

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the rapidly growing number of published articles on the subject of social capital and health, social capital at the individual level is significantly associated with health behaviors and health.1234 Though the concept of social capital is not always clear, its survey indicators usually fall into the five themes of trust; social participation; social networks and support; perception of community; and perceived control (or empowerment).15
Trust is important and is thought to be a core component of social capital, for which it can be used as a key indicator.6 According to Putnam, trust is classified as either generalized trust (horizontal trust) in other people or vertical trust in the institutions of society.7 Another important aspect of social capital is social participation, which is closely related with trust among individuals in both dimensions.89 High levels of social participation in different organizations often cause increased generalized trust between people, and vice versa. This reciprocal influence between social participation and trust can be virtuous or exist in vicious circles.8
Many studies have found that social trust and/or participation are positively associated with self-rated health.34781011 A positive role of social capital for individual health could be partially explained by improved access to health-relevant information (for example, via social interaction through membership in formal and informal organizations), such as having the best hospital or physician nearby,3 which can foster access to healthcare utilization.
A previous study12 showed that generalized trust and social participation at the individual level were related to access to a primary care doctor. Another study7 concluded that the association of trust in the healthcare system with self-rated health in their study might be partly mediated by “not seeking health care when needed.” Both studies suggest that high trust and/or social participation reduce unmet healthcare needs.
However, there has been little evidence in empirical studies for the association of social capital with unmet needs. Only one study13 conducted in Canada reported that social participation in a political or ethnic organization reduced the perceived unmet healthcare needs. No study found in an online database has focused on the relationship of social trust with unmet healthcare needs.
The aim of this study was to investigate whether social capital indicators (generalized trust and social participation at the individual level) have negative associations with subjective assessments of unmet healthcare needs for implications of health policy to reduce these unmet needs.
Go to : 
METHODS
Study population and data collection
The data used in this study were from community health interviews conducted in 40 sub-municipal-level administrative units (called “myeon,” “eup,” or “dong”) of the local city or county government with high mortality rates from August to October in 2010, 2011, or 2012 for Health Plus Happiness Plus Projects, a collection of strategies to address regional health inequalities in the Gyeongsangnam-do Province in Korea. The 8,800 study participants included 220 people from each administrative unit who were sampled systematically using the resident registration database. Interviewees were adults aged 19 or older who had the earliest birth month and day of the year in their respective households, regardless of age. Trained interviewers conducted door-to-door interviews to collect information about sociodemographics, social capital measures, health behaviors, and unmet healthcare needs. The average response rate was 74.8% in 2010 (17 areas), 72.0% in 2011 (12 areas), and 70.3% in 2012 (11 areas). Additional details have been reported elsewhere.14
Before the interviews began, all participants were informed about the aims of the projects and the confidentiality of the information they would provide. They all provided informed written consent.
Measures
Generalized trust
Trust is a difficult concept to measure directly; a wide range of questions has been developed for this purpose.1 In this study, generalized trust was chosen as a measure of social trust. To obtain more consistent answers, generalized trust was assessed with three questions used in the Health Survey for England by the National Center for Social Research15 and in the European Social Survey.16 The questions were as follows: “Generally speaking, would you say that most people can be trusted, or you can't be too careful in dealing with people?” with responses of “can be trusted,” “can't be too careful,” or “don't know”; “Would you say that most of the time, people try to be helpful or just look out for themselves?” with responses of “try to be helpful,” “look out for themselves,” or “don't know”; and “Do you think most people would take advantage of you if they got the chance, or would they try to be fair?” with responses of “take advantage,” “try to be fair,” or “don't know.”
Generalized trust was analyzed as a quantitative variable with possible values of 0, 1, 2, or 3, which indicated the number of positive responses to the three questions.
Social participation
To measure social participation, participants were asked if and how actively (very actively, actively, neutral, not actively, not at all actively) they had been involved in formal groups (political parties, school associations, religious meetings, women's clubs, environmental groups, groups for youth or older people, volunteer groups, unions, neighborhood watch groups) and informal groups (various social gatherings, adult education groups, sports groups, other groups). If participants reported their levels of participation in these activities as “not active” or “not at all active,” their responses were re-coded as “no participation.”
Social participation was analyzed as a categorical variable consisting of “no participation,” “only informal participation,” “formal participation only,” and “both formal and informal participation.”
Unmet healthcare needs
In most studies, unmet healthcare needs have been presumed to be subjective and not chosen by the individual; for example, a person perceives himself or herself to be in need of some form of healthcare but does not receive it because of access barriers.17 Similarly, in this study, unmet healthcare needs were measured subjectively using the following question: “During the past 12 months, was there ever a time when you felt that you needed healthcare (excluding dental care) at hospitals or clinics but did not receive it?” with possible responses of either “yes” or “no”; this process was conducted much in the same manner as in the Korea National Health and Nutrition Examination Survey (KNHANES) and in other studies.1718 Responses of “yes” were coded as “unmet healthcare needs.” Those who responded “yes” were asked to answer a follow-up question, “Why didn't you receive healthcare?” and to choose their own reasons for not obtaining care from possible selections of “cost,” “difficulties in making an appointment with a doctor,” “having no available babysitter,” “transportation problems (too far),” “no available clinics or hospitals at night or on the weekend,” “long waiting times,” “health problems (including physical handicaps),” or “unable to leave work or school.”
Sociodemographics, self-rated health, and perceived stress
Sociodemographic factors of gender, age, marital status, educational level, occupation, food security, and administrative unit (myeon, eup, and dong) were included as covariates in the analysis. Age was stratified into five categories: ≤ 39, 40–49, 50–59, 60–69, and ≥ 70 years. Based on the participants' responses, marital status was categorized into one of four groups: living with a spouse; not married (age ≥ 30); not married (age ≤ 29); and divorced, widowed, or other. Educational level was reported as the highest educational degree completed by the respondent and was categorized as no education; elementary school; middle or high school; and junior college or more. Participants' occupations were categorized into one of seven groups: manager, professional, or clerk; sales or service; farmer or fisherman; technical engineer; blue-collar worker; housewife; or other/unemployed. Accurate information on household income was difficult to obtain, so we replaced it with information about household food security, which is a good indicator of household income.19 We used the following question from the Canadian Community Health Survey20: “Which of the following statements best describes the food eaten in your household in the past year?” Based on the responses, household food security was categorized into one of four groups: always enough of the desired foods; usually (but not always) enough of the desired foods; sometimes not enough; and often not enough. Administrative unit (myeon, eup, and dong) was categorized as either city (dong) or rural area (myeon or eup).
As health status is an important correlate of unmet needs,1321 we considered self-rated health as a covariate. Participants were asked to rate their own general health on a five-point scale: very good; good; fair; poor; and very poor. These ratings ultimately were categorized into three groups: good, fair, and poor. We also included perceived stress level as an important confounder because experiencing stress in life was a significant and strong predictor of unmet healthcare needs in a previous study.13 To measure the amount of perceived stress, we asked a single question: “How much do you feel stressed in your daily life?”; this same question was used in the KNHANES.19 Perceived stress was categorized into four groups: almost none, low, high, and very high.
Statistical analysis
In a simple analysis, we created cross-tabulations to analyze the associations of sociodemographic variables, self-rated health, and perceived stress with unmet healthcare needs. P values were calculated using the χ2 test. Crude odds ratios (ORs) and 95% confidence intervals (CIs) were assessed with a bivariate logistic regression to analyze the associations of generalized trust and social participation in organizations with unmet healthcare needs. Adjusted ORs and 95% CIs were also calculated using multiple logistic regression analysis. The analysis proceeded in three steps. The regression models were Model 1, in which the unmet healthcare need was regressed on sociodemographic variables; Model 2 (Model 1 plus self-rated health and perceived stress); and Model 3 (Model 2 plus the social capital indicators of generalized trust and social participation in organizations). Thus, we calculated the adjusted ORs for unmet healthcare needs based on the aforementioned measures of social capital. A greater than or equal to two log change in likelihood between Model 2 and Model 3 indicated that adding social capital indicators to Model 2 would further improve the fit. All analyses were performed using PASW Statistics 18 (WinWrap Basic, 2009; IBM Co., Armonk, NY, USA).
Ethics statement
This paper used data from Health Plus Happiness Plus Projects in Gyeongsangnam-do provincial government, Korea. All participants were informed about the aims of the projects and the confidentiality of the information they would give, and signed the written consent. The data were originally collected for governmental health projects, not for study, and this study did not require institutional ethics review and approval according to Korean law.
Go to :
RESULTS
Out of 8,800 participants, 15.7% reported unmet healthcare needs during the past 12 months. Self-rated health, perceived stress, and all the sociodemographic characteristics (gender, age, marital status, educational level, occupation, food security, and administrative unit) were significantly associated with unmet healthcare need (Table 1).
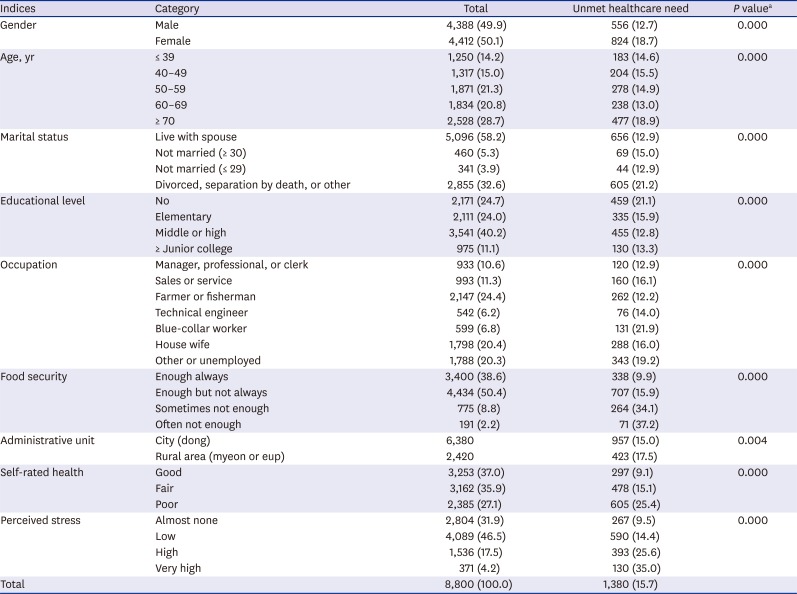
Table 1
Proportion of unmet healthcare need by sociodemographic characteristics, self-rated health, and perceived stress
![]()
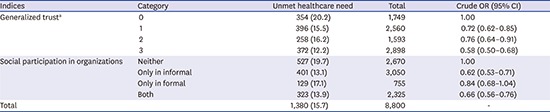
Both generalized trust and social participation in organizations were significantly associated with unmet healthcare needs in the simple analysis. The crude OR for unmet healthcare needs based on one positive response, two positive responses, and three positive responses to the three questions of generalized trust compared to no positive responses was 0.72 (95% CI, 0.62–0.85), 0.76 (95% CI, 0.64–0.91), and 0.58 (95% CI, 0.50–0.68), respectively. Crude ORs for unmet healthcare needs based on social participation only in informal organizations, social participation only in formal organizations, and social participation in both informal and formal organizations compared to no social participation were 0.62 (95% CI, 0.53–0.71), 0.84 (95% CI, 0.68–1.04), and 0.66 (95% CI, 0.56–0.76), respectively (Table 2).
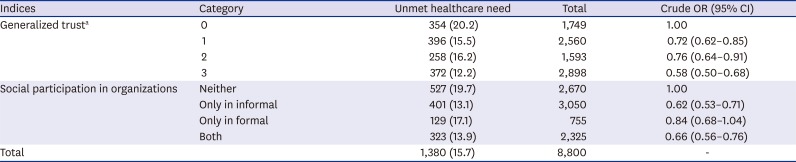
Table 2
Associations of generalized trust and social participation in organizations with unmet healthcare need
Values are presented as number (%).
OR = odds ratio, CI = confidence interval.
aNumber of positive responses to the 3 question items of generalized trust.
![]()
Including self-rated health and perceived stress (Model 2) in the logistic regression for Model 1 significantly improved the fit. Adding generalized trust and social participation in organizations (Model 3) further improved the fit, confirming that social capital had an independent association with unmet healthcare needs. Both generalized trust and social participation in organizations were significantly associated with unmet healthcare needs in the logistic regression analysis. Though the strengths of the associations were weakened, the significances were maintained after adjustment for sociodemographic variables, self-rated health, and perceived stress (Table 3).
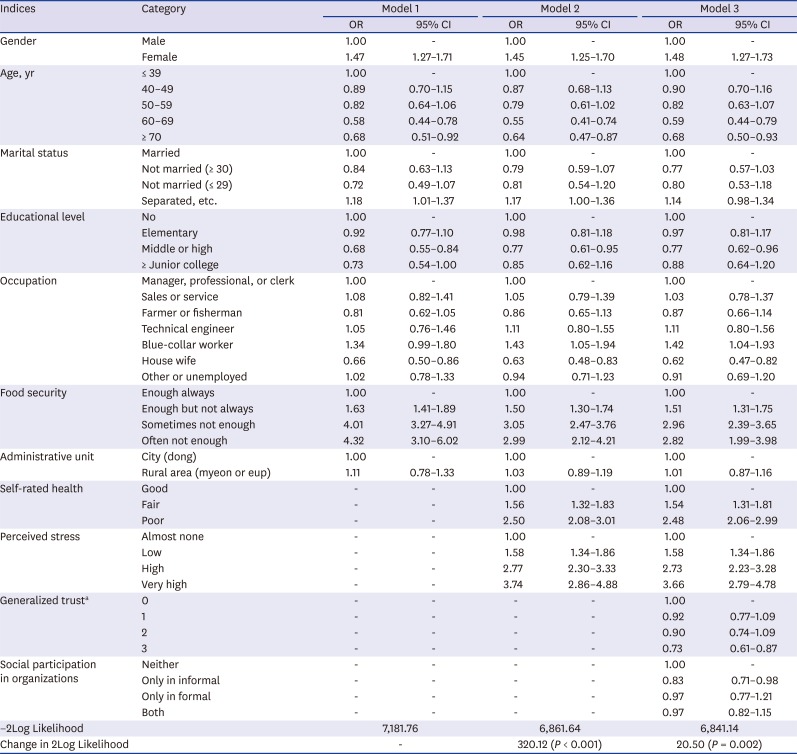
Table 3
Adjusted odds ratios (95% CI) of sociodemographic characteristics (Model 1), self-rated health and perceived stress (Model 2), and social capital measures (Model 3) for unmet healthcare need in the logistic regression analysis
OR = odds ratio, CI = confidence interval.
aNumber of positive responses to the 3 question items of trust.
![]()
The adjusted ORs for unmet healthcare needs based on one positive response, two positive responses, and three positive responses to the three items of generalized trust compared to no positive responses were 0.92 (95% CI, 0.77–1.09), 0.90 (95% CI, 0.74–1.09), and 0.73 (95% CI, 0.61–0.87), respectively. The adjusted ORs for unmet healthcare needs based on social participation only in informal organizations, social participation only in formal organizations, and social participation in both informal and formal organizations compared to no social participation were 0.83 (95% CI, 0.71–0.98), 0.97 (95% CI, 0.77–1.21), and 0.97 (95% CI, 0.82–1.15), respectively (Table 3).
The reported reasons for unmet needs among the 1,380 persons who reported perceived unmet healthcare needs were as follows: cost (56.7%); being unable to leave work or school (26.4%); experiencing health problems, including physical handicaps (25.7%); no available clinics or hospitals at night or on the weekend (23.8%); transportation problems (too far) (20.9%); long waiting times (17.2%); difficulties in making an appointment with a doctor (13.6%); and having no available babysitter (2.8%) (Table 4).
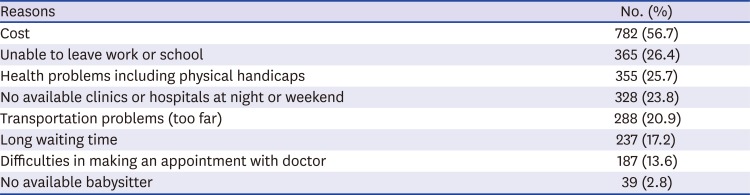
Table 4
Distribution of reasons (multiple responses) for unmet healthcare need among those who reported unmet healthcare need (n = 1,380)
![]()
Go to :
DISCUSSION
This study demonstrated that both generalized trust and social participation in an informal organization were significantly and negatively associated with unmet healthcare needs regardless of potential confounders of sociodemographic characteristics, self-rated health, and perceived stress in Korean communities with high mortality. Those with the highest amount of generalized trust or with social participation in informal organizations were less likely to report perceived unmet healthcare needs. We provide evidence that social capital has an impact on health services, which has been less apparent despite many studies on the subject of social capital and health.22
As a measure of social trust, we assessed generalized trust with three questions that have been adapted from questions included in the United States Social Survey and used in the Health Survey for England. Despite high correlations among the three questions and a lengthy interview, it is recommended to include all of them for a more consistent analysis across studies and countries.15
As unmet healthcare needs were found to be associated with poorer health status and healthcare utilization, further studies of this area are needed to provide policy-relevant information and implications.17 In this study, unmet healthcare needs, the dependent variable, was based on individuals' subjective assessment conducted using either “clinical” or “subjective” methods of measurement. Assessments of subjective unmet needs are superior and more feasible than clinical ones because individuals can easily estimate their health status; there are also numerous existing surveys pertaining to this topic.17
The prevalence of subjective unmet needs in this study population was 15.7% (12.7% for men and 18.7% for women), which was similar to the findings (12.3% for men and 20.8% for women, respectively) of the 2012 Korea National Health Statistics23 and higher than an international EU Survey of Income and Living Conditions (EU-SILC) (range, 1.3% in Denmark to 13% in Sweden).24 Another study25 conducted in Canada showed a lower prevalence of unmet needs (11.7%) than was found in the present study. A long waiting time (36%) was the most important reason for self-perceived unmet needs, whereas cost (12%) was the third most cited cause. The relative lack of direct cost-related barriers to healthcare is due to the universal healthcare coverage in Canada.17 Korea has a national health insurance system that is both publicly and privately funded; however, there are some limitations in benefit coverage and high out-of-pocket payments.26 We suspect that this influenced the higher prevalence of unmet needs than in European countries or in Canada; the most important stated reason (57%) in our study was cost. It is therefore necessary to investigate unmet needs in different socio-legal contexts.
Though some studies have suggested that social trust and/or social participation might reduce unmet healthcare needs, there have been few empirical studies on the association of social capital and unmet needs. Social participation in a formal organization reduced perceived unmet healthcare needs in a prior study13 in Canada, whereas social participation in informal organizations had the same effect in this current study. A literature review suggested some plausible mechanisms for how social participation might reduce perceived unmet healthcare needs. For instance, social participation may facilitate social support,27 allowing for greater information sharing (e.g., on the availability of services, their location and any eligibility criteria) and support to schedule and attend medical appointments and to better cope with healthcare issues.1328 Informal assistance, such as babysitting and offering a ride, as well as financial support to cover out-of-pocket expenditures also can be provided in case of illness.3 In our study, the type of social participation that fostered healthcare was observed in only one informal organization in multivariate analysis, unlike in a Canadian study,13 which may indicate a sociocultural difference between the two countries. Examples of formal organization in this study were political parties, school associations, religious meetings, groups for youth or older people, and unions. Membership in these organizations mainly depends on one's sociodemographic characteristics and is largely irrespective of their preferences for the members. This is not the case in informal organizations, suggesting that greater social support is provided in the presence of familiarity among members.
Despite the suggestions of some studies of a negative relationship between generalized trust and unmet healthcare needs,712 no study has explored this topic thus far. This study found that those with the highest amount of generalized trust reported lower perceived unmet healthcare needs independent of social participation and of other confounders. One plausible explanation is that high levels of generalized trust often lead to high amounts of social participation in different organizations8 and thus facilitate formal and informal social support, simplifying access to healthcare services. In this case, adding social participation as a covariate could weaken the association between generalized trust and unmet healthcare needs. However, the independent associations of unmet healthcare needs with both generalized trust and social participation were maintained by the logistic regression. We do not think that generalized trust promotes social participation and then decreases unmet healthcare needs. Instead, an alternative explanation is the positive correlation of horizontal (generalized) trust with vertical trust.29 High generalized trust levels might cause high trust levels in the healthcare system (vertical trust) and therefore increase the likelihood of seeking healthcare when needed, as suggested in a previous study.7 Another possible mechanism is in the context of reciprocal trust indicated in game theory, in which cooperative equilibrium is achievable only if each player trusts others.3 Social support and informal assistance for seeking healthcare may be facilitated by reciprocal trust (as indicated by a high level of generalized trust) as well as by social participation.
Our study has some limitations. First, like other investigations on social capital and self-rated health, this study was based on cross-sectional survey data. An association in such a study does not always imply a causal relationship but instead simply means that people with a high level of generalized trust and/or informal social participation are likely to have a low level of unmet healthcare needs. However, it is unlikely that seeking healthcare services causes people to trust others or to take part in an informal organization in their community. Nevertheless, further study using a cohort design is needed to exclude the possibility of reverse causation. Second, we measured social capital using aggregated individual-level questions. As the concept of social capital is usually understood at the group level,5 a multilevel analysis could provide useful information regarding the influence of contextual social capital on behavior.30 A study conducted in Canada31 showed that community social capital, as measured by the Petris Social Capital Index, was not significant regarding the use of general practitioners. Most studies on health service utilization have not considered both individual-level and community-level social capital concurrently.22
Both generalized trust and social participation in an informal organization were negatively associated with unmet healthcare needs regardless of potential confounders of sociodemographic characteristics, self-rated health, and perceived stress in Korean communities with high mortality. This study suggested some implications in health policy aimed at reducing unmet healthcare needs.
Go to :
 XML Download
XML Download