

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
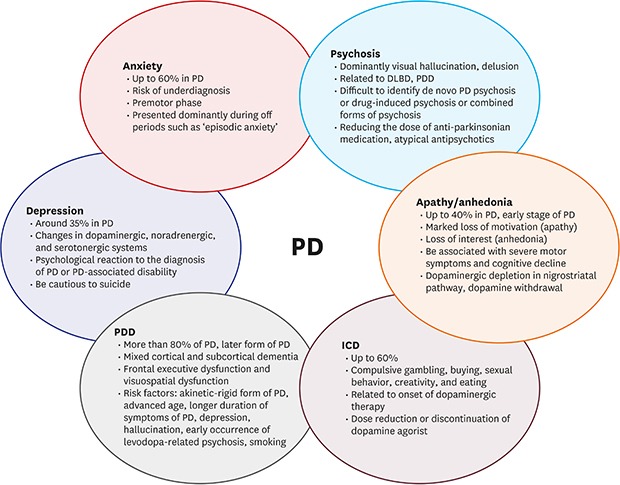
Parkinson's disease (PD) is the second most common neurodegenerative disorder, accounting for 0.5%–5% of the population older than 65 years.1 The prevalence has been shown to increase with age. Motor symptoms, such as bradykinesia, rigidity, tremor, and gait disturbance, resulting from the loss of dopaminergic neurons in the substantia nigra, are the main symptoms of PD. However, the clinical importance of nonmotor symptoms, including hyposmia, rapid eye movement sleep behavior disorder, constipation, and psychiatric symptoms, is being realized. Psychiatric symptoms, such as depression, anxiety, hallucination, delusion, apathy and anhedonia, impulsive and compulsive behaviors, and cognitive dysfunction, appears to be manifesting in most PD patients (Fig. 1).2 Given that the quality of life — and the need for institutionalization — is so highly dependent on the psychiatric well-being of PD patients, psychiatric symptoms are of high clinical significance.34 Here, we reviewed the prevalence, risk factors, pathophysiology, and treatment of psychiatric symptoms in PD patients (Table 1).
Fig. 1
Diagram of psychiatric manifestations in PD. Nonmotor symptoms in PD include various psychiatric symptoms, such as depression, anxiety, psychosis, apathy/anhedonia, ICD, and dementia. These psychiatric symptoms contribute to impaired quality of life for patients and families and are considered risk factors for nursing home placement.
PD = Parkinson's disease, ICD = impulse control disorder, DLBD = diffuse Lewy body disease, PDD = Parkinson's disease dementia.
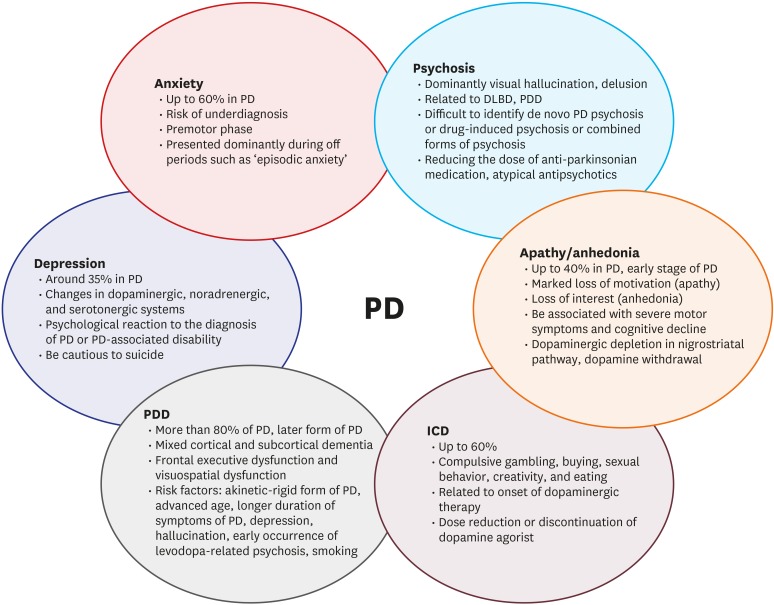
Table 1
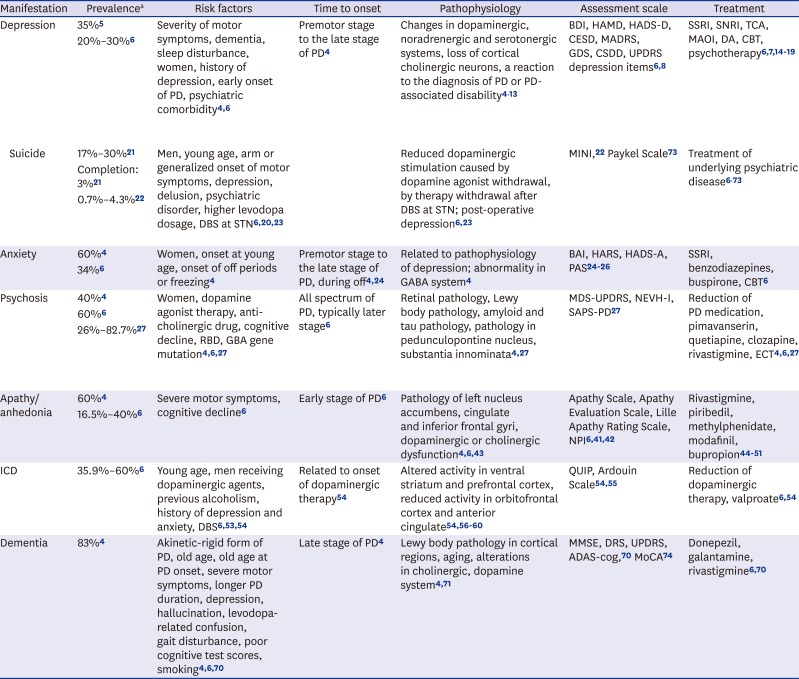
Summary of psychiatric manifestations in PD
| Manifestation | Prevalencea | Risk factors | Time to onset | Pathophysiology | Assessment scale | Treatment | |
|---|---|---|---|---|---|---|---|
| Depression | 35%5 | Severity of motor symptoms, dementia, sleep disturbance, women, history of depression, early onset of PD, psychiatric comorbidity46 | Premotor stage to the late stage of PD4 | Changes in dopaminergic, noradrenergic and serotonergic systems, loss of cortical cholinergic neurons, a reaction to the diagnosis of PD or PD-associated disability413 | BDI, HAMD, HADS-D, CESD, MADRS, GDS, CSDD, UPDRS depression items68 | SSRI, SNRI, TCA, MAOI, DA, CBT, psychotherapy67141516171819 | |
| 20%–30%6 | |||||||
| Suicide | 17%–30%21 | Men, young age, arm or generalized onset of motor symptoms, depression, delusion, psychiatric disorder, higher levodopa dosage, DBS at STN62023 | Reduced dopaminergic stimulation caused by dopamine agonist withdrawal, by therapy withdrawal after DBS at STN; post-operative depression623 | MINI,22 Paykel Scale73 | Treatment of underlying psychiatric disease673 | ||
| Completion: 3%21 | |||||||
| 0.7%–4.3%22 | |||||||
| Anxiety | 60%4 | Women, onset at young age, onset of off periods or freezing4 | Premotor stage to the late stage of PD, during off424 | Related to pathophysiology of depression; abnormality in GABA system4 | BAI, HARS, HADS-A, PAS242526 | SSRI, benzodiazepines, buspirone, CBT6 | |
| 34%6 | |||||||
| Psychosis | 40%4 | Women, dopamine agonist therapy, anti-cholinergic drug, cognitive decline, RBD, GBA gene mutation4627 | All spectrum of PD, typically later stage6 | Retinal pathology, Lewy body pathology, amyloid and tau pathology, pathology in pedunculopontine nucleus, substantia innominata427 | MDS-UPDRS, NEVH-I, SAPS-PD27 | Reduction of PD medication, pimavanserin, quetiapine, clozapine, rivastigmine, ECT4627 | |
| 60%6 | |||||||
| 26%–82.7%27 | |||||||
| Apathy/anhedonia | 60%4 | Severe motor symptoms, cognitive decline6 | Early stage of PD6 | Pathology of left nucleus accumbens, cingulate and inferior frontal gyri, dopaminergic or cholinergic dysfunction4643 | Apathy Scale, Apathy Evaluation Scale, Lille Apathy Rating Scale, NPI64142 | Rivastigmine, piribedil, methylphenidate, modafinil, bupropion4445464748495051 | |
| 16.5%–40%6 | |||||||
| ICD | 35.9%–60%6 | Young age, men receiving dopaminergic agents, previous alcoholism, history of depression and anxiety, DBS65354 | Related to onset of dopaminergic therapy54 | Altered activity in ventral striatum and prefrontal cortex, reduced activity in orbitofrontal cortex and anterior cingulate545657585960 | QUIP, Ardouin Scale5455 | Reduction of dopaminergic therapy, valproate654 | |
| Dementia | 83%4 | Akinetic-rigid form of PD, old age, old age at PD onset, severe motor symptoms, longer PD duration, depression, hallucination, levodopa-related confusion, gait disturbance, poor cognitive test scores, smoking4670 | Late stage of PD4 | Lewy body pathology in cortical regions, aging, alterations in cholinergic, dopamine system471 | MMSE, DRS, UPDRS, ADAS-cog,70 MoCA74 | Donepezil, galantamine, rivastigmine670 | |
PD = Parkinson's disease, BDI = Beck depression inventory, HAMD = Hamilton depression rating scale, HADS-D = hospital anxiety and depression scale-depression subscale, CESD = center for epidemiologic studies depression scale, MADRS = Montgomery–Asberg depression rating scale, GDS = geriatric depression scale, CSDD = Cornell scale for depression in dementia, MDS-UPDRS = Movement disorder society-unified Parkinson's disease rating scale, SSRI = selective serotonin reuptake inhibitors, SNRI = serotonin–norepinephrine reuptake inhibitors, TCA = tricyclic antidepressants, MAOI = monoamine oxidase B inhibitor, DA = dopamine agonists, CBT = cognitive behavioral therapy, DBS = deep brain stimulation, STN = subthalamic nucleus, MINI = mini-international neuropsychiatric interview suicidality module, RBD = rapid eye movement sleep behavior disorder, GBA = glucocerebrosidase, GABA = gamma-aminobutyric acid, BAI = Beck anxiety inventory, HARS = Hamilton anxiety rating scale, HADS-A = hospital anxiety and depression scale-anxiety subscale, PAS = Parkinson anxiety scale, NEVH-I = north-east visual hallucinations interview, SAPS-PD = scale for the assessment of positive symptoms in Parkinson's disease, ECT = electroconvulsive therapy, NPI = neuropsychiatric inventory, QUIP = questionnaire for impulsive-compulsive disorders in Parkinson's disease, ICD = impulse control disorder, MMSE = mini-mental state examination, DRS = dementia rating scale, ADAS-cog = Alzheimer's disease assessment scale-cognitive subscale, MoCA = Montreal cognitive assessment.
aAmong the patients with Parkinson's disease.
DEPRESSION
The prevalence of depression in PD patients is 20%–35%,56 and the 1-year incidence of minor depression is 18%.7 The prevalence and incidence of depression in PD patients are varied depending on the diagnostic criteria. Depression can manifest anytime, from the premotor stage to the late stages of the disease.4 Depression in PD patients generally involves apathy, anhedonia, somatic, and neurovegetative symptoms, such as fatigue, concentration difficulty, insomnia, etc.; therefore, it may be challenging to identify clinical depression in PD patients.8 Depressive symptoms can be assessed using general depression scales, such as Beck Depression Inventory, Hamilton Depression Rating Scale, Hospital Anxiety and Depression Scale-depression subscale, Centre for Epidemiologic Studies Depression Scale, Montgomery–Asberg Depression Rating Scale, Geriatric Depression Scale, Cornell Scale for Depression in Dementia, and Unified Parkinson's Disease Rating Scale (UPDRS) depression item.68 Risk factors of depression are women, severity of motor symptoms, occurrence of motor complications or fluctuations, dosage of dopaminergic medication, cognitive decline and dementia, psychotic episodes, anxiety, and sleep disturbance.46
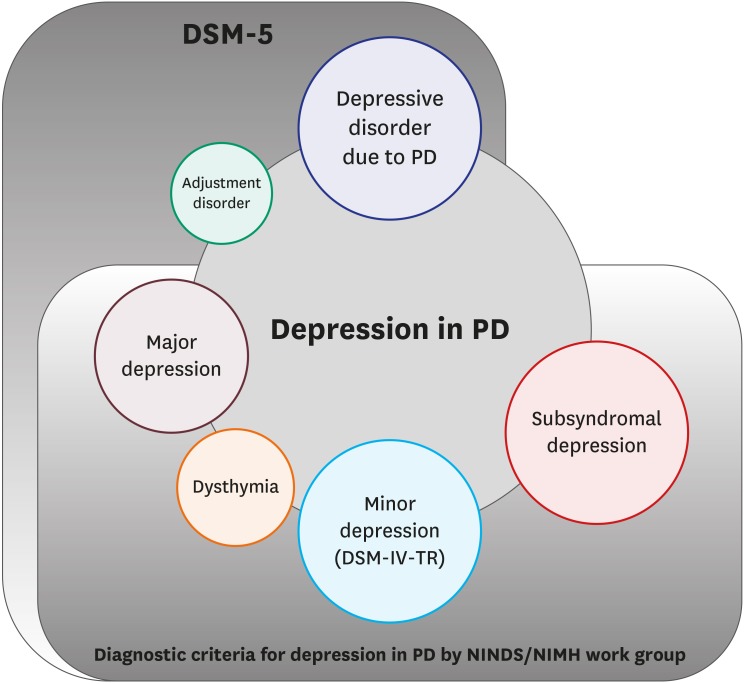
Depressive symptoms in PD patients can manifest across a wide range of severity, chronicity and etiology, including major depression, dysthymia, minor depression, subsyndromal depression or depressive disorder due to PD, and adjustment disorders (Fig. 2).910 According to the provisional diagnostic criteria for depression in PD patients and the Diagnostic and Statistical Manual of Mental Disorders (5th Edition), the criteria for diagnosing major depression are as follows: persistent and pervasively depressed moods, loss of interest and pleasure with other cognitive and somatic symptoms. Dysthymia is defined as a persistent chronic depressive disorder, lasting more than two years. The depressive symptoms in minor depression involve fewer symptoms and less impairment than major depression. Subsyndromal depression can be diagnosed for depressive symptoms that do not meet the criteria for major depression, dysthymia, or minor depression with respect to severity and symptom duration; the depressive symptoms are of short duration or are not ‘present most of the day, nearly every day.’ For example, depressive symptoms that arise only during the off phase of motor fluctuation in PD can be classified as subsyndromal depression. Depressive disorder due to PD refers to depressive symptoms which could have direct pathophysiological relevance to PD, regardless of symptom severity; it can manifest a depressive episode responsive to dopamine replacement therapy or major depressive-like episodes, even with mixed features of manic or hypomanic episodes. Adjustment disorders are a reactive depression, such as grief and demoralization, to the diagnosis of PD. A systemic review reported that the weighted prevalence of major depressive disorder was 17% of PD patients, that of dysthymia was 13%, and that of minor depression was 22%.11 In the depression in PD, symptoms as irritability and dysphoria are more frequent than in the major depression not related to PD, while guilt, self-blame, and suicide attempts are less usual.12
Fig. 2
Diagnostic nomenclature of depression in PD. The Diagnostic and Statistical Manual of Mental Disorders (5th Edition) by American Psychiatric Association classifies depression according to its etiology and symptom severity. The provisional diagnostic criteria for depression in Parkinson's disease proposed by the NINDS/NIMH Work Group classifies depression according to the presence or absence of symptoms and severity.
PD = Parkinson's disease, DSM-IV-TR = a text revision of diagnostic and statistical manual of mental disorders (4th edition), DSM-5 = diagnostic and statistical manual of mental disorders (5th edition).
Changes in dopaminergic, noradrenergic, and serotonergic systems are known to be the main pathophysiology of depression in PD patients. Reduction in dopamine transporter at the striatum and limbic brain regions, decrease in forebrain serotonin innervation, reduction in dopaminergic and noradrenergic innervation in the locus coeruleus, thalamus, and limbic brain regions, as well as an increase in neuronal loss and gliosis in locus coeruleus are evidences for changes in neurotransmitter systems related to depression. The loss of cortical cholinergic neurons also involves depression. Psychological reactions to the diagnosis of PD or PD-associated disability also play a role in triggering depression.413
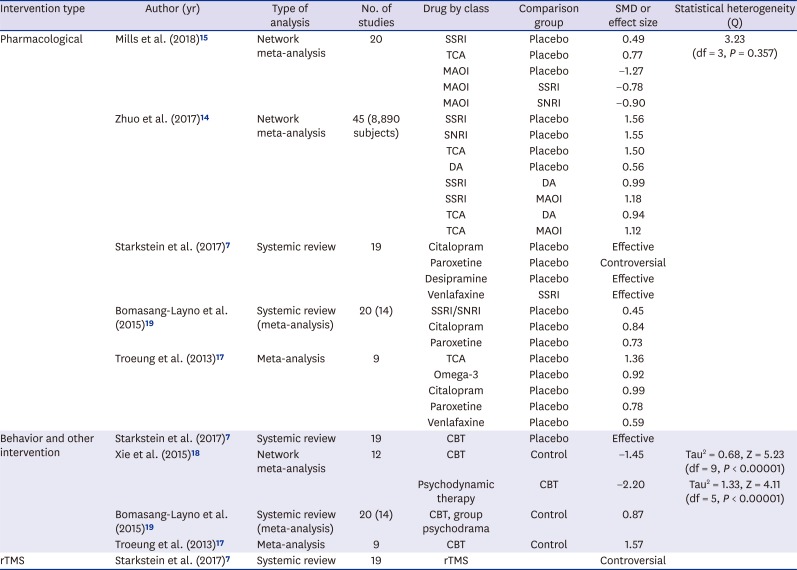
Selective serotonin reuptake inhibitors have a satisfying efficacy for depression in PD (Table 2). They show outstanding efficacy, not only in depression, but also in daily living and motor function.1415 Serotonin–norepinephrine reuptake inhibitors are the safest medication with high efficacy for depression; however, improvements in motor symptoms remain poor.14 Tricyclic antidepressants are also good for improving depression.16 Many previous studies have focused on selective serotonin reuptake inhibitors as the first line of treatment for depression in PD patients; however, monoamine oxidase B inhibitors may also be considered as therapeutic alternatives for depression in PD, showing a higher standardized mean difference than selective serotonin reuptake inhibitors or tricyclic antidepressants.15 As shown previously, monoamine oxidase B inhibitors and dopamine agonists tend to have better performance than serotonin–norepinephrine reuptake inhibitors or tricyclic antidepressants in motor symptoms in PD.6141516 Cognitive behavioral therapy and psychotherapy can also improve depression by improving the executive function.7171819 Nonetheless, further studies are needed to determine whether repetitive transcranial magnetic stimulation works for depression in PD.7
Table 2
Systematic review and meta-analysis of treatment of depression in PD
| Intervention type | Author (yr) | Type of analysis | No. of studies | Drug by class | Comparison group | SMD or effect size | Statistical heterogeneity (Q) |
|---|---|---|---|---|---|---|---|
| Pharmacological | Mills et al. (2018)15 | Network meta-analysis | 20 | SSRI | Placebo | 0.49 | 3.23 (df = 3, P = 0.357) |
| TCA | Placebo | 0.77 | |||||
| MAOI | Placebo | −1.27 | |||||
| MAOI | SSRI | −0.78 | |||||
| MAOI | SNRI | −0.90 | |||||
| Zhuo et al. (2017)14 | Network meta-analysis | 45 (8,890 subjects) | SSRI | Placebo | 1.56 | ||
| SNRI | Placebo | 1.55 | |||||
| TCA | Placebo | 1.50 | |||||
| DA | Placebo | 0.56 | |||||
| SSRI | DA | 0.99 | |||||
| SSRI | MAOI | 1.18 | |||||
| TCA | DA | 0.94 | |||||
| TCA | MAOI | 1.12 | |||||
| Starkstein et al. (2017)7 | Systemic review | 19 | Citalopram | Placebo | Effective | ||
| Paroxetine | Placebo | Controversial | |||||
| Desipramine | Placebo | Effective | |||||
| Venlafaxine | SSRI | Effective | |||||
| Bomasang-Layno et al. (2015)19 | Systemic review (meta-analysis) | 20 (14) | SSRI/SNRI | Placebo | 0.45 | ||
| Citalopram | Placebo | 0.84 | |||||
| Paroxetine | Placebo | 0.73 | |||||
| Troeung et al. (2013)17 | Meta-analysis | 9 | TCA | Placebo | 1.36 | ||
| Omega-3 | Placebo | 0.92 | |||||
| Citalopram | Placebo | 0.99 | |||||
| Paroxetine | Placebo | 0.78 | |||||
| Venlafaxine | Placebo | 0.59 | |||||
| Behavior and other intervention | Starkstein et al. (2017)7 | Systemic review | 19 | CBT | Placebo | Effective | |
| Xie et al. (2015)18 | Network meta-analysis | 12 | CBT | Control | −1.45 | Tau2 = 0.68, Z = 5.23 (df = 9, P < 0.00001) | |
| Psychodynamic therapy | CBT | −2.20 | Tau2 = 1.33, Z = 4.11 (df = 5, P < 0.00001) | ||||
| Bomasang-Layno et al. (2015)19 | Systemic review (meta-analysis) | 20 (14) | CBT, group psychodrama | Control | 0.87 | ||
| Troeung et al. (2013)17 | Meta-analysis | 9 | CBT | Control | 1.57 | ||
| rTMS | Starkstein et al. (2017)7 | Systemic review | 19 | rTMS | Controversial |
PD = Parkinson's disease, SMD = standardized mean difference, SSRI = selective serotonin reuptake inhibitors (citalopram, fluoxetine, paroxetine, sertraline, etc.), TCA = tricyclic antidepressants (amitriptyline, clomipramine, desipramine, nortriptyline, trazodone, etc.), MAOI = monoamine oxidase B inhibitors (lazabemide, rasagiline, safinamide, selegiline, etc.), SNRI = serotonin–norepinephrine reuptake inhibitors (duloxetine, venlafaxine etc.), DA = dopamine agonists (pergolide, piribedil, pramipexole, ropinirole, rotigotine, etc.), CBT = cognitive behavioral therapy, rTMS = repetitive transcranial magnetic stimulation.
Suicide
The prevalence of suicidal ideation is approximately 17%–30% among those with PD, which is two times higher than the general population.2021 The completion rate of suicidal attempt has been reported to be between 0.7% and 4.3%.22 Risk factors of suicide are men, upper extremity or generalized onset of motor symptoms, depression, delusion or any comorbid psychiatric disorder, higher levodopa dosage, and deep brain stimulation (DBS) at the subthalamic nucleus.62023 Among patients treated with DBS, suicidal behavior appears to be associated with postoperative depression and/or altered impulse regulation. A large international multicenter study reported that the prevalence of suicides occurring in the first postoperative year (263/100,000/year, 0.26%) were higher than the age-, gender- and country-adjusted World Health Organization suicide rates (standardized mortality ratio, 12.63–15.64; P < 0.001) and remained elevated at the fourth postoperative year (38/100,000/year, 0.04%) (standardized mortality ratio, 1.81–2.31; P < 0.05).23 One recent study compared 10 PD patients with complete suicide and randomly selected 30 PD patients who died from natural causes.21 PD patients with complete suicide were younger and had less comorbidities, better cognition, lower UPDRS motor scores, lower Hoehn and Yahr stage, and higher use of entacapone than their counterparts.
The pathogenesis of suicidal ideation has been shown to be hypo-dopaminergic syndrome caused by dopamine agonist withdrawal, which is associated with depression, anxiety, apathy, and anhedonia, resulting in suicide attempts.623 After DBS at subthalamic nucleus, reduced dopaminergic stimulation after drug dose reduction may be related to suicide. Treatment of suicide ideation is targeting the underlying suicide-related psychiatric symptoms, such as depression or anxiety.623 Proper management of motor fluctuation is also important to prevent suicide for relatively young, cognitively well-functioning patients with few comorbidities.21 Preoperative assessment, including psychosocial assessments, focusing on the potential suicidal risks before DBS at subthalamic nucleus is recommended as a preventive measure.623
ANXIETY
Anxiety appears to be underrecognized and undertreated in PD patients due to diagnostic imprecision, symptom overlap with motor and cognitive features of PD, complexity of diagnosis, healthcare access and resources, as well as under-reporting of symptoms by patients and caregivers.24 Anxiety symptoms are commonly accompanied by depression; they can be also presented as generalized anxiety with somatic symptoms, anxiety attacks, agoraphobia, and social avoidance. Anxiety and depression are the strongest predictors of poor quality of life. They can occur prior to the onset of motor symptoms to the late stages of PD.4 It can be presented dominantly during off periods as ‘episodic anxiety,’ but does not always correspond with motor fluctuation.24
The prevalence of anxiety in PD patients was shown to be as high as 60%, a frequency greater than that found in community dwelling age-matched controls.4624 Risk factors of anxiety are women, onset at young age, and onset of off periods or freezing.4 Psychosocial factors are related to fear of being unable to function or being embarrassed due to the exhibition of motor symptoms, and biological factors are related to the brain and chemical pathways linked with depression in PD patients, such as abnormal gamma-aminobutyric acid function.4 Degeneration of subcortical nuclei and ascending dopamine, as well as norepinephrine and serotonin pathways within the frontal–basal ganglia circuits may be responsible for symptoms of anxiety.13
Screening using anxiety assessment scales, such as Beck Anxiety Inventory, can improve diagnostic accuracy for anxiety.25 Hamilton Anxiety Rating Scale and Hospital Anxiety and Depression Scale-anxiety subscale can be used to detect anxiety in PD patients; however, they do not show satisfactory validity due to the heterogeneity of anxiety disturbances in PD.24 Parkinson Anxiety Scale – a 12-item observer- or patient-rated scale with three subscales for persistent, episodic anxiety, and avoidance behavior – is easy and brief to administer, offering better clinimetric properties than the existing anxiety rating scales.26
Pharmacological treatments are mainly selective serotonin reuptake inhibitors, benzodiazepines, and buspirone. Nonpharmacological intervention, such as cognitive behavioral therapy, can be a treatment option.6 Because the pattern of anxiety or mood fluctuations can be heterogeneous, adjustment of antiparkinsonian medications to minimize motor fluctuations can be beneficial.24
PSYCHOSIS
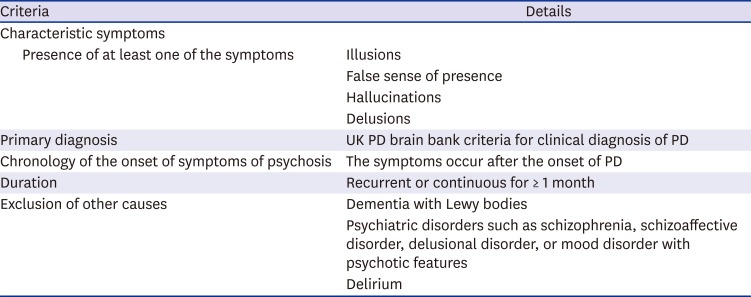
Psychosis as early PD symptoms manifests as passage hallucination (peripheral visual field), illusion, and formed hallucinations. Hallucination is most often presented as visual hallucination of people, animal or inanimate objects. In the early stages, patients are nearly aware of hallucination with preserved insight. In the advanced stages, psychosis manifests as non-visual hallucination and delusions, as well as visual hallucination.6 The contents of delusions are guilt, grandiosity, reference, religious idea, persecution, jealousy, and theft. Delusional misidentification syndrome, such as Capgras delusion, can also be presented.27 The criterion for being considered as having dementia with parkinsonism, such as diffuse Lewy body disease and Parkinson's disease dementia is recurrent visual hallucinations that are typically well formed and detailed. The diagnostic criteria of PD psychosis are summarized in Table 3.28
Table 3
Diagnosis of PD psychosis
The prevalence of visual hallucination ranges from 22% to 38%, and that of auditory hallucination ranges from 0% to 22%.4627 The overall prevalence of psychosis ranges from 26% to 82.7%. The assessment scales are the Movement Disorder Society-Unified Parkinson's Disease Rating Scale, North-East Visual Hallucinations Interview, and Scale for the Assessment of Positive Symptoms in Parkinson's disease.27 Risk factors are women, dopamine agonist therapy, anti-cholinergic drug, cognitive decline, presence of rapid eye movement sleep behavior disorder symptoms, and glucocerebrosidase gene mutations.4627 Psychosis increases the risk of dementia, and cognitive decline is one of the risk factors for psychosis in PD and vice versa.
Decrease in retinal dopamine concentration, thinning of retinal ganglion cell layer in the dominant eye, Lewy body in amygdala and parahippocampal gyrus, high level of amyloid and tau pathology in frontal, parietal, and hippocampal areas are well-established underlying pathophysiologic mechanisms of psychosis in PD patients.427 Brainstem atrophy in pedunculopontine nucleus and substantia innominata are known to be associated with psychosis in PD patients.27
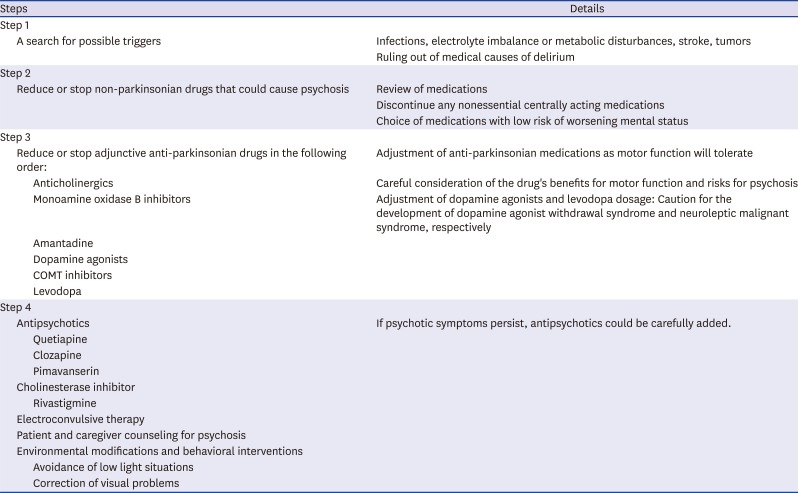
It is difficult to discriminate between de novo PD psychosis, drug-induced psychosis, and combined forms of psychosis. About 30% of patients treated with chronic dopaminergic therapy have drug-induced psychosis. A reduction in PD medication is often the first option to treat psychosis in PD.4627 If PD psychosis does not improve by reducing the dose of PD medication, atypical antipsychotics are often considered. A neuroimaging study showed that PD patients with visual hallucinations have elevated serotonin 2A (5-HT2A) receptor binding density in the visual processing areas.29 Therefore, 5-HT2A receptor inverse agonist is considered for treating psychotic symptoms in PD patients. Pimavanserin, a neocortical 5-HT2A receptor inverse agonist, may be a potential therapeutic medication targeting PD psychosis,2730 which received approval by the Food and Drug Administration in 2016 (Table 4). Compared to the placebo, pimavanserin showed no significant differences in the discontinuation rates due to all causes, adverse effects, and death. Moreover, the incidence of at least one adverse event and serious adverse events were similar between the two groups. The pimavanserin group showed a lower incidence of orthostatic hypotension than the placebo group, suggesting an additional benefit with respect to the management of common nonmotor symptoms in PD patients.3031 Quetiapine, a 5-HT2A blocker with low affinity for dopamine D2 receptors and minimal motor side effects, is the most commonly used antipsychotic in PD psychosis.3233 Although double-blind, randomized, placebo-controlled trials of quetiapine have failed to demonstrate the efficacy in PD psychosis, open-label, rater-blinded studies showed significant improvement. Quetiapine may be useful in mild cases. Clozapine has been regarded to have minimal motor side effects, like quetiapine; it did not show significant effect on the UPDRS motor scores and showed the lowest attrition among the antipsychotics.34 Clozapine was recommended by National Institute for Health and Care Excellence (NICE) in the United Kingdom;35 however, it requires close blood monitoring given the risk of dose-independent leukopenia/neutropenia, since 3% of patients treated with clozapine have experienced leukopenia/neutropenia requiring withdrawal.31 Psychosis with cognitive impairment can be treated by cholinesterase inhibitor, such as rivastigmine. Electroconvulsive therapy is also one of the treatment options for psychosis. Patients usually receive 5 to 12 sessions, and the effects persist for 5 to 30 weeks. Table 5 summarizes a general approach to the management of PD psychosis.
Table 4
Systematic review and meta-analysis of treatment of psychosis in PD

| Intervention type | Author (yr) | Type of analysis | No. of studies | Drug by class | Comparison group | SMD or effect size | Statistical heterogeneity (Q) |
|---|---|---|---|---|---|---|---|
| Pharmacological | Yasue et al. (2016)30 | Systemic review and meta-analysis | 4 | Pimavanserin | Placebo | −2.26 | Tau2 = 0.78 |
| Jethwa and Onalaja (2015)31 | Network meta-analysis | 9 | Clozapine | Placebo | −1.10 | Tau2 = 0.00 | |
| Pimavanserin | Placebo | Effective | |||||
| Frieling et al. (2007)34 | Network meta-analysis | 7 | Clozapine | Placebo | −1.10 | Chi2 = 0.08 |
Table 5
A recommended stepwise approach to the management of PD psychosis
APATHY AND ANHEDONIA
Apathy, defined as a marked loss of motivation not attributable to emotional distress, intellectual impairment, or diminished level of consciousness, is seen throughout the spectrum of neurocognitive disorders.3637 Anhedonia refers to the impaired ability to experience pleasure — in other words, loss of interest — and it is one of the two core symptoms when diagnosing depressive disorder (the other symptom is ‘depressed mood’). Although apathy and anhedonia are often confused with depression, they differ in terms of the mechanisms, therapeutic approaches, and prognoses occurring in PD patients.38 Some symptoms are more specific to apathy; hence, their presence or absence may help separate apathy from depression (Table 6).39
Table 6
Clinical differentiation between apathy and depression
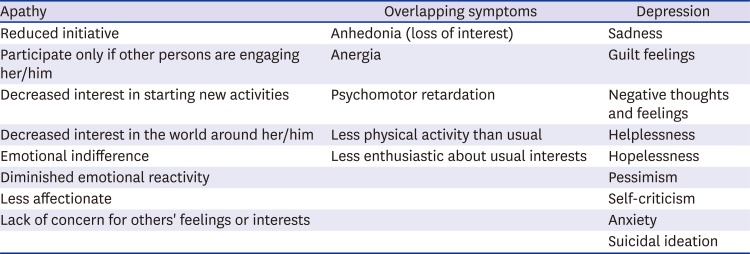
Modified from Pagonabarraga et al.39
The prevalence of apathy in PD is between 16.5% and 40%; it can manifest in the early stage of the disease.6 Although apathy is usually associated with fatigue and anhedonia, about half of the patients with apathy do not suffer from concomitant depression or cognitive impairment. Therefore, apathy could be regarded as a separate clinical entity in PD patients. Apathy among treatment-naïve patients with early-stage PD was shown to be associated with more severe motor symptoms, worse cognitive status, and low quality of life.640 Apathy can be evaluated by using the Lille Apathy Rating Scale41 and the apathy section of Neuropsychiatric Inventory.42 Lille Apathy Rating Scale has four dimensions for evaluating apathy: curiosity, action initiation, emotion, and self-awareness.
Risk factors are severe motor symptoms and cognitive decline.6 Apathy that is associated with the severity of motor symptoms suggests that apathy may be caused by dopamine depletion in the nigrostriatal pathway.43 Apathy in patients with post-DBS showed a relationship with dopaminergic therapy withdrawal. Atrophy of the left nucleus accumbens and reduction on gray matter density in cingulate gyrus and inferior frontal gyrus are suggested as the pathophysiological mechanisms.46
Pharmacological treatments are rivastigmine44 and piribedil,45 a dopamine agonist, whose dosage of up to 300 mg per day led to 34.7% reduction in apathy scores at 12 weeks. Anticholinergics, antidepressants, and nonpharmacological treatment strategies, such as cognitive training and exercise, have been suggested.6 Methylphenidate, modafinil, and stimulating antidepressants, including bupropion, can be used to treat apathy syndrome.46 Methylphenidate and modafinil were not fully investigated to prove efficacy on apathy in PD patients. They may be effective in treating fatigue or PD-related sleep problems, such as excessive daytime sleepiness.4748 Bupropion, one of the norepinephrine–dopamine reuptake inhibitors, was not shown to be effective in treating apathy by clinical trials; however, expert opinion suggested its potential efficacy.49 Since cases of bupropion-related parkinsonism or dystonia have been reported, caution is needed when using bupropion.5051
IMPULSE CONTROL DISORDER
The reported prevalence of impulse control disorder (ICD) varied from 35.9% to 60%.6 Recent longitudinal studies that followed-up PD patients for 5 years reported that the 5-year cumulative incidence of ICD was about 46%.52 Symptoms were revealed as compulsive gambling, buying, sexual behavior, creativity, and eating. ICD is one of the main reasons for referral to the psychiatric department since it can lead to serious financial, legal, or psychosocial consequences.52 Risk factors are young age, dopaminergic therapy especially in men, previous alcoholism, history of depression and anxiety, ICD symptom prior to PD onset, and DBS.65354 The PD-specific assessment scales for ICD are Questionnaire for Impulsive-compulsive disorders in PD (QUIP)54 and Ardouin Scale.55
The relation to dopaminergic therapy is a clue to suggest the relationship between ICD and dopamine replacement therapy.54 Regulation of reward responsiveness and motivational drives may be affected by dopamine replacement therapy. There seems to be difference in brain function between patients with both PD and ICD and those with PD but not ICD at baseline and during risk-taking tasks, especially, in the ventral striatum and prefrontal cortex.56 Hyperactivity in the ventral striatum among PD patient with ICD symptoms, such as pathological gambling, was suggested by some positron emission tomography (PET) studies, which showed greater dopamine release and greater dopamine D2-like receptor availability in the ventral striatum among PD patients with pathological gambling than those without during a gambling task and in response to general rewarding cues during levodopa challenge.57 In contrast, hypoactivity in the ventral striatum was suggested by some functional magnetic resonance imaging studies, which reported that PD patients with ICD showed lower activity in the ventral striatum compared with PD patients without ICD during risk-taking tasks.5859 Another PET research suggested lower activity in impulse control and response inhibition areas, such as the lateral orbitofrontal cortex and rostral cingulate, following the dopamine agonist administration in PD patients with pathological gambling than in PD patients without pathological gambling.60 Relatively reduced activity was also shown in the orbitofrontal cortex and anterior cingulate in PD patients with ICD during a risk-taking task.59 Castrioto et al.61 suggested that ICD and apathy, like levodopa-induced dyskinesia and parkinsonian bradykinesia, lie at the opposite ends of the spectrum of dopaminergic stimulation. They proposed that pulsatile dopamine replacement therapy may induce sensitization of the limbic ventral striatum, leading to a shift from apathy to ICD.
DEMENTIA
The prevalence of Parkinson's disease dementia (PDD) is as high as 83%.4 PD patients has 5–6 folds increase in the risk of dementia compared with healthy controls. The prevalence increases with age and duration of PD; therefore, PDD is a more progressed form of PD.4 Dementia in PD manifests as mixed subcortical and cortical features of dementia. Subcortical features include slowness of thought (bradyphrenia), impaired working memory, executive dysfunction, and visuospatial constructional deficits. Cortical features are comprised of memory impairment and language dysfunction. PDD is shown to be associated with many comorbid behavioral symptoms, including depression (58%), anxiety (49%), hallucination (44%), apathy (54%), disinhibition, and irritability.66 Memory decline is usually not the first symptom; therefore, the diagnosis of PDD tends to be delayed. Frontal executive dysfunction and visuoconstructive disability may initially appear. Administration of the comprehensive neuropsychological battery is necessary for early detection of cognitive decline in PD.
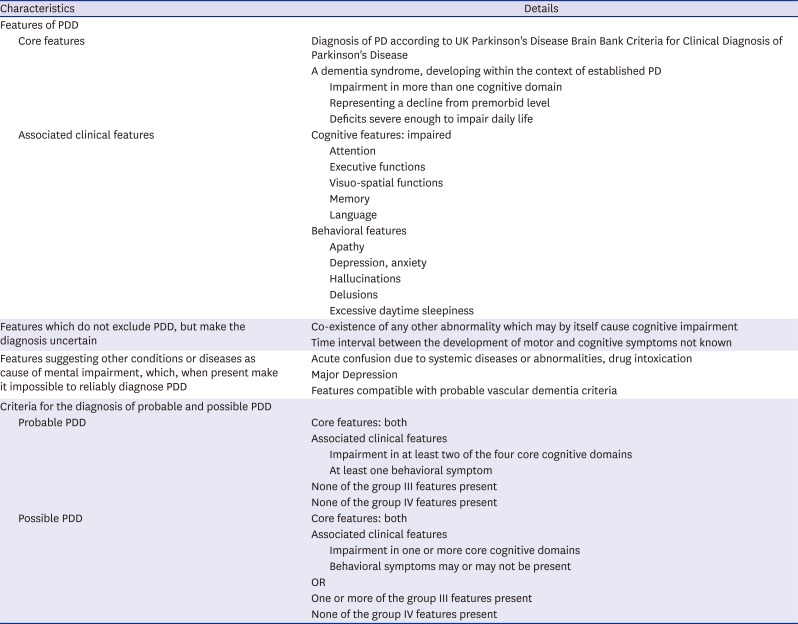
Clinical diagnostic criteria for probable and possible PDD were proposed for the diagnosis of dementia associated with PD by the Movement Disorder Society Task Force for PDD in 2007 (Table 7).67 Because the spectrum of cognitive dysfunction ranges from mild cognitive impairment (MCI) to PDD, the MDS PD-MCI criteria were also developed.68 The Diagnostic and Statistical Manual of Mental Disorders (5th Edition) provided the diagnostic criteria for major neurocognitive disorder due to PD (corresponding to PDD) and mild neurocognitive disorder due to PD (corresponding to PD-MCI).10 The term, PDD, should be used to describe dementia that occurs in the context of well-established PD, and 1-year rule between the onset of dementia and parkinsonism (i.e., motor symptoms precede the onset of dementia by at least one year) has been applied to distinguish dementia with Lewy bodies (less than 1-year) from PDD (more than 1-year).69
Table 7
Diagnosis of PDD
Risk factors of PDD are akinetic-rigid form of PD, advanced age, older age at onset of PD, severe motor symptoms, longer duration of symptoms of PD, depression, hallucination, early occurrence of levodopa-related confusion or psychosis, severe gait and postural reflex disturbances, poor cognitive test scores, and smoking.4670
Dementia can be developed due to Lewy body pathology in posterior cortical regions (notably parietal and temporal) that correspond to Braak's stages of 5 and 6 for PD.71 Aging process, reduction in cortical cholinergic markers, and the loss of dopamine transporter in striatum/inferior frontal gyrus also contribute to the dementing process in PD.4 Cholinesterase inhibitors (donepezil, galantamine, rivastigmine) are pharmacological treatments.670
CONCLUSION
Identification, assessment, treatment, and management of psychiatric symptoms in PD may require comprehensive and multidisciplinary approach based on the Bio-Psycho-Social model.72 Treatment should be tailored to the needs of individual patient based on their unique etiology or pathophysiology of each psychiatric symptom, ranging from pharmacological or nonpharmacological treatment to the psychological and socioenvironmental interventions.
Psychiatric symptoms of PD can be improved if they are identified at the right time and properly treated. It is important to pay close attention to the psychiatric symptoms and to educate the family about the potential symptoms, especially for high-risk patients, prior to symptom onset. Further studies are necessary to better understand the neurobiological mechanism of each symptom and to develop more appropriate pharmacological and nonpharmacological treatments.
 XML Download
XML Download