

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic diseases are highly related to the behavior of individuals and they are preventable through changes in the knowledge, beliefs, attitudes, and social environments of individuals.1 It is clear that people do not always engage in healthy behavior, because multiple factors can lead to unexpected outcomes for any given health behavior. Stage theories may be used to better understand the complex relationships among health behaviors and the multiple influences of various factors.23 For example, the Precaution Adoption Process Model (PAPM) model suggests that different individuals may be at different levels of awareness and motivation regarding their health behaviors, and it is important to determine the current status of each particular individual.
Currently, the rapid increase in the number of Koreans with chronic diseases has highlighted the importance of population-wide prevention strategies and their application to public health. An overwhelming amount of evidence links behavioral factors to a variety of cancers.4567 In Korea, individual behavior changes aimed at preventing cancer have been an important issue since the introduction of the 10 codes for cancer prevention in 2006, which suggests that the enactment of preventative behaviors can mitigate cancer development. Although information on cancer-related behaviors has been disseminated since the introduction of the 10 codes, research has shown that the influence of the level of knowledge on behavioral changes remains limited in Korea.
Because smoking is one of most important and avoidable causes of cancer and is included in the 10 codes for cancer prevention, this study placed a particular focus on smoking behaviors. While there are many reasons to continue smoking in spite of its well-documented consequences for health, many studies have shown or have done the research with underlying assumption that smokers misperceive the risks of smoking.89101112 There are studies which have investigated whether smokers underestimate their health risks through the manipulated misleading beliefs about the smoking by tobacco companies.91012 Recently, there are studies attempting to answer how the knowledge, beliefs, and attitudes causes smokers to change their smoking behaviors.811
In this context, the present study attempted to explain how tobacco-related knowledge and awareness could be related to smoking behaviors in Korea.
METHODS
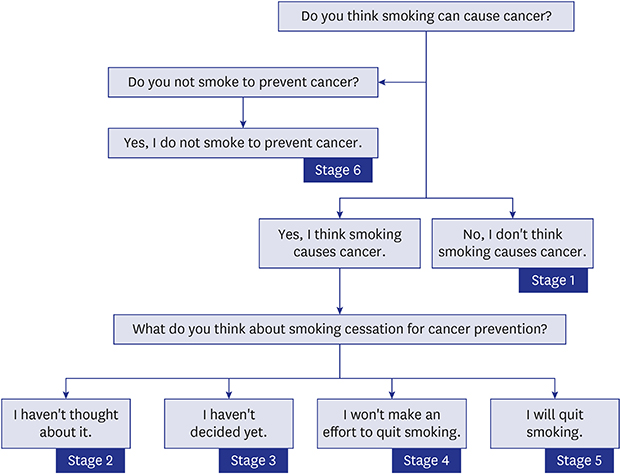
The present study employed a national questionnaire survey that was designed by the National Cancer Center, Korea and the Ministry of Health and Welfare for monitoring awareness and behaviors on 10 codes for cancer prevention that can be followed in daily life, such as smoking cessation, healthy diet, exercise, and screening tests for early detection. The survey was initiated in 2007 and has been carried out annually until 2010 and biannually thereafter. The study population of each year was selected randomly and stratified based on age, gender, and residence using Korean census data, and the survey was conducted via face-to-face interviews using a structured questionnaire based on the PAPM. Traditionally, the PAPM has been applied successfully to predict a wide range of health-related behaviors, including smoking cessation.13 This model includes stage 1: unaware of a risk or precaution, stage 2: aware of but unengaged, stage 3: engaged and deciding on whether to perform or not perform the behavior, stage 4: made the decision not to act, stage 5: made the decision to act but not yet in action, stage 6: acting out the behavior, and stage 7: maintaining the behavior. The distribution of stages among the study subjects was determined by asking whether the subject thought smoking could cause cancer, whether the subject did not smoke to prevent cancer, and the subject's opinion on smoking cessation for cancer prevention (Fig. 1).
 | Fig. 1Schematic flow chart illustrating the steps involved in defining the PAPM stages.
PAPM = precaution adoption process model.
|
The survey data from the 2010 (n = 1,006) were only used for the current analysis, where tobacco related knowledge were investigated together with awareness and behaviors on 10 codes for cancer prevention which have been monitored, routinely. The 12 statements for tobacco related knowledge were certified and developed by professionals with expertise related to tobacco control in Korea. The subjects could either agree or disagree about the truth of each statement by selecting one of two response options: true or false (Fig. 2). A quantitative method was used to assess the level of tobacco-related knowledge based on the total number of correct answers provided by each participant. The highest knowledge group was defined as subjects who had more than 9 correct answers which should have at least one correct answer among the 4 statements (the number of statement is 7, 8, 10, and 11) which showed the lowest percent of correct answers among 12 statements. Subjects who had 5 to 8 correct answers were classified as middle level of knowledge group and rest of them were classified as the lowest knowledge group.
 | Fig. 2Percentage of study subjects who correctly answered each statement regarding tobacco-related knowledge.
|
Furthermore, additional health measures were assessed by asking the subjects whether they had an interest in health (yes or no) and to rate their own health (good or poor).
The assessed sociodemographic characteristics included gender (men/women), age (19–29, 30–39, 40–49, 50–59, or 60+ years of age), place of residence (metropolitan/small city or country), education level (middle school or less, high school, or postsecondary and beyond), occupation (blue collar, white collar, or other), and monthly income (in Korean won).
All data were analyzed using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were used to calculate the frequencies of the responses for the sociodemographic characteristics, awareness of health-related behaviors, and the total number of correct answers for tobacco-related statements. Additionally, differences between men and women were compared. The χ2 analyses were employed to assess differences in knowledge, awareness, and behaviors; for data with expected values below 10, Fisher's exact test was used. Student's t-tests were used to compare overall cancer knowledge and smoking status with each of the independent variables. A multivariate logistic regression model was performed to produce odds ratio (OR) and 95% confidence intervals (CIs) for the influence of the level of smoking-related knowledge on the changing pattern of awareness and behaviors regarding smoking and cancer prevention. For the analyses, the PAPM stages were divided into two groups: stage 1–4 (reference case) and stages 5–6 (event case). Stage 5 (decided) and stage 6 (acting) were differentiated as event case compare to other stages in change of behaviors because these stages are closer to practicing of behaviors while other stages are in unaware or undecided. A P value < 0.05 was considered to indicate statistical significance.
RESULTS
A comparison of the distributions of the major characteristics according to level of tobacco-related knowledge
Of the 1,006 subjects in the present study, 129 correctly answered fewer than four tobacco-related statements (12.8%), 592 correctly answered between five and eight tobacco-related statements (58.8%), and 285 correctly answered more than nine tobacco-related statements (28.3%). Moreover, the level of tobacco-related knowledge was significantly associated with age, education level, monthly income, and smoking status (Table 1).
Table 1
Distributions of demographic characteristics, self-rated health status, and health-related interests according to the level of tobacco-related knowledge
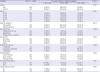
Data are presented as number (%).
aBlue collar: sales, service and craft workers, skilled laborers, and machine operators; White collar: managers, professionals, experts, engineers, and office workers; Others: students, unemployed, and housewives; bSample sizes for individual characteristics may not equal the total due to missing values; cTotal number of correct answer for 12 statements on tobacco related knowledge.
![]()
The outcomes of the univariate and multivariate analyses assessing the factors associated with awareness of the relationship between smoking cessation and cancer prevention
Health-related interests (OR, 3.53; 95% CI, 1.77–7.01) and the total number of correct answers for tobacco-related statements (5–8: OR, 2.14; 95% CI, 1.06–4.31; ≥ 9: OR, 4.26; 95% CI, 1.61–11.27) were significantly correlated with awareness of the relationship between smoking cessation (Table 2).
Table 2
OR and CIs of demographic characteristics, self-rated health status, health-related interests, and the level of tobacco-related knowledge for having awareness on smoking cessation can help prevent cancer
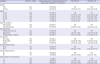
Data are presented as number (%).
OR = odds ratio, CI = confidence interval, Ref = reference.
aBlue collar: sales, service and craft workers, skilled laborers, and machine operators; White collar: managers, professionals, experts, engineers, and office workers; Others: students, unemployed, and housewives; bSample sizes for individual characteristics may not equal the total due to missing values;
cAdjusted for age and gender; dAdjusted for gender, age, place of residence, education level, occupation, self-rated health status, health related interest, and total number of correct answer as appropriate.
![]()
The outcomes of the univariate and multivariate analyses that assessed the factors associated with positive behaviors among all subjects and among current smokers
When age and gender were adjusted, education level, occupation of white collar, health-related interest, and total number of correct answers for tobacco-related statements were significantly correlated with positive attitudes towards smoking cessation behaviors among all subjects. On the other hand, when age and gender were adjusted, only health-related interest (OR, 2.43; 95% CI, 1.10–5.35) and more than nine correct answers for tobacco-related statements (OR, 3.61; 95% CI, 1.45–8.97) were significantly correlated with positive attitudes towards smoking cessation behaviors among current smokers.
After controlling for confounding variables, gender (OR, 7.64; 95% CI, 4.94–11.84), health-related interests (OR, 2.56; 95% CI, 1.63–4.02), and more than five correct answers for tobacco-related statements (5–8: OR, 2.53; 95% CI, 1.57–4.08; ≥ 9: OR, 3.90; 95% CI, 2.22–6.82) were significantly correlated with positive attitudes towards smoking cessation behaviors (subjects in stage 5 and 6). On the other hand, health-related interests (OR, 2.79; 95% CI, 1.23–6.34) and more than nine correct answers for tobacco-related statements (OR, 4.14; 95% CI, 1.60–10.67) were significantly correlated with positive attitudes towards smoking cessation behaviors in current smokers (subjects in stage 5) (Table 3).
Table 3
OR and CIs of demographic characteristics, self-rated health status, health-related interests, and level of tobacco-related knowledge for positive attitudes towards non-smoking (stage 5 and 6 of PAPM) among all subjects and current smokers
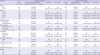
Data are presented as number (%).
OR = odds ratio, CI = confidence interval, PAPM = Precaution Adoption Process Model, Ref = reference.
aBlue collar: sales, service and craft workers, skilled laborers, and machine operators; White collar: managers, professionals, experts, engineers, and office workers; Others: students, unemployed, and housewives; bSample sizes for individual characteristics may not equal the total due to missing values; cStages 5 and 6 of PAPM for all subjects and stage 5 of PAPM for current smokers; dAdjusted for age and gender; eAdjusted for gender, age, place of residence, education level, occupation, self-rated health status, health related interest, and total number of correct answer as appropriate.
![]()
DISCUSSION
The present study aimed to determine the challenges associated with promoting behaviors that help prevent cancer, including reducing the prevalence of smoking, in Korea. More specifically, this study evaluated knowledge regarding smoking and cancer prevention. Overall, the results indicate that many subjects understood tobacco-related statements correctly. Understanding the harmful effects of smoking is important, because it will help individuals to recognize their own situation regarding smoking, leading to positive changes.14 However, a few statements showed misunderstandings that could lead to negative effects on health behavior. In the present study, the subjects exhibited pervasive misperceptions regarding the risk of lung cancer; for example, the vast majority of individuals reported that living in a polluted city results in a greater risk of cancer than does cigarette smoking. A study assessing the prevalence and sociodemographic measures of beliefs regarding cancer risks in the United States reported that the belief that “living in a polluted city is a greater risk for lung cancer than is smoking a pack of cigarettes a day” could affect smoking behaviors by reducing concerns for the risks associated with tobacco.15 Taken together, these results indicate that knowledge regarding smoking continues to be important and that interventions should focus on teaching individuals about the harmful health effects of smoking to create awareness about the related health risks.
One of the strongest findings in the present study was that differences in knowledge regarding attitudes towards smoking cessation exist. Subjects with a higher total number of correct answers for tobacco-related statements were more likely to have positive attitudes towards smoking cessation. Although different health-related behaviors were assessed in previous studies, consistent patterns were observed among higher levels of knowledge and awareness, the promotion of positive attitude changes, and a greater intent to take action.161718 Similarly, the present study found that subjects who had a higher number of correct answers for tobacco-related statements tended to have positive attitudes and behaviors. Several previous studies demonstrated that knowledge, attitudes, and beliefs about risk factors for disease contribute to differences in health-related behaviors.192021
The present study also investigated how the PAPM leads to predicted smoking cessation behavior. Health-related interests and more than nine correct answers for tobacco-related statements could contribute to positive attitudes towards smoking cessation among current smokers. However, over two-thirds of the present subjects reported no interest in or intention to undergo smoking cessation. It has been shown that tobacco-related knowledge and attitudes do not necessarily translate into smoking cessation,11 and although the awareness of smoking cessation is growing, there is still a need to address smoking cessation strategies and interventions for current smokers. Moreover, subjects who correctly answered more than nine tobacco-related statements were four-fold more likely to have a positive attitude towards smoking cessation than were those who correctly answered fewer tobacco-related statements. This finding indicates that interventions should include factual knowledge as well as comprehensive detailed knowledge to aid individuals in making positive changes and to support the long-term maintenance of cessation in current smokers.2223 Overall, these results highlight the importance of a current smoker's stage of change in forming smoking cessation strategies, to determine whether one is open to change or needs further encouragement to undergo smoking cessation.242526
The present study had several limitations that should be taken into account. First, there was a lack of strong scientific evidence regarding the measures of knowledge. The quantitative measure of knowledge based on the total number of correct answers for tobacco-related statements may not have been an objective validation for knowledge. The lack of additional measures limited the interpretation of the relationship between knowledge and changes in health behavior. However, 12 statements on tobacco related knowledge have been selected from 50 statements, which were adopted from frequently asked questions of ‘No Smoke Guide’ website (http://www.nosmokeguide.go.kr/index.do) in 2009 to deliver information on prevention and cessation of tobacco use in Korea, with the review and consensus of experts working on tobacco control in Korea. Second, the generalizability of the present findings may be limited due to the small sample size. Third, cross-sectional studies are not designed to determine causal relationships, and it is possible that acting on smoking cessation after a diagnosis changed attitudes and beliefs. Furthermore, it was not possible to confirm the underlying assumption of the PAPM that positive attitudes lead to action.
In conclusion, this study demonstrated that a higher level of tobacco-related knowledge has an impact on positive attitudes and smoking cessation intentions for the goal of cancer prevention. This was particularly true among current smokers; however, only smokers who correctly answered more than 9 of 12 tobacco-related statements were significantly associated with positive attitudes towards smoking cessation. This indicates the need to disseminate appropriate knowledge to the general population to encourage positive attitudes and promote healthful behaviors. Overall, this study may provide a basic reference on how tobacco-related knowledge can promote smoking cessation behaviors in the Korean population. This study also has important implications for public health policies and supports the need for behavioral intervention strategies that engage people in healthy behaviors with positive attitudes.
 XML Download
XML Download