

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Recent advances in the highly-active antiretroviral treatment (HAART) have transformed the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) into a manageable chronic disease.1 There had been a relatively slow progression in the prevention of HIV/AIDS, although high-risk individuals were urged to abstain from sex and use condoms, in addition to being given treatment for prevention of the infection in pregnant women2 until more advanced interventions were introduced. However, remarkable progress has been observed in recent years in the prevention of HIV infections.3
A tenofovir disoproxil fumarate and emtricitabine (TDF/FTC) co-formulate was first approved for use as pre-exposure prophylaxis (PrEP) for adults by the US Food and Drug Administration in 2012.4 The efficacy of PrEP with daily oral TDF/FTC therapy for the prevention of HIV infection has been proven in randomized, placebo-controlled trials.567 In 2014, the US Centers for Disease Control and Prevention (CDC) recommended that PrEP should be offered to people at a high-risk of HIV infection,8 and in 2016, the World Health Organization (WHO) recommended PrEP to people at a substantial risk of HIV infections.2
Studies have reported the attitudes, awareness, or willingness of high-risk people and medical personnel (MP) in some countries.91011 However, there has been no study investigating the awareness, knowledge, interest, and willingness of PrEP among high-risk people or even MP in Korea, despite the increasing number of newly-diagnosed HIV/AIDS cases in Korea.12 Therefore, this study was conducted to investigate the level of awareness among high-risk people, including men who have a sex with men (MSM) and among MP in Korea through a cross-sectional online and offline survey, to identify possible obstacles that hinder the access of MSM and MP to PrEP, and to improve the access of such individuals to PrEP for prevention of HIV infections.
METHODS
Survey
Between August 2016 and November 2016, the first questionnaire survey was sent to MSM from the internet community (www.love4one.com) through a Google survey and other social media. Simultaneously, randomly selected people and MP (physicians and nurses) completed the offline survey with the same questionnaire. To compare the changes in the attitudes and knowledge of MSM, the second questionnaire survey was conducted in August 2017, with same questions as that in the first. To ensure protection of personal identity, all surveys were conducted anonymously. A total of 499 people responded to the survey in 2016, and 123 MSM responded in 2017 (Fig. 1).
 | Fig. 1The distribution of respondents in this study.
MSM2016 = men who have sex with men who responded to the survey in 2016, MSM2017 = men who have sex with men who responded to the survey in 2017, MP = medical personnel, HIV2016 = human immunodeficiency virus-positive respondents in 2016, HIV2017 = human immunodeficiency virus-positive respondents in 2017.
|
Measures and questionnaires
The respondents' sociodemographic information included sex, age, status of HIV infection, final education level, and monthly income of the family. The questionnaires asked about respondents' experience related to HIV testing, whether they were aware of or had been given a prescription for PrEP, whether they felt the need of taking PrEP, and whether they would use PrEP in the future. In addition, the questionnaires asked regarding the most common obstacles in approaching PrEP.
Statistical analysis
We assessed bivariate associations of respondents' sociodemographic characteristics and experience in HIV/AIDS care, along with their knowledge of PrEP and responses to the various questions on PrEP in the questionnaires. Statistical differences were assessed by the χ2 test for categorical variables and the Mann-Whitney U test for continuous variables. All statistical analyses were performed using the R statistics version 3.4.1. for Windows® (R Foundation, Vienna, Austria; http://www.R-project.org).
RESULTS
Study population
To obtain as many responses as possible, the surveys were distributed to not only MSM but also the non-specific general population and MP, such as physicians and nurses, working in various hospitals, through social media, e-mails, or offline papers. Therefore, we were unable to estimate the exact percentage of people responding to our survey. From a total of 499 respondents in 2016, 266 respondents were MSM and 107 were MP. The number of people who did not belong to the MP or high-risk HIV groups was 126 (Fig. 1). More than half of MSM responded that they were HIV positive, 55.3% in 2016 and 50.4% in 2017 (Fig. 1).
The sociodemographic findings of respondents
The median age and sex distribution of respondents among MSM, MP, and the general population are shown in Table 1. Among MSM, 77.4% answered that their last academic records were at least at the university level. There was no noticeable difference in the final education levels between HIV-positive and HIV-negative MSM. Responses regarding the monthly income of families are shown in Table 1. A small number of MSM answered that their monthly income was above 3 million KRW (equivalent to approximately 3,000 USD) (Table 1).
Table 1
The socioeconomic characteristics of all respondents in the survey in 2016 and 2017

Data are shown as number (%).
MSM2016 = men who have sex with men who responded to the survey in 2016, MSM2017 = men who have sex with men who responded to the survey in 2017; HIV = human immunodeficiency virus, MP = medical personnel, IQR = interquartile range.
![]()
The awareness and willingness regarding HIV and PrEP
Among HIV-negative MSM, 63% (in 2016) and 55.7% (in 2017) people responded they had taken an HIV test once a year. In contrast, among MP and the general population, only 24 (22.4%) and 23 (18.3%) people had taken an HIV test in each group (Table 1). The percentage of awareness in each group is shown in Fig. 2. Among MSM, 61.3% (2016) and 88.6% (2017) people were aware of the use of PrEP, whereas among the general population, only 7.9% were aware of the use of PrEP; among MP, only 23.4% respondents were aware of the use of PrEP (Fig. 2A). Positive response rates to questions on the respondents' use of PrEP (in the MSM and the general population or given to their clinic's visitors in the case of MP) were low: 3.4% in MSM in 2016, 5.7% in MSM in 2017, 1.9% in MP, and none in the general population (Fig. 2A). When asked whether PrEP was considered to be necessary, 88% (2016) and 95.1% (2017) MSM and 81.7% of the general population answered “yes”; however, among MP, only 68.2% people answered “yes” (Fig. 2B).
 | Fig. 2Response for PrEP. (A) The awareness and experience regarding PrEP for HIV infections among all respondents. (B) Proportion of the respondents who answered that PrEP was necessary.
PrEP = pre-exposure prophylaxis, HIV = human immunodeficiency virus, MSM2016 = men who have sex with men who responded to the survey in 2016, MSM2017 = men who have sex with men who responded to the survey in 2017, MP = medical personnel.
|
When MSM were asked whether they would use PrEP in the future, 54.9% answered “yes,” but 43.2% in 2016 and 65% in 2017 answered they would use PrEP if medical insurance covered the cost of the treatment (Fig. 3).
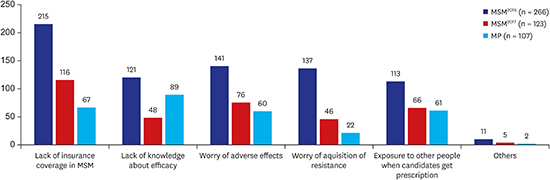
The perception for the possible obstacles to PrEP
Regarding the question on what were considered as the most common obstacles in approaching PrEP, the lack of insurance coverage was the most common answer among MSM (29% in 2016 and 32% in 2017); however, the lack of knowledge regarding the efficacy of PrEP (30%) was the common answer among MP (Fig. 4). MSM were mainly concerned about the possible adverse effects of the drugs administered during treatment (19% in 2016 and 21% in 2017), and emergence of antiviral drug resistance during PrEP (19% in 2016 and 13% in 2017). MP were concerned about the efficacy of PrEP (30%), high costs due to the lack of insurance coverage for PrEP (22%), and unwanted exposure of the spouses or partners of their patients to HIV infections (20%) (Fig. 4). The distribution of this response was significantly different between MSM and MP (MSM2016 or MSM2017 vs. MP; P < 0.001). However, there was no difference between MSM2016 and MSM2017 (P = 0.110).

DISCUSSION
To the best of our knowledge, this study was the first to investigate the trends in the awareness and acceptance of PrEP for preventing HIV infection among a high-risk population, such as MSM and MP as medical care providers, compared with those among the general population in the Republic of Korea through comprehensive questionnaires. Because MSM belong to a high-risk population for HIV infection, more than half of these individuals (61.3%) are aware of PrEP. However, MP who administer PrEP to prevent the spread of HIV infection had less knowledge regarding PrEP (23.4%). Moreover, because of obstacles such as no introduction of PrEP, no coverage by healthcare insurance, inadequate knowledge and awareness regarding PrEP among MSM and MP, concern regarding the possible adverse effects and emergence of resistance to antiretroviral drugs during PrEP, the frequency of PrEP experience among MSM and MP in this survey was low (3.4% in MSM2016, 5.7% in MSM2017 and 1.9% in MP as shown in Fig. 2A).
Recent studies have reported the awareness, interest, and attitudes toward HIV PrEP among specific populations.91011 Because the efficacy of PrEP for the prevention of HIV infection has been proven in randomized, placebo-controlled trials,567 in 2014, the US CDC recommended that PrEP should be offered to people at a high risk of HIV infection,8 and in 2016, the WHO recommended PrEP to people at a substantial risk of HIV infections.2 An Australian study aimed to determine the awareness and knowledge of HIV PrEP among MSM and bisexual men, and found that 77% (954/1,251 participants) of these men were aware of PrEP, and better knowledge was independently associated with living in a capital city, having a university degree, having full-time employment, being HIV-positive, and use of post-exposure prophylaxis or PrEP.9 In this study, the frequency of awareness among high-risk men was much higher than the frequency of those in our study (61.3%). Another study conducted among young transwomen (YTW) in San Francisco found that 42.7% of 67 YTW had heard of PrEP.11 The authors of this study described that, MSM had been the primary target of interventions to promote PrEP in San Francisco; therefore, MSM might have had more chances to have access to and understand the information regarding PrEP than high-risk women. High-risk women were not included in our study. In Korea, women may have disadvantages in accessing information on PrEP, such as the study of YTW. Further studies aimed at high-risk women should be conducted in Korea.
The study on attitudes toward HIV PrEP in urban populations in clinics in the US reported that men were more likely to express openness to learn about possible treatments (61.4% of men, 54.8% of women, P < 0.001). The main reason for this was the fear of HIV, and disinterest in learning about new treatments was attributed to lack of recognition of the risk of infection.10 In contrast, our study showed that the percentage of respondents among the general population who were thought to have required HIV PrEP was very low (20.6%).
One of the serious findings of our study that would require urgent action by the academic society or policymakers was the low frequency (23.4%) of awareness of HIV PrEP. Several studies reported on the perceptions of MP and the accuracy of their knowledge or attitudes toward HIV PrEP.131415 In the study investigating the healthcare provider's knowledge, perception, and willingness toward HIV PrEP in southern US, knowledge regarding PrEP was higher among physicians than among non-physicians, and higher among nonpublic healthcare providers than among public healthcare providers.13 A national survey targeting family-planning providers in the US reported that among potential prescribers, 38% accurately defined PrEP (95% confidence interval [CI], 32.5–42.8) and 37% accurately stated the efficacy of PrEP (95% CI, 32.0–42.4).14 These two studies did not exactly describe how many respondents had prior knowledge regarding HIV PrEP, but only evaluated the accuracy of the knowledge of MP as a score. Therefore, a direct comparison of the rate of awareness of PrEP with our study was impossible. However, low awareness of MP in our country could be expected sufficiently from this study result. Therefore, efforts for the implementation of HIV PrEP among MP as the well-proven way to slow the increase of HIV infections in Korea should be discussed and managed among associated academic societies and policymakers. In the previous study,13 the willingness to prescribe PrEP was more likely in the case of higher PrEP knowledge scores (adjusted odds ratio, 14.94; 95% CI, 3.21–69.61); therefore, educating MP regarding PrEP may be an important step in decreasing new cases of HIV infection.
The majority of healthcare providers were concerned about the safety, efficacy, and cost of PrEP. The study investigating a healthcare provider's knowledge of PrEP in southern US showed that a high proportion of providers (97%) were in support of more research on the safety and efficacy of PrEP.13 In addition, our results showed that the most common factors that MP worried about were the efficacy, safety, and cost of PrEP due to the lack of insurance coverage for PrEP. There are well-organized studies to prove the efficacy of PrEP for the prevention of HIV infections.56716 Not only US CDC but also the WHO recommended that PrEP should be offered to people at a high-risk of HIV infection28; therefore, although some studies have reported the adverse effects of TDF/FTC used as PrEP,171819 the authors believe that no delay should occur in the implementation of HIV PrEP in Korea.
Approximately one-fifth of MSM and MP who participated to this study were concerned about the possible adverse effects of drugs administered during PrEP. In the study to investigate the effect of PrEP for HIV prevention in MSM, nausea was reported more frequently during the first 4 weeks in the TDF/FTC group compared with the placebo group.5 In the study to investigate the effect of PrEP with TDF/FTC among heterosexuals, the TDF/FTC group had higher rates of nausea, vomiting, and dizziness than the placebo group; however, the rates of serious adverse effects of these drugs were similar.7 Participants, who received TDF/FTC had a significant decline in bone mineral density compared with those who received placebo.7 In the report on renal safety during PrEP in a large integrated healthcare system, discontinuation of PrEP due to renal toxicity was rare.17 In a report on the results of a meta-analysis about the effectiveness and safety of PrEP for all populations, adverse events were shown to be similar between the PrEP and placebo groups.16 Therefore, the benefits from PrEP are more than the possible serious adverse effects, and no reason to postpone the introduction of PrEP has been observed.
Concern regarding the emergence of antiviral resistance was not high in MSM and MP in our study. Some studies investigating the risk of HIV resistance during PrEP showed that antiviral resistance was rare and concern over drug resistance should not be a reason to limit the use of PrEP.202122 However, despite adherence to TDF/FTC-based PrEP, incidents of HIV infection were reported when persons were exposed to the FTC-resistant virus, TDF-resistant virus, or both. Therefore, patients should be consulted regarding the use of PrEP as part of a combination approach to HIV prevention.23
The cost of medication is critical in order to access treatment in the real world. In our study, the lack of insurance coverage for PrEP was the most critical obstacle among MSM (29% in 2016 and 32% in 2017). According to the PrEP study with YTW, a significant number of participants with health insurance were interested in PrEP compared to those with no health insurance (74.5% vs. 25.5%, P = 0.03).11 The study with a large integrated healthcare system reported that no HIV seroconversions occurred during PrEP use; however, two HIV seroconversions occurred in individuals who discontinued PrEP after losing insurance coverage. They emphasized that strategies were needed to increase PrEP access during gaps in insurance coverage.17 To improve access to PrEP to prevent the increase of new HIV infections, establishment of insurance coverage for PrEP was considered to be an important issue in Korea.
US CDC recommended that persons at a high-risk of HIV infection should be annually screened for HIV at least in all healthcare settings.24 However, our study showed that 63% (2016) and 55.7% (2017) HIV-negative MSM (Table 1) took an HIV test once a year. Policymakers and MP in all healthcare settings should offer further information on this and encourage high-risk people in Korea to take HIV tests at least annually.
This study had several limitations. First, the survey response rate was not evaluated. Second, the respondents among MSM could have led to some bias, because MSM who attempted the online survey via e-mails or SMS may have attained a higher educational level and may have had more access to information provided through online medical sites. Therefore, in reality, the percentage of awareness and willingness regarding PrEP may be much lower than the results of this study. Third, no woman in the high-risk group (e.g., serodiscordant spouses or partners of HIV-positive males) was included in this study because we were unable to contact them.
Despite these limitations, this study showed that we need to make every effort to improve the awareness and accessibility of PrEP to prevent HIV infection among not only high-risk populations but also medical staff and policymakers.
 XML Download
XML Download