genotypic mutation rate was significantly higher in the LAM group compared with the ETV group (P = 0.011).
We next examined the factors thought to be associated with HBeAg seroconversion, loss of HBeAg, virologic suppression and ALT normalization during ETV treatment using a logistic regression model with a logit link. However, no important factors influencing the results were identified. ETV and LAM treatments were tolerated well. No severe adverse effects associated with either drug occurred during the treatment.
Go to :
DISCUSSION
This is the first real-life multicenter study comparing the long-term antiviral efficacy of ETV monotherapy and LAM monotherapy in children with nucleoside-naïve CHB. ETV is a recently approved drug to treat pediatric CHB and has shown potent antiviral effects, low drug resistance and tolerable side effects.1114151617 In an adult study, Chang et al.13 reported the superiority of ETV to LAM in HBeAg-positive CHB, with histologic and HBV DNA level improvement and ALT normalization at 48 weeks. Another adult study comparing ETV vs. LAM therapy for naïve patients with spontaneously reactivated CHB presenting as acute-on-chronic liver failure showed that ETV significantly reduced HBV DNA titers, improved Child-Turcotte-Pugh and model for end-stage liver disease scores and extended long-term survival rates.6
In our study, there was a significant difference in cumulate virologic suppression rates between the ETV and LAM groups throughout the study period. These results were similar to a previous adult study, which showed that 48-week ALT normalization and virologic suppression rates were higher in the ETV group than in the LAM group.13
We also found the treatment duration before virologic suppression was shorter in the ETV group than in the LAM group, similar to the result of another adult study showing that more than 90% of patients achieved virologic suppression after 2 years of ETV treatment.19 These findings confirm that ETV is a potent antiviral agent.
We reported no differences in cumulative HBeAg seroconversion rates between the ETV and LAM groups. Chang et al.15 also reported that the cumulative HBeAg seroconversion rates were similar between their ETV-treated group and untreated control pediatric CHB patients. Similarly, in an adult study, no significant difference was reported in HBeAg seroconversion rates between ETV- vs. LAM-treated patients.13
In our study, the cumulative seroconversion rate of the ETV group in the first year (15.4%) was similar to those reported in other studies, including 24.4% in pediatric patients and 15.9 to 20% in adults.131419 We also reported that the seroconversion rates increased in the second year to 30.8% and 51.5% in the fifth year, which is supported by another study reporting rates of 44.3% at 2 years and 55.4% at 4 years.16
The major limitation of LAM treatment is the need for prolonged treatment, which leads to higher resistance rates.69101120 In a pediatric multicenter trial, 19% of children undergoing 52 weeks of LAM therapy developed codon changes in the YMDD (tyrosine-methionine-aspartate-aspartate) motif of the HBV polymerase gene.21 In contrast, ETV exhibited lower resistance rates in a pediatric clinical trial (0.6% at 1 year of treatment and 2.6% at 2 years of treatment).14 In our study, the cumulative virologic breakthrough and genotypic mutation rates were significantly higher in the LAM group than in the ETV group, similar to previous studies.291016 The cumulative virologic breakthrough rate was 33.3% at 6 years of ETV treatment, less than the 37.8% rate at 4 years of LAM treatment. We reported only one patient who developed genotyping resistance in the ETV group after 67 months, while 47.8% of patients in the LAM group developed resistance after 14 to 53 months.
Similar to other reports and clinical trials that have suggested that ETV is well tolerated.14151617 We reported no severe adverse effects associated with ETV.
This was a small, nonrandomized, retrospective study. However, this study included young patients under 16 years of age, and our treatment duration was relatively longer than that in other studies, with a median ETV treatment duration of 4.3 years and follow-up duration of 5.1 years.13141516
In conclusion, our results indicate that ETV is superior to LAM in pediatric CHB treatment because of its higher virologic suppression rate and shorter time to virologic suppression as well as lower cumulative rates of virologic breakthrough and genotypic mutation.
Go to :
 XML Download
XML Download