

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Suicide is a significant public health problem worldwide resulting in loss of lives and societal burden. The suicide rates in South Korea have been recorded as the highest among Organization for Economic Cooperation and Development (OECD) nations since 2003. The overall suicide rate is slightly declining, but the suicide rate of the elderly has risen. The averages were 62.5 per 100,000 persons in their 70's, and 83.7 per 100,000 persons in their 80's. These rates are three times higher than the OECD average in 2016.1 In persons aged 65 and older, suicide methods were hanging (49.5%), carbon monoxide poisoning (16.3%), pesticide poisoning (7.1%), drowning (4.0%), drug intoxication (1.6%), and blunt weapon (0.7%), according to reports of the Korea Statistics Office.2 Suicidal death in the elderly by drug intoxication was 1.6%, but the rate of drug-related suicide attempts may be higher. The emergency department (ED) is an important entry of drug-related suicide attempt patients.3
In this study, we compared different of types of drugs ingested for suicide attempts by age group, as well as the frequency with which they were ingested. Through this study, it can be helpful to identify the type of drugs in elderly suicide attempters and to assist suicide prevention for the elderly.
METHODS
Patients and data collection
This study was conducted at two teaching hospitals; tertiary medical centers in Korea. We retrospectively reviewed the medical charts and drug intoxication records collected according to ED protocols. Between 1 May 2015 and 30 April 2017, 481 patients were admitted to ED for suicide attempt by overdosing with pills. We excluded 48 patients who co-ingested pesticides, corrosive agents, unknown drugs or pills belonging to another person and who were transferred to other hospitals. All patients or their guardians provided informed consent prior to the collection of information; according to drug intoxication collecting protocols in the department of emergency medicine.
All senior residents and board physicians in emergency medicine were informed about the protocols, as they collected the data in the ED. We analyzed data on the following variables: demographic factors (sex and age of patients, whether the patients had an underlying disease, and whether the patients had a psychiatric disease); history of intoxication (ingredients of pills used for overdose, amount ingested, and suicidal intention); and clinical manifestation (systolic and diastolic blood pressure, body temperature, and heart rate and Glasgow coma scale).
Drugs were categorized according to the indication for which they were approved, rather than by pharmacological class. Five categories were used: 1) antidepressants, including tricyclics, selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and novel antidepressants; 2) hypnotics, including benzodiazepine and non-benzodiazepine sleep medications; 3) analgesics, including narcotics and non-narcotics, aspirin, acetaminophen, and nonsteroidal anti-inflammatory agents; 4) over-the-counter (OTC) medications, such as sleeping agents, including sleep inducers and doxylamines; and 5) others, such as herbs, hypertensive medications, diabetes medications, and other drugs for a patient's own condition.
Statistical analysis
Categorical variables were analyzed with the χ2 test. And Student's t test was used for continuous variables. A P value of under 0.05 was considered statistically significant. The statistics program used for this research was SPSS for Windows (ver. 18.0; SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 433 individuals were enrolled in this study (Table 1).
Table 1
Demographic and clinical characteristics of patients who attempted suicide by ingesting drugs
Demographic and clinical characteristics of patients who attempted suicide by ingesting drugs
Patients were grouped into two age categories: “non-elderly” (younger than 65 years of age) and “elderly” (65 years of age and older).
The non-elderly group included 77 male patients (22.3%) and 268 female patients (77.7%), while the elderly group included 32 male patients (36.4%) and 56 female patients (63.6%). There was a significant difference in the sex ratio between the two groups (P = 0.010).
There was a significantly higher share of patients with psychiatric diseases in the non-elderly age group compared to in the elderly group (P < 0.001). In total, 146 patients had been diagnosed with depression, including 126 non-elderly patients and 20 elderly patients (P = 0.021). There were significant differences in systolic blood pressure (P = 0.010), Glasgow coma scale (P < 0.001), and underlying diseases (diabetes, hypertension, and cardiovascular accident) (P < 0.001). There were no significant differences between the two groups regarding diastolic blood pressure (P = 0.856) and body temperature (P = 0.334; Table 1).
Relationship between drug poisoning and age group
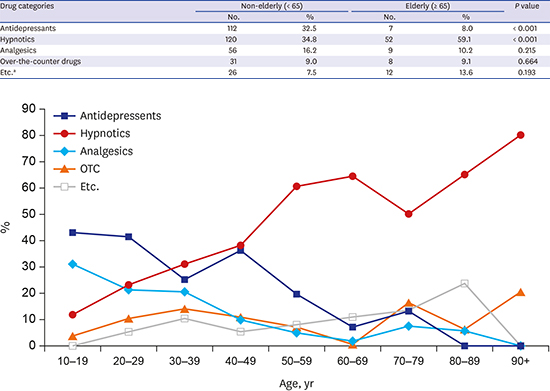
There was a statistically significant difference between the category of drugs ingested in the non-elderly group and the elderly group (P < 0.001). Patients who overdosed on antidepressants accounted for 112 (32.5%) in the non-elderly group and 7 (8.0%) in the elderly group. There was a statistically significant difference between the two groups (P < 0.001).
Among the elderly, the most commonly ingested agent was hypnotics 52 (59.1%), and a statistically significant difference was found (P < 0.001). OTCs and other medications showed similar usage in both age groups, with no significant difference found (P = 0.664, P = 0.193).
The number of patients who had been diagnosed with depression was 126 in the non-elderly age group and 20 in the elderly age group. In patients with depression, 65 (51.6%) of non-elderly patients and 3 (15%) of elderly patients had ingested antidepressants (P = 0.005). There are differences in ingested drugs for suicide attempt between non-elderly and elderly groups on a decade basis (Fig. 1 and Table 2)
Fig. 1
Differences in ingested drugs for suicide attempt between non-elderly and elderly groups on a decade basis.
OTC = over-the-counter drugs.
Etc. = herbs, hypertension medication, diabetes medication, or other drugs for own disease.


Results of patients who ingested drugs to attempt suicide
A higher hospital admission rate was found for the elderly group (36%) compared to the non-elderly group (20%), and a statistically significant difference was found (P = 0.020). The duration of hospital stay of admitted patients was 3.70 ± 2.51 days for the elderly group and 2.98 ± 1.89 days for the non-elderly group (Table 3).

DISCUSSION
Suicide is currently the fourth leading cause of death in Korea, which has had the highest rate among OECD countries during the past 10 years.4 Life expectancy continues to increase globally; in 2015, the average global life expectancy was 71.4 years; 73.8 years for females and 69.1 years for males.1 Longer life expectancy is partly due to a decline in mortality resulting from advances in rehabilitative medicine and healthcare coverage and effectiveness,5 which also reduces impairment in functioning and disability over the life course.6 Nevertheless, high suicide rates among the elderly indicate that suicide is a major public health concern and that further suicide prevention efforts are needed.7
Studies show that, in many countries, suicide rates among the elderly are higher than or as high as those of young people.8 However, suicide in the elderly is a much-neglected area. In fact, there is a lack of basic knowledge about elderly suicide among clinicians.9 Geriatric suicide attempts remain an area of great concern.
Ingestion of medications is the most common reason (90%) for which suicide victims visit the ED. As studies suggest, the most common reason for ingesting drugs is intentional suicide, accounting for over 70% of such cases.1011 Therefore, it is necessary to evaluate intention in drug overdoses and classify the medications ingested by patients. And many types of drugs are linked to suicide attempts, such as antidepressants, analgesics, and sedative-hypnotic medications. In this study, drugs ingested for drug-related suicide attempts were classified according to different age subgroups. The proportion of patients who overdosed on antidepressants was 32.5% in the non-elderly age group and 8.0% in the elderly age group. The most commonly ingested agent in the elderly age group was hypnotics (59.1%). Those who attempt drug-related suicide often ingest drugs that were prescribed for them. There is a high probability that patients have an underlying disease, particularly a psychiatric disease.
It has been widely reported that many diseases increase the risk of suicide in the elderly. In the study of geriatric suicide, a statistically significant relationship has been found to exist between medical and psychiatric diseases and geriatric suicides.12 In this study, there were significantly higher underlying diseases in the elderly; diabetes, hypertension, chronic heart failure, and cerebrovascular accidents. Patients with late-life-onset depression are heterogeneous in terms of clinical history and coexisting medical conditions. Compared with older adults reporting an initial depressive episode early in life, those with late-onset depression are more likely to have neurologic abnormalities, including deficits on neuropsychological tests, and age-related changes on neuroimaging that are greater than normal. They are also at higher risk of subsequent dementia.13 Such observations informed the hypothesis that vascular disease may contribute to depression in some older adults.1415 Thus, this group is prescribed hypnotics rather than antidepressants in non-psychiatric clinics in order to alleviate their symptoms.
Irritability, anxiety, and somatic symptoms may be more common in elderly patients with depression.16 Depression and depressive symptoms have been identified as a growing public health concern for older adults in the United States. The estimated overall prevalence of depression among the elderly ranges from 10% to 20%.17 Depression in older adults is common, disabling and accompanied by high levels of medical morbidity and disability.16 Beyond personal suffering, depression is associated with a wide range of negative outcomes, including cognitive decline and dementia, increased family caregiving burden, poor medical outcomes, risk of suicide and high mortality.14 Depression clearly requires treatment. Antidepressants reduce the risk of suicide attempts and deaths by 20%.18 Unfortunately, however, depression is often unrecognized, and even when diagnosed, depression in the elderly is often untreated or undertreated.19 The most serious result of depression in the elderly is suicide.20 The risk of suicide ideation in the elderly is higher than the younger population.21 All depressants are known to have a protective effect against suicidal tendencies or suicidal behavior in the elderly.22 But too many doctors are frightened and refuse to prescribe antidepressants. And patients and guardians may be reluctant to go to the psychiatric department. In this study, suicide attempts among elderly patients who did not receive psychiatric treatment were significantly higher than non-elderly patients. This may suggest a failure to diagnose depression in the elderly or that patients require more psychiatric treatment. Non-psychiatric physicians who prescribe hypnotics to the elderly must consider their depressive moods.
In the United States, the most common toxic substances ingested for suicide are analgesics (11.5%), followed by cosmetics/personal care products (7.7%), household cleaning substances (7.6%), and sedatives/hypnotics/antipsychotics (5.9%); however, the frequency of toxicity from sedatives is rapidly increasing.23 In Korea, there is an effort to supplement the poisoning information database,24 in addition, toxicology and addiction management systems and programs should be established. According to data from the Korean Health Insurance Review and Assessment Service, 9% of elderly individuals are taking antidepressants and 30% are taking hypnotics. Comparing the amount per patient in both groups, the rate was similar for antidepressants but doubled for hypnotics prescribed to the elderly.25 A large amount of hypnotic is prescribed to elderly patients with or without psychiatric assessment.
This study had several limitations. First, it included patients at only two general hospitals. Additionally, several subjects were excluded because not all were confirmed to have attempted suicide. Another limitation was the lack of availability of pharmacy records, accurate drug doses, and correct diagnoses. We were able to obtain medical information by interviewing patients or their guardians; however, that information may have limitations and errors. This issue will be further reviewed using the national insurance data for medicine prescription and ICD diagnosis codes. In the future, information on social status will be collected together with such medical data.
The categories of drugs ingested for suicide attempts vary widely between different age groups. Younger people used antidepressants more frequently in suicide attempts, while the elderly used hypnotics more frequently. And elderly patients required longer hospital stays.
Suicide ideation and depressive mood in older patients who were prescribed hypnotics with various reasons should not be neglected. Further prevention efforts are needed to prevent suicide among the elderly.
 XML Download
XML Download