

 PDF
PDF Citation
Citation Print
Print



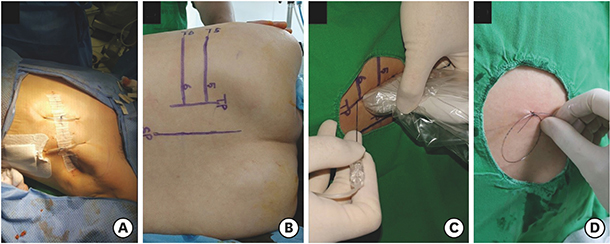
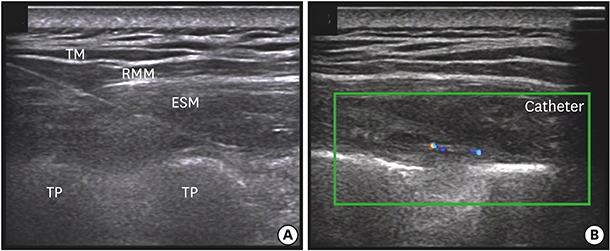
Three patients underwent total mastectomy with sentinel/axillary lymph node dissection. After the surgical procedure, ultrasound (US)-guided erector spinae plane block (ESPB) was performed. The fifth rib and transverse process (TP) was located using a 5–12 MHz linear probe; this was marked on the skin. At this level, the probe was moved from the lateral to the medial side transversely to identify any change in shape that traversed the rib and TP. Where the round shadow of the rib shifted to the rectangular shape of the TP, an 18-G Tuohy needle was inserted by using the in-plane technique (Fig. 1). After penetrating the erector spinae muscle, the needle was located in the fascial plane between the TP and erector spinae muscle. We confirmed that the fascial plane was well-separated by injecting 2 mL of saline. Then, 0.375% ropivacaine 30 mL with epinephrine (1:200,000) was injected, and the catheter was inserted 2 cm over the tip of the needle under real-time US guidance (Figs. 2 and 3). After the ESPB procedure, fentanyl 50 µg and ketorolac 30 mg were administered intravenously, and the patients were allowed to recover from general anesthesia. Postoperative pain was controlled by the acute pain service protocol of our hospital, oral acetaminophen 650 mg three times per day, combined with intravenous fentanyl patient-controlled analgesia (PCA; bolus 0.5 µg/kg without background infusion) and local anesthetic injection (0.375% ropivacaine 30 mL with epinephrine 1:200,000) via catheter every 12 hours for 3 days. Resting and dynamic (coughing, deep breathing) pain scores after surgery were assessed by using the visual analogue scale score.
The resting/dynamic pain scores were maintained below 2 points for 5 days postoperatively, and no additional rescue analgesics were administered during this period. The fentanyl consumption and demand were tracked using the PCA pump. The patients received their first demand dose of 24–34 µg of fentanyl between 12 hours and 15 hours after surgery, and the total number of bolus demands was two (case 1 and 2) and one (case 3) during the entire postoperative period.
Breast tissue is innervated by the anterior and lateral cutaneous branches of the T2–T6 intercostal nerves with variable involvement of the T1 and T7 intercostal nerves, as well as the supraclavicular branch of cervical plexus.1 Thus, thoracic epidural block and thoracic paravertebral nerve block are commonly used for analgesia after breast surgery, primarily by blocking these nerves. However, these techniques involve serious complications and multiple injections are needed.2345
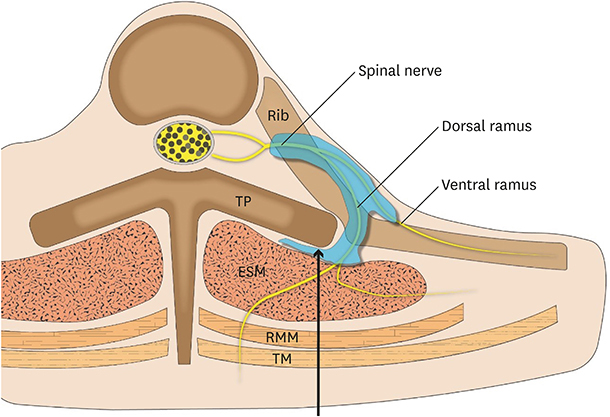
ESPB is a newly emerging truncal block that can cover a wide range, from T1–2 to T8–10,6 due to its wide cephalad-caudad spreading characteristic. It is an easy technique that involves injection of local anesthetic between the TP and erector spinae muscle. Moreover, ESPB can be performed regardless of wound dressing or surgical tissue disruption and is expected to cause less adjacent structural damage than other reginal anesthetic techiques.6789
In conclusion, continuous ESPB provided effective analgesia after mastectomy with sentinel/axillary lymph node dissection. Therefore, we believe that ESPB can be a safe and effective option for analgesia after mastectomy.



 XML Download
XML Download