

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cerebral microbleeds (CMBs) are small brain hemorrhages with tiny focal points of low-intensity detected in T2-weighted gradient-recalled echo or susceptibility-weighted magnetic resonance imaging (MRI).1 Histologically, CMBs are focal leakages of hemosiderin from small vessels affected by lipohyalinosis or arteries affected by amyloid deposition.12 CMBs are associated with cerebrovascular risk factors (age, hypertension, and diabetes),34 and they are frequently discovered in patients with hemorrhagic or ischemic stroke, as well as in those with cognitive dysfunction, including mild cognitive impairment or Alzheimer's disease.5
These associations have also been reported in patients with Parkinson's disease (PD). Older age and white matter changes were associated with CMBs in PD patients.6 Moreover, CMBs were more commonly observed in patients with PD dementia than cognitively normal PD patients or cognitively normal control subjects.78 However, a direct association between CMBs and PD, especially without cognitive dysfunction, has not been fully elucidated to date. Hence, in this study, we investigated the association between CMBs and PD by making a comparison of the prevalence, number, and location of CMBs between non-demented PD patients and control subjects who were matched for age, sex, and hypertension.
METHODS
Participants
We enrolled newly diagnosed PD patients without dementia between October 2010 and March 2016 in our movement disorders unit at Seoul National University Bundang Hospital, which is a tertiary, nationwide referral-based hospital. Patients undergoing brain imaging studies, including 3-Tesla brain MRI and 123I-2β-carbomethoxy-3β-(4-iodophenyl)-N-(3-fluoropropyl)-nortropane single photon emission computerized tomography (123I-FP-CIT SPECT) imaging, were followed up by an experienced movement specialist. Based on regular follow-up and neuroimaging studies, clinical diagnosis of PD was made according to the diagnostic criteria.9 After the initial clinical diagnosis and neuroimaging, follow-up care was continued in all patients. In this study, we included PD patients without dementia. All PD patients were screened for cognitive function by detailed history taking, Korean version of mini-mental state examination (K-MMSE), and Korean version of Montreal cognitive assessment (K-MoCA). Patients without subjective cognitive dysfunction via history taking, and those with scores within the normal range (K-MMSE score higher than −1 standard deviation below the mean of normative value, K-MoCA score above the cutoff value of mild cognitive impairment) were included for final analysis.1011
For comparison, age-, sex-, and hypertension-matched subjects with no signs of neurological disorders were randomly selected from a pool of 9,106 health-check examinees who underwent brain MRI as a part of a routine health-check examination at our hospital during the same period.
Classification of PD subtypes
All PD patients were measured using Unified Parkinson's Disease Rating Scale (UPDRS) and Hoehn and Yahr stage (HY stage) at the time of neuroimaging, and the postural instability gait scores and tremor scores were calculated. Postural instability gait scores were calculated by the mean score of 5 items: history of falling, freezing, and difficulty walking, as well as exam results of gait and postural instability. Tremor scores were calculated by the mean score of 9 items: history of right and left arm tremor, resting tremor of head (face, lips, or chin), all 4 limbs, as well as exam results of action or postural tremor in both arms. The tremor dominant (TD) group was defined as patients with a ratio of mean tremor score/mean postural instability gait score greater than or equal to 1.5; the postural instability-gait disturbance (PIGD) group included all patients with a ratio of less than or equal to 1.0; and the rest were defined as intermediate.12
Clinical information regarding vascular risk factors
Hypertension was diagnosed using the criteria and methodology set by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (a consistent average of two or more blood pressure measurements on two or more visits, systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg), history of treated hypertension, or current antihypertensive therapy.13 Diabetes mellitus was diagnosed using the standard criteria (hemoglobin A1c ≥ 6.5%, fasting plasma glucose ≥126 mg/dL, or postprandial 2-hour plasma glucose ≥ 200 mg/dL), history of treated diabetes mellitus, or current anti-diabetic medications.14 Hyperlipidemia was defined as elevated plasma cholesterol ≥ 240 mg/dL, history of treated hyperlipidemia, or current lipid-lowering therapy.15 Prior history of ischemic heart disease and stroke was obtained from history taking and the past medical record. Body mass index (BMI) was calculated as body weight in kilogram divided by the square of height in meters. We collected the subjects' smoking history as non-smoker, ex-smoker, or current smoker.
Imaging protocol
MRI was performed at 3-Tesla (Achieva and Ingenia; Philips Healthcare, Best, the Netherland) using a 32-channel sensitivity encoding (SENSE) head coil. Patients underwent axial T2-weighted imaging (T2-WI), axial fluid-attenuated inversion recovery (FLAIR) imaging, and T2*-gradient recalled echo (T2*-GRE) imaging. The parameters for MRI were as follows: T2-WI, repetition time (TR) 3,000 msec, echo time (TE) 80 msec, field-of-view (FOV) 185 mm × 230 mm, acquisition matrix 400 × 320, slice thickness 5 mm; FLAIR, TR 11,000 msec, TE 125 msec, inversion time 2.5 sec, FOV 185 mm × 230 mm, acquisition matrix 370 × 260, slice thickness 5 mm; and T2*-GRE, TR 800 msec, TE 18 msec, flip angle (FA) 23 degree, FOV 185 mm × 230 mm, acquisition matrix 256 × 256, slice thickness 5 mm.
MRI analysis
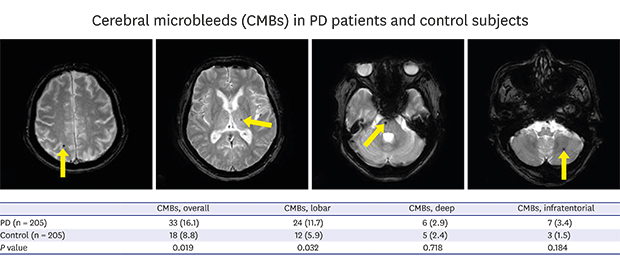
Two readers, who were blinded to the clinical information, independently assessed all MRIs; the presence of CMBs and small vessel disease (SVD) burden were measured (Fig. 1). CMBs were defined as small (3 to 10 mm), homogeneous, round foci of low signal intensity on GRE images in the cortico-subcortical junction, basal ganglia, thalamus, brainstem, and cerebellum. CMB-mimics—calcium and iron deposits in the basal ganglia, flow voids of blood vessels, volume artifact, and cavernous malformation—were excluded.16 The locations of CMBs were as follows: lobar area, including cortical and subcortical areas of the frontal, temporal, parietal, and occipital lobes; deep area, including basal ganglia and thalamus; and infratentorial area, including the brainstem and cerebellum.
Fig. 1
CMBs and other features for SVD score. (A-D) The presence of one or more CMBs scored 1 point in the SVD score. (A) The CMBs, located in high right parietal cortex, (B) left thalamus, (C) right pons, and (D) left cerebellum, are indicated by arrows. (E-G) In addition to the CMBs, each of the following; (E) existence of lacunes (indicated by the arrow), (F) white matter changes with periventricular Fazekas scale 3 and/or deep white matter Fazekas scale from 2 to 3, and (G) moderate-to-severe perivascular spaces (indicated by arrows) in the basal ganglia, earned 1 point in the SVD score.
CMB = cerebral microbleed, SVD = small vessel disease.

The presences of lacunes, white matter hyperintensities (WMH), and perivascular spaces were measured, and SVD burden on MRI was scored on a scale from 0 to 4 (SVD score), according to the presence of the following: presence of one or more CMBs in GRE images, presence of one or more lacunes, presence of confluent deep WMH (Fazekas score 2 or 3) or irregular periventricular WMH extending into the deep white matter (Fazekas score 3) in FLAIR images, and presence of moderate-to-severe (grade 2 to 4) periventricular space in the basal ganglia in T2-WI.171819 The SVD score on 3 of the 4 items—except CMB score—was also measured.
Statistical analysis
The clinical findings were compared using Student's t-test, one-way analysis of variance, and χ2 test for parametric data. Mann-Whitney U test, Kruskal-Wallis test, and Fisher's exact test were used for non-parametric data. Bonferroni correction was used for multiple comparison analyses. Binary logistic regression was used to estimate the odds ratio (OR) adjusted for age, sex and hypertension. The inter-observer agreement was tested using Cohen's κ statistics. P values of less than 0.05 were considered statistically significant. Statistical analyses were performed using SPSS software (version 22.0; SPSS, Chicago, IL, USA).
RESULTS
Clinical characteristics of the subjects
A total of 1,214 patients were diagnosed with PD during the study period. Among them, 205 (114 men and 91 women) PD patients, including 123 PIGD, 56 TD, and 26 intermediate subtypes, showed preserved cognitive function during the screening process, and were eligible for the study (Table 1). All PD patients showed a decreased uptake of the unilateral or bilateral putamen in 123I-FP-CIT SPECT.
Table 1
Clinical characteristics of PD patients and control subjects

Data are presented as means ± standard deviation (range) or number (%).
PD = Parkinson's disease, PIGD = postural instability-gait disturbance, BMI = body mass index, MRI = magnetic resonance imaging, SVD = small vessel disease, UPDRS = Unified Parkinson's Disease Rating Scale, HY stage = Hoehn and Yahr stage, K-MMSE = Korean version of mini-mental state examination, K-MoCA = Korean version of Montreal cognitive assessment, CMB = cerebral microbleed.
aAs the presence of CMBs is a component of SVD score, the score which subtracted CMBs score from the SVD score is presented.
There were no significant differences in the clinical characteristics between PD patients and control subjects, except a higher SVD score in those with the PIGD subtype compared with the controls. In a comparison among PD subtypes, PIGD showed higher mean age, progressed periventricular WMH, higher SVD score, UPDRS score, and HY stage than the other subtypes (Supplementary Table 1).
CMBs among subjects
Among 410 subjects, (205 patients and 205 controls), 51 subjects were determined to have CMBs. The initial inter-observer agreement with respect to the presence of CMBs was 97.2% (κ = 0.87; P < 0.001). CMBs were more frequently found in PD patients (33 out of 205, 16.1%) than in controls (18 out of 205, 8.8%), with an adjusted OR of 2.126 (Table 2); the PIGD subtype accounted for most of the difference (21.1% vs. 8.9%, with an adjusted OR of 2.759). Regarding the location of CMBs, there was a significant difference only in the lobar area (OR of 2.234; P = 0.032) between PD patients and controls; no significant difference was found in other locations. The PIGD subtype showed the same result as the entire PD-patient group. CMBs in patients with TD and intermediate subtypes were not different from controls (Supplementary Table 2). In comparisons among the PD subtypes, CMBs seemed to appear in PIGD type more frequently than in other subtypes, without statistical significance. The mean numbers of CMBs in CMB-positive subjects were not different between PD patients and controls, and in between PD subtypes.
Table 2
Existence of CMBs in PD patients and control subjects

Vascular risk factors and MRI features according to CMBs
We compared the vascular risk factors, MRI features, and clinical profiles among PD patients—particularly between those with and without CMBs (Table 3). PD patients with CMBs, compared with those without CMBs, showed a greater frequency in hypertension, greater intensity of WMHs in the deep white matter, higher HY stage, and higher SVD scores, with or without microbleeds score. We also made the same comparisons between PD patients with lobar CMBs and those with CMBs only in the deep or infratentorial areas. We found no significant differences.
Table 3
Clinical characteristics of PD patients according to microbleeds or lobar microbleeds

Data are presented as means ± standard deviation (range) or number (%).
PD = Parkinson's disease, CMB = cerebral microbleed, BMI = body mass index, MRI = magnetic resonance imaging, SVD = small vessel disease, UPDRS = Unified Parkinson's Disease Rating Scale, HY stage = Hoehn and Yahr stage, K-MMSE = Korean version of mini-mental state examination, K-MoCA = Korean version of Montreal cognitive assessment, NA = not applicable.
aAs the presence of CMBs is a component of SVD score, the score which subtracted CMBs score from the SVD score is presented.
DISCUSSION
In this study, we found that the prevalence of CMBs was higher in PD patients, especially in those with the PIGD subtype, than control subjects matched for age, sex, and hypertension. This difference may mostly be attributed to lobar CMBs, as there were no significant differences with respect to the CMBs in other areas between PD patients and controls. Among PD patients, the PIGD subtype seemed to show a higher frequency of CMBs than the other subtypes; however, this was without statistical significance. This study reports a higher frequency of CMBs in non-demented PD patients compared with control subjects.
CMBs have various pathologic features and different patterns of etiology, depending on their location. Lobar CMBs tend to be associated with amyloid burden, while deep or infratentorial CMBs are made from lipohyalinosis and tend to be associated with hypertensive disease or vascular risk factors.520 Based on this pathophysiologic difference, it is possible to assert that patients with PD might have advanced degree of amyloid pathology than controls, although CMBs were only found in a portion of PD patients. In particular, patients with the PIGD subtype showed a significantly higher frequency of CMBs than controls. This implies that the degree of amyloid pathology may be different depending on the motor subtype.
The association between amyloid deposition and cognitive impairment in PD patients has been well established.21 To date, a direct association between amyloid pathology and synucleinopathy has not been determined, despite the promotion of alpha-synuclein aggregation by the beta-amyloid peptides in a previous experimental study.22 Rather, it would be reasonable to consider amyloid pathology and synucleinopathy as products of a certain pathologic process.
Inflammation may provide an explanation of the relationship between amyloid pathology and synucleinopathy. Inflammatory responses seem to have an influence on amyloid angiopathy. Amyloid deposits activate complement and inflammatory cytokines, causing microglial activation and neuronal damages.23 Accumulation of amyloid deposits could also cause cerebrovascular constriction, which seems to be mediated via pro-inflammatory mechanism with a production of vasoactive eicosanoids (prostaglandin E2 and F2α).24 Such inflammatory processes might influence the formation of CMBs. Previously, proinflammatory cytokines were increased in subjects with CMBs (both in lobar and deep areas) compared with those without CMBs,25 and cortical microbleeds were shown to cause inflammatory responses in the brains of mice.26
Furthermore, inflammation can also explain the neurodegeneration in PD patients.27 In postmortem studies of PD, astrocytosis, microgliosis, and lymphocyte infiltration were found in the substantia nigra.2829 Moreover, proinflammatory cytokines were increased in the substantia, striatum, and cerebrospinal fluid of patients with PD.30 These findings support the notion that inflammation may be an important process for the development of PD.
This study has several limitations. First, we were unable to examine the cognitive function in greater detail than using K-MMSE and K-MoCA. However, we applied the strictest inclusion criteria using K-MMSE and K-MoCA to determine preserved cognitive function; hence, our study population could be regarded as free from dementia. Second, although the prevalence of CMBs in the PIGD subtype of PD was more than twice of that in other subtypes, which might reflect a difference in a pathologic process according to the manifestation of PD, we were unable to find a significant difference in the prevalence of CMBs among PD subtypes. This might be due to the small number of subjects in our study. Further study is needed with larger number of subjects in the future. Third, we did not evaluate the presence of orthostatic hypotension or apolipoprotein E genotype, which are risk factors of CMBs in PD.531 Finally, our study was based on MRI analysis, thus further study using pathological confirmation should be done.
In summary, we found that CMBs—especially in the lobar areas—were more frequent in patients with the PIGD subtype of PD than the controls with similar vascular risk factors. Future study investigating the role of CMBs is needed.
 XML Download
XML Download