

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although depressive episodes are not always essential for the diagnosis of bipolar disorder, they are known to have a significant influence on the course of the disease and the function of the patient.1 According to the International Society for Bipolar Disorders (ISBD) task force report for 2013, antidepressants (ADs) may be used as adjunctive treatment to mood stabilizers (MS) or antipsychotics (APS) for an acute bipolar depressive episode and for maintenance treatment in a patient who experienced a relapse of depressive symptoms after stopping AD therapy. The unopposed use of ADs without MS or APS is generally not recommended in bipolar depression, because it may increase affective instability, accelerate episode cycles, and lead to conversion to manic or mixed episodes.2 The causal relationship between the use of ADs and mania remains unclear, and the benefits and disadvantages of AD use in bipolar disorder remains to be clarified.3
Actual clinical prescriptions often differ from the established clinical guidelines for psychiatric drugs,4 and the rate of concordance between prescriptions and the guidelines is particularly low in bipolar depression.5 Many clinicians have used ADs for treatment of bipolar depression,6 because the duration of depressive symptoms is three times longer than that of manic or hypomanic symptoms,7 subsyndromal depressive symptoms cause significant functional impairment,8 and patients with depressive symptoms are at risk for suicide;9 all of these are related to poor prognosis. The results of a questionnaire survey of expert psychiatrists in Korea showed that there was almost no preferred strategy as the initial treatment for bipolar depression.10 The selection of clinical therapeutic agents for bipolar depression is very diverse and inconsistent in the real world.
There have been several studies to date on prescribing patterns for bipolar disorder. Although some studies have reported prescription patterns of psychotropic drugs for bipolar disorder,511 few studies have focused on the prescription of ADs for bipolar disorder.
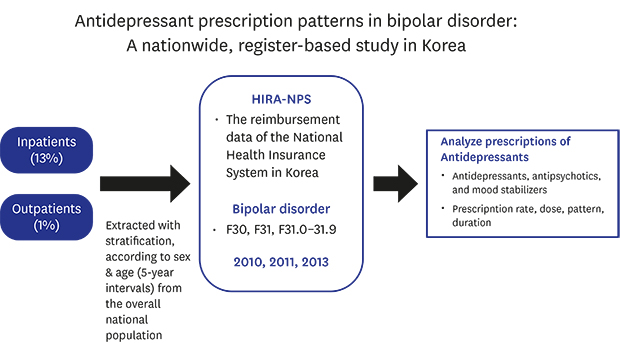
This study aimed to examine the prescription of ADs for patients with bipolar disorder in practice, using nationwide, whole population-based registry data. More specifically, the study aimed to 1) investigate the annual prescription rates of ADs for patients with bipolar disorder and examine changes in the prescription rates during the years 2010, 2011, and 2013, 2) identify the prescription patterns of ADs, whether they are used alone or in combination with MS or antipsychotic drugs, and 3) describe the frequency, dosage, and duration of the use of individual ADs.
Presence of a comorbid life time anxiety disorder is known to be associated with increased use of ADs, and greater severity and impairment in patients with bipolar disorder.1213 We investigated the presence of comorbid anxiety disorders and its influence on AD prescription in patients with bipolar disorder.
METHODS
Data source
The Republic of Korea has a universal, single government-payer health coverage system in which the National Health Insurance (NHI) covers approximately 98% of the national population. The claim data of the NHI include all diagnoses, treatments, procedures, and prescription drugs for patients who have used medical care for one year.14 The Health Insurance Review and Assessment Service-National Patient Sample (HIRA-NPS) in Korea was developed to increase the utilization of health insurance information and to activate public health research using patient sample data. The data were extracted with stratification according to sex and age (in 5-year intervals) from the overall national population. For efficient sampling, data from inpatients and outpatients were separately extracted and assigned different weights. The extraction ratios for inpatients and outpatients were 13% and 1%, respectively, and the total population was reconstructed by weights of 7.69 times for inpatients and 100 times for outpatients.15 The validity and representativeness of HIRA-NPS data were extensively demonstrated by examining and comparing the total amount of medical expenses per patient, the cost per patient, the number of disease outbreaks, and the total number of patients between HIRA-NPS and the whole national population.14 Based on this, various population-based studies using HIRA-NPS data were conducted in Korea, including a study on the prescription patterns of antipsychotic medication in patients with schizophrenia.1617
The present study utilized the Korean HIRA-NPS data for the years 2010, 2011, and 2013 (serial numbers, HIRA-NPS 2010-0078, 2011-0101, and 2013-0066). The prescription data for sample patients diagnosed with bipolar disorder were analyzed for each year (from January 1 to December 31). There was no continuity between the data for the three years.
The bipolar disorder group was defined as follows. According to the Korean Standard Classification of Disease-6 edition (KCD-6), which is a modification of the International Statistical Classification of Diseases and Related Health Problems, 10th edition, all patients were identified who visited a clinic or hospital at least once with a main diagnosis code of manic episode (F30), bipolar affective disorder (F31), hypomanic episode (F31.0), manic episode without psychotic symptoms (F31.1), manic episode with psychotic symptoms (F31.2), mild or moderate depression (F31.3), severe depression without psychotic symptoms (F31.4), severe depression with psychotic symptoms (F31.5), mixed episode (F31.6), currently in remission (F31.7), other bipolar affective disorders (F31.8), or unspecified bipolar disorders (F31.9). We also identified three episodes, according to the main diagnosis at each visit: bipolar disorder, current episode manic (F30, F31.0, F31.1, and F31.2); bipolar disorder, current episode depressed (F31.3, F31.4, and F31.5); and other bipolar disorders (F31.6, F31.7, 31.8, and F31.9). Patients who had multiple main episodes in a year were counted for each episode separately.
Basic demographic characteristics (sex and age) of the patients were recorded. According to the KCD-6, patients who visited at least once with diagnosis codes of neurotic, stress-related, or somatoform disorders (KCD-6, F40.0–F48.9) were identified as anxiety disorders.
ADs and other psychotropic medications
ADs, MS, and antipsychotic drugs were classified according to the World Health Organization's Anatomical Therapeutic Chemical Code (ATC code). During the baseline period of three years, the ADs (ATC code N06A) prescribed were amitriptyline, bupropion, citalopram, clomipramine, duloxetine, escitalopram, fluoxetine, fluvoxamine, imipramine, milnacipran, mirtazapine, nortriptyline, paroxetine, sertraline, tianeptine, trazodone, and venlafaxine. The MS (ATC code N05A for lithium and N03A for other drugs) prescribed were carbamazepine, lamotrigine, lithium, oxcarbazepine, phenytoin, phenobarbital, topiramate, and valproate. The APS (ATC code N05A) prescribed were amisulpride, aripiprazole, bromipridol, chlorpromazine, chlorprothixene, clozapine, haloperidol, olanzapine, paliperidone, perphenazine, quetiapine, risperidone, ziprasidone, and zotepine. Prescriptions of amitriptyline of < 50 mg per day, clomipramine of < 30 mg per day, imipramine of < 50 mg per day, nortriptyline of < 50 mg per day, and trazodone of < 100 mg per day were excluded from the analysis, because these are mainly used for hypnotic purposes at low doses. Prescriptions with a dose greater than 10 times the mean prescribed dose of the drug were removed as outliers.
For each AD, the 1-year prescription rates for patients with depressive, manic, and other episodes were compared. In addition, the 1-year prescription rates for patients with and without comorbid anxiety disorders were compared.
The patterns of AD prescription were classified into four categories: AD monotherapy, ADs combined with antipsychotic agents (AD + APS), ADs combined with MS (AD + MS), and ADs combined with APS and MS (AD + APS + MS). The annual prescription rate and the mean number of days of prescription in one year were calculated for each pattern and for each individual AD.
Statistical analysis
Categorical variables were analyzed by the chi-square test, and one-way analysis of variance and the Jonckheere–Terpstra test were performed for continuous variables. The data were analyzed using R version 3.4.1 (R Core Team [2017]; R: A language and environment for statistical computing; R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/),18 Foreach (version 1.4.3),19 Plyr (version 1.8.4),20 Data.table (version 1.10.4),21 and doParallel (version 1.0.11) softwares.22 P < 0.05 was considered to indicate a statistically significant difference.
RESULTS
Demographics of patients
Overall, 2,022 (in 2010), 2,038 (in 2011), and 2,626 (in 2013) patients visited psychiatric clinics or hospitals with a main diagnosis of bipolar disorder (the number of subjects sampled from the national data set, Table 1). The mean age of the patients was 45.4 years (standard deviation [SD], 16.56; 2010), 44.5 years (SD, 16.87; 2011), and 46.5 years (SD, 17.28; 2013). The proportion of males ranged from 41% to 43%, with no significant differences in the sex ratio over the three years. The prevalence of comorbid anxiety was approximately 10% over the three years (10.6%, 2010; 12.6%, 2011; 10.7%, 2013).
Table 1
Demographics of subjects with bipolar disorder

Data are presented as number (%).
SD = standard deviation.
aComorbid anxiety disorders: the patient visited a clinic or hospital at least once with a diagnosis code of neurotic, stress-related, or somatoform disorder (F40.0–F48.9); bManic: the patient visited a clinic or hospital at least once with a main diagnosis code of manic episode (F30), hypomanic episode (F31.0), manic episode without psychotic symptoms (F31.1), or manic episode with psychotic symptoms (F31.2). Depressive: the patient visited a clinic or hospital at least once with a main diagnosis code of mild or moderate depression (F31.3), severe depression without psychotic symptoms (F31.4), or severe depression with psychotic symptoms (F31.5). Other: the patient visited a clinic or hospital at least once with a main diagnosis code of mixed episode (F31.6), currently in remission (F31.7), other bipolar affective disorder (F31.8), or unspecified bipolar disorder (F31.9).
![]()
The annual prescription rates of ADs for all patients with bipolar disorder were 27.4% (2010), 30.4% (2011), and 33.7% (2013). The rates were 52.1% (2010), 45.8% (2011), and 50.9% (2013) in patients with bipolar depressive episodes (F31.3, F31.4, and F31.5); 16.6% (2010), 19.7% (2011), and 22.3% (2013) in patients with manic episodes (F30, F31.0, F31.1, and F31.2); and 24.1% (2010), 29.5% (2011), and 32.3% (2013) in patients with other episodes (F31.6, F31.7, F31.8, and F31.9). In patients with bipolar disorder, the annual prescription rate of ADs gradually increased over the 3-year period (P < 0.001).
Among patients with bipolar disorder, ADs were prescribed for 92 (45.8%, 2010), 113 (47.1%, 2011), and 150 (55.8%) in patients with comorbid anxiety disorders and for 460 (25.3%, 2010), 506 (28.1%, 2011), and 733 (31.1%, 2013) patients who had not been diagnosed with comorbid anxiety disorders. In all three years, the AD prescription rate was significantly higher (P < 0.001) in patients with comorbid anxiety disorders (45.8%–55.8%) than in patients without comorbid anxiety disorders (25.3%–31.1%).
Comparison of demographics between AD users and non-users
The mean age was 46.0 years (SD, 17.71; 2010), 43.4 years (SD, 16.91; 2011), and 44.1 years (SD, 17.00; 2013) in AD users, and 44.2 years (SD, 16.16; 2010), 44.0 years (SD, 16.88; 2011), and 46.5 years (SD, 17.47; 2013) in non-users (Table 2). The mean age of 2010 and 2013 was significantly different (P < 0.05) between AD users and non-users, but the tendency was the opposite. The proportion of males was 46.3% (2010), 44.6% (2011), and 43.5% (2013) in AD users and 34.8% (2010), 35.9% (2011), and 36.8% (2013) in non-users, with significant female predominance in AD users in all three years (P < 0.001). Presence of comorbid anxiety disorder was significantly higher in AD user group in all three years (P < 0.001).
Table 2
Comparison of demographics between AD users and non-users

Data are presented as number (%)
SD = standard deviation, AD = antidepressant.
aP < 0.05 compared with non-users; bP < 0.001 compared with non-users; cComorbid anxiety disorders: the patient visited a clinic or hospital at least once with a diagnosis code of neurotic, stress-related, or somatoform disorder (F40.0–F48.9).
![]()
Patterns of AD prescriptions
The annual prescription rate for all patients with bipolar disorder was 7.04%–7.90% for AD monotherapy, 8.90%–12.91% for AD + APS, 9.35%–9.76%% for AD + MS, and 10.83%–12.64% for AD + APS + MS (Table 3). The prescription rate of AD + APS tended to increase over the three years (P < 0.001). The average number of prescription days per year was 55.71–67.75 for AD monotherapy, 82.73–111.77 for AD + APS, 93.34–109.10 for AD + MS, and 112.21–118.50 for AD + APS + MS. The average number of prescription days per year for AD + APS tended to increase gradually over the three years (P = 0.001), but AD alone, AD+MS, and AD+MS+APS did not.
Table 3
Patterns of ADs prescription in patients with bipolar disorder

Data are presented as number (%)
AD = antidepressants; APS = antipsychotics; MS = mood stabilizers.
aSum of number of days that the pattern was prescribed in a year/total number of patients prescribed with the pattern.
![]()
Number of patients, mean number of days, and mean daily dose of ADs
Table 4 shows the number of patients, mean daily dose, and mean number of prescription days per year for individual ADs. Escitalopram was prescribed most frequently in all three years, and fluoxetine (2010 and 2013) and bupropion (2011) were the next most frequently prescribed ADs.
Table 4
Number of patients, average number of prescription days per year, and mean daily dose of antidepressants†
![]()
The mean duration of bipolar depressive episodes was 146.16 days (SD, 122.92; 2010), 135.90 days (SD, 117.14; 2011), and 152.53 days (SD, 121.53; 2013). For these episodes, ADs were prescribed for 119.59 days (SD, 108.72; 2010), 115.60 days (SD, 106.36; 2011), and 121.98 days (SD, 108.01; 2013). There were no significant differences in the mean duration of bipolar depressive episodes (P = 0.384) and mean days of AD prescription (P = 0.851) over the three years.
DISCUSSION
The 1-year prescription rate of ADs was 27.3%–33.6% for all patients with bipolar disorder, 45.8%–52.1% for patients with bipolar depressive episodes, 16.6%–22.3% for patients with manic episodes, and 24.1%–32.3% for patients with other episodes, including remission. In a study of AD prescriptions based on nationwide prescription data, AD prescription rates for patients with bipolar disorder were reported to be approximately 40%–60%, according to mood states,11 and up to 74% in one study of inpatients with bipolar depression.23 The prescription rates of ADs in this study were similar to those in previous studies. The rate of AD prescription during manic episode was about 20%. It was also reported in previous study as 40% of patients with a current manic or mixed episode were given ADs,11 in contrast to guidelines. Since clinicians often overlook the diagnostic coding, it is possible that a patient switched from mania to depression would have been wrongly coded as mania, as the previous diagnosis is carried forward. This could be reason for the high rate of ADs prescription during manic phase.
ADs were prescribed for about half of patients with bipolar depression and annual prescription rate was increased over the 3-year period. The latest guidelines show changes in treatment strategies in bipolar depression, based on relatively weak efficacy of ADs in bipolar depression.24 The Canadian Network for Mood and Anxiety Treatments and ISBD 2018 guidelines led to the change from the last guidelines, which previously recommended adjunctive use of ADs (selective serotonin reuptake inhibitors or bupropion) with an atypical APS or lithium/divalproex as one of the first-line treatment, is now considered a second-line treatment.25 Recent expert consensus-based domestic guidelines for treatment of bipolar disorder (Korean Medication Algorithm Project for Bipolar Disorder [KMAP-BP] 2018, Fourth Revision) also recommend the adjuvant use of ADs as the second-line strategy.10 Our results are the data from 2010 to 2013, prescribed according to the previous guidelines of adjuvant AD treatment as the first treatment strategy in bipolar depression. The enduring, treatment-resistant nature of bipolar depression could be the reason for discordance with current guidelines.
The mean duration of AD treatment was 116–122 days per year, which was over 80% the number of days of depressive episodes. The duration of AD treatment for bipolar depression is also a controversial issue. Some studies have reported that maintaining treatment with ADs after remission delays relapse of depressive episodes and lowers the severity of depression,2627 thus providing evidence to support recommendations for long-term maintenance with ADs. Other studies have concluded that ADs should be used in the short term to minimize the risk of manic switch.2829 In the 2013 ISBD task force report, patients with a history of relapse after withdrawal of AD treatment are considered for AD maintenance therapy, but the level of evidence is not high.2 However, depressive and remission phases of bipolar disorder were not specified in the present study; therefore, distinguishment of the purpose of AD prescription between acute phase treatment and maintenance treatment is unclear.
The prescription rate of ADs was significantly higher for patients with bipolar disorder with comorbid anxiety disorder than for those without comorbid anxiety disorder, as shown in a previous study (44% vs. 33%).12 The rate of comorbid anxiety disorders is reported to be approximately from 25% to over half of the lifetime prevalence in patients with bipolar disorder. 1230 The coexistence of anxiety disorders is associated with a shorter duration of euthymia, a higher frequency of psychotic symptoms, more hospitalizations, a higher risk of suicide, poorer quality of life, and overall greater severity of bipolar disorder.1231 In the present study, the prescription rate of ADs may be higher for patients with comorbid anxiety disorders because the severity of bipolar disorder may be higher in these patients, not because the AD is used as the first-line treatment for anxiety disorder.13 However, because this study is based on prescription data, the results should be interpreted cautiously. The prevalence of comorbid anxiety disorders in patients with bipolar disorder was approximately 10% in this study, which was much lower than that in the general population of patients with bipolar disorder.1230 The short observation period and the use of diagnoses based on claim data may have contributed to the lower prevalence rate observed in this study.
The proportion of women was significantly higher in AD users than non-users in all three years, as seen in previous study. Women experience depressive episodes more often than men. Bipolar II disorder, which is predominated by depressive episodes, also appears to be more common in women than men.32 This could be the reason for higher female predominance.
The use of ADs with concomitant atypical antipsychotic drugs tended to increase gradually over the three years of this study. Atypical APS have been shown to have a mood-stabilizing effect in the acute phase of depression, as in acute phase mania in bipolar disorder.23 Olanzapine has proved to be effective in acute bipolar depression when used alone or in combination with fluoxetine.33 Quetiapine has been shown to be superior to lithium and paroxetine for the treatment of bipolar depression3435 and has been approved for maintenance treatment in bipolar disorder.36 Recent meta-analysis studies have shown that quetiapine alone is effective in preventing recurrence of mania and depression, compared with lithium or valproate.37
Based on these findings, atypical APS are currently being recommended as the first-line treatment for bipolar depression,23 and an increased preference for monotherapy with atypical APS for the treatment of bipolar depression was also reported in the fourth revision of KMAP-BP.10 The use of atypical APS in bipolar disorder is increasing due to their wide therapeutic range and stable tolerance compared with MS.12 In this study, the increasing use of atypical APS combined with ADs seems to reflect this tendency.
The high frequency of escitalopram prescription was prominent in all three years. This is in line with the results of the Questionnaire of the Review Committee for the Development of the 2018 Korean Version of the Bipolar Disorder Treatment Guidelines.10 In general, there are no significant differences in efficacy between different selective serotonin reuptake inhibitors, but they may have different clinical effects due to different profiles in pharmacokinetics, pharmacodynamics, and side effects.38 A meta-analysis of randomized, controlled trials in patients with major depressive disorder demonstrated that escitalopram and sertraline have greater efficacy and tolerability than other ADs.39 Although there are no studies on the efficacy and tolerability of individual drugs of the same class of ADs in patients with bipolar disorder, the preference for certain ADs in the treatment of bipolar disorder may be an extrapolation from experiences with major depression.
Fluoxetine and bupropion were the most frequently prescribed ADs after escitalopram. The lower risk of destabilization or affective switch, compared with tricyclic ADs or serotonin-norepinephrine reuptake inhibitors,2 could be the reason for the preference.
Most tricyclic ADs, except clomipramine, were prescribed at less than the usual minimum AD therapeutic dose. Conversely, all selective serotonin reuptake inhibitors, i.e., bupropion, duloxetine, milnacipran, mirtazapine, trazodone, and venlafaxine, were used within the range of usual AD therapeutic doses for depression40 in all three years. This suggests that most tricyclic ADs may have been used as hypnotics or anxiolytics, rather than for their AD effects.
Our study has several limitations. First, because our dataset is based on claim data rather than medical records or structured interviews, a discrepancy between the clinical characteristics of the actual patients and the diagnostic codes may exist. We included main diagnostic codes only in the analysis to reduce discrepancies. Second, the observation period was limited to one year, preventing the investigation of bipolar disorder characteristics with a long clinical course. Third, there was no distinction between bipolar types I and II, a subdivision used in the ‘Diagnostic and Statistical Manual of Mental Disorders.’ However, given that global treatment guidelines suggest very similar treatments for both subtypes of the disorder, this is unlikely to affect the generalizability of our findings. Differences between drug prescriptions according to clinical features and severity of the illness remain uninvestigated. Fourth, some ADs that were probably used for their hypnotic/anxiolytic effects were included in the analysis. However, we excluded low doses of trazodone and tricyclic ADs, which was the most commonly prescribed AD for sleep.
Despite these limitations, this is a large-scale, population-based study that represents the entire domestic population of patients with bipolar disorder, free from subject selection bias and loss to follow-up. All psychiatric prescription data, regardless of the type of medical institution, were included. To the best of our knowledge, this is the first study to analyze recent trends in the prescription of ADs to patients with bipolar disorder. Further investigations with longer observation periods and specified criteria to reflect the clinical characteristics of the patients are needed.
 XML Download
XML Download