

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The United Nation's Sustainable Development Goals (SDGs), which inherited the Millennium Development Goals (MDGs), include “universal and equitable access to safe and affordable drinking water” and “adequate and equitable sanitation and hygiene.”1 These goals mean that a safe drinking water supply, adequate sanitation facilities, and good hygiene are essential to maintaining human health and socioeconomic development.23 Intestinal infectious diseases with diarrhea caused by ingestion of unsafe drinking water are the major cause of death in children in low-income countries.4 The level of sanitation associated with sewage treatment represents the national capacity for adequate waste management and supply of safe drinking water.5 Handwashing for good hygiene after contact with feces acts as an important barrier to the spread of fecal-orally transmitted diseases and reduces the secondary transmission of pathogens.6 Because of these advantages, handwashing with soap is an essential element for health care and disease control.
The World Health Organization (WHO) estimated that the population attributable fraction (PAF) of diarrheal disease due to risk factors such as inadequate drinking water, sanitation, and hygiene (WASH) is more than 25% in a report assessing the global environmental burden of disease.7 In the global burden of disease (GBD) study conducted by the Institute for Health Metrics and Evaluation (IHME), the PAF of deaths caused by risk factors such as unsafe water, sanitation, and handwashing in the Republic of Korea (Korea) was estimated to be 21.7% (15.9%–27.1%) for diarrheal disease and 19.9% (15.4%–24.4%) for intestinal infectious diseases.8 However, the WHO's estimates did not provide any results for subcategories of risk factors or for each country. In addition, the IHME estimates for Korea that the PAF of deaths due to risk factors such as unsafe water and sanitation is 0, and the PAF from not washing hands is presented using old data. The WHO did not calculate the value of the PAF of inadequate drinking water and sanitation facilities in high-income countries of all regions, and the IHME suggested a value of 0 in Korea based on its being a Western-Pacific high-income country.89 The results of previous studies indicate that the PAF and burden of disease caused by inadequate WASH are mainly focused on low-income and middle-income countries.49 However, even in high-income countries, low-income families living in harsh environments suffer from diseases caused by inadequate WASH. Some households in rural areas of Korea still have places where sewage facilities are not available.10
In studies involving countries around the world, there is a limitation in estimating the burden of disease from inadequate WASH due to a lack of representative data sources. In Korea, it is possible to present detailed research results because data such as the number of people consuming a specific type of drinking water, the results of drinking water quality inspection, the water supply and sewerage coverage area, and National Handwashing Survey results are readily available. In this study, we aimed to estimate the burden of disease due to inadequate WASH in Korea.
METHODS
The process of estimating the disease burden attributable to inadequate drinking WASH takes several steps. We have presented a flow chart (Fig. 1).
 | Fig. 1Flow chart for estimating disease burden from inadequate drinking WASH in Korea.WASH = water, sanitation, and hygiene, ICD-10 = International Classification of Diseases and Related Health Problems 10th Revision, YLL = years of life lost, YLD = years lived with disability, DALY = disability-adjusted life years, PAF = population attributable fraction.
|
Exposed population and the relative risk
The relative risk (RR) of disease from inadequate WASH was determined by using IHME GBD study data that showed the results according to the level of each category of WASH after applying WHO methodology.4691112 The proportion of the population using inadequate drinking water was estimated based on the proportion of the population using a piped-water supply and the proportion of households depending on unsafe drinking water. The RR for inadequate drinking water was derived from studies that assessed the risk of disease according to drinking water treatment methods (Supplementary Table 1).11 Sanitation was assessed by taking into account the proportion of the population living in areas where sewage treatment is not conducted. The RR for sanitation was derived from studies that estimated the risk of disease according to the type of sewage treatment method (Supplementary Table 2).11 The hygiene level was assessed based on the percentage of the population who washed hands properly with soap and water after using the toilet and the RR associated with hand washing behavior was applied (Supplementary Table 3).11 The RRs related with inappropriate WASH applied in this study can be found in the supplementary appendix of Reference 11.11
Theoretical minimum-risk exposure level
In GBD studies, theoretical minimum-risk exposure level (TMREL) is the risk exposure that is both minimizes risk in the exposed population and theoretically possible.11 Therefore, TMREL is set differently depending on the risk factors. The TMREL for unsafe water is defined as the risk to health effects that may occur in household members who have access to high-quality piped water that has been boiled or filtered before drinking water. The TMREL for unsafe sanitation is defined as the risk to health effects that may occur in household members who have access to a sanitation facility with sewer connection. A sanitation facility with sewer connection included flush toilets and any toilet with connection to the sewer or septic tank. The TMREL for unsafe hygiene is defined as the risk to health effects that may occur in household members who engaging in handwashing with soap practices after any contact with excreta.
PAF
The PAF was estimated according to the following formula by applying the exposure ratio of each population to the RR for each exposure level of risk factor.

Where Pi is the proportion of the exposure population at exposure level i, RRi is the RR at exposure level i, and n is the total number of exposure levels.
The following formula was used to calculate the PAF due to inadequate WASH as a cluster of the risk factors. The interval estimates for the total PAFs incorporating the three risk factors were calculated using Monte Carlo simulation.

Where r is the individual risk factor and R is the total number of risk factors considered in the cluster. Each risk factor in the formula is assumed to be independent and non-interacting.
Mortality and morbidity data
The range of diarrhea and intestinal infections due to inappropriate WASH, included in the calculation of disease burden in this study, was based on criteria classified according to the International Classification of Diseases and Related Health Problems 10th Revision (ICD-10). In 2013, the number of premature deaths was calculated from entries in the national death registry for which the cause of death was defined as intestinal infectious disease (A00–A09), acute hepatitis A and E (B15, B17.2), and helminthiases including schistosomiasis, hookworm diseases, ascariasis, and trichuriasis (B65, B76, B77, B79) (Supplementary Table 4). To calculate the burden of disease, national health insurance statistic were used to calculate the actual number of patients treated with the above-mentioned disease code in 2013.
Disability weights and severity distribution of diseases
WHO values were used for disability weights according to the health status of patients with intestinal infections caused by inadequate WASH in Korea.13 Disease severity for diarrheal and intestinal infectious disease-related health status was classified as mild for outpatients and moderate for hospitalized patients. In the case of viral hepatitis A and E, the outpatient cases were classified as moderate and the hospitalized patients were classified as severe.
Burden of disease due to inadequate WASH
Disability-adjusted life years (DALY) is a single health indicator of disease burden consisting of the sum of years of life lost (YLL) and years lived with disability (YLD). The YLL for each disease was calculated by multiplying the number of cause-specific deaths by the loss of standard life expectancy due to premature death according to the sex and age of the individual at the time of death. The basic formula of YLL was the following for a given cause (c), sex (s), and age (a) in a particular time period (t). YLD is calculated by multiplying the disability weight corresponding to the number of prevalent morbidities according to the severity of the cause of disease in a particular time period (t). The basic formula of YLD is the following for a given cause (c) and health state (h):
Where N(c, s, a, t) is the number of deaths due to the cause c for the given age a and sex s in time t, L(s, a) is the loss of standard life expectancy due to cause c of premature death at age a for sex s, DW(c, h, t) is the disability weight for cause c in health states h, and P(c, h, t) is the number of prevalent cases for cause c in health states h in a particular time period t.
The burden of disease attributable to each risk factor (AB) was calculated by multiplying the PAF by total DALY as the burden of diarrheal and intestinal infectious disease (B).
RESULTS
The Korean population distribution for inadequate WASH exposure, excess premature deaths, and burden of disease due to inadequate WASH-associated diarrheal and intestinal infectious diseases in Korea were estimated for the base year of 2013. However, in case of a lack of data sources for estimating the probability distribution, the data of adjacent years were used.
Exposure estimates of inadequate drinking water
From the 2010 census questionnaire on drinking water consumption, the percentage of the population consuming safe drinking water was estimated. Tap water and bottled water, which were previously treated or purified to the TMREL, accounted for 80.2% and 13.9%, respectively. The proportion of unqualified well water, groundwater, and unconfirmed water used as drinking water was 2.9%, 2.9%, and 0.1%, respectively (Table 1).14 According to the quality survey for unqualified drinking water types, the inadequacy rate of groundwater was 11.6% and that of well water was 32.1% (Table 2).15 As of 2013, inadequate consumption of drinking water accounted for 1.4% of the total population (713,342 people). Gangwon-do had the highest rate of 3.3% in its administrative area, and Jeju had the lowest rate of 0.1% (Table 3). In the metropolitan area, although the waterworks supply rate was almost 100%, some people still consumed inadequate drinking water. Local areas, including rural areas, had a slightly lower rate of waterworks supply than metropolitan areas and a higher proportion of inadequate drinking water populations.
Table 1
Use of drinking water sources in population census in 2010 in Koreaa
aData source: usage of drinking water (Korean Statistical Information Service, http://kosis.kr/).
![]()
Table 2
Drinking water sources other than waterworks in Korea in 2014a

| Sources | Investigated samples | Exceeding the standard | Proportion of exceeding the standard (%) |
|---|---|---|---|
| Groundwater | 1,331 | 155 | 11.6 |
| Well water | 6,052 | 1,945 | 32.1 |
aData source: soil and groundwater information system (National Institute for Environmental Research, http://sgis.nier.go.kr/sgis).
![]()
Table 3
Estimated population with insecure drinking water in Korea in 2013a
aData source: waterworks statistics (Korean Statistical Information Service, http://kosis.kr/).
![]()
Exposure estimates of inadequate sanitation
In Korea, no one lives in an unimproved sanitation area and 515,722 people, 1.0% of the total population, live in areas with improved sanitation facilities excluding sewer connections. In mega-cities, the sewage treatment rate was 100% and Gyeongsangbuk-do had the lowest rate of 93.8%. The sewage treatment rate in the metropolitan area has reached almost 100%. However, excluding Sejong and Jeju, local areas showed a slightly lower range of 93.8%–99.5% (Table 4).
Table 4
Sewage treatment status in Korea in 2013a
aData source: sewage treatment statistics (Korean Statistical Information Service, http://kosis.kr/).
![]()
Exposure estimates of inadequate hygiene
The RR with respect to hygiene levels reflects the practice of proper handwashing, which reflects the observed prevalence of handwashing with soap and water after using the restroom or being in contact with excreta. Handwashing with soap after using a public restroom was observed in 23.5% of individuals in a Korean National Handwashing Survey in 2013.16
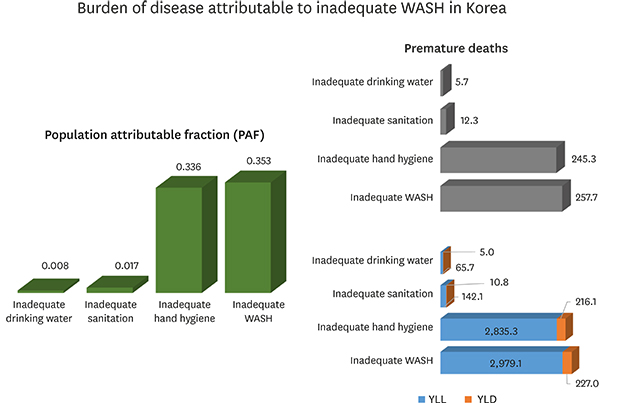
PAF and disease burden attributable to inadequate WASH in Korea in 2013
In Korea, the RRs of contaminated groundwater and inadequate drinking water as wells were applied at a RR (95% confidence interval [CI]) of 1.56 (1.43–1.70), which is one level above the theoretical minimum-risk exposure level. The PAF of diseases due to inadequate drinking water consumption was calculated as 0.008 (0.006–0.010), and the excess mortality was estimated to be 5.7 (4.4–7.1) persons in 2013. The disease burden was calculated as 65.7 (50.6–82.0) DALY for YLL and 5.0 (3.9–6.2) DALY for YLD. The RR for the sanitation-related improved category, which uses a septic tank or private sewage treatment plant for sewage treatment, was 2.71 (2.55–2.88). The PAF of diseases due to inadequate sanitation facilities was calculated as 0.017 (0.015–0.018), and the excess mortality was estimated to be 12.3 (11.2–13.5) persons in 2013. The disease burden was calculated as 142.1 (129.0–155.9) DALY for YLL and 10.8 (9.8–11.9) DALY for YLD. People who do not wash their hands with soap after contact with excreta in Korea accounted for 76.5% of the total population. The RR for the category of no handwashing with soap and water was 1.66 (1.46–1.87). The PAF of disease due to inadequate hand hygiene status was calculated as 0.336 (0.262–0.400), and the excess mortality was estimated to be 245.3 (190.3–292.1) persons in 2013. Disease burden was calculated as 2,835.3 (2,199.8–3,377.0) DALY for YLL and 216.1 (167.6–257.3) DALY for YLD (Table 5).
Table 5
PAF and disease burden attributable to inadequate water, sanitation, and hand hygiene in Korea in 2013

PAF = population attributable fraction, YLL = years of life lost, YLD = years lived with disability, CI = confidence interval, WASH = water, sanitation, and hygiene.
![]()
DISCUSSION
This study estimated the burden of diarrheal and intestinal infectious diseases attributed to inadequate WASH by using the exposure level of risk factors of the Korean population. Exposure to inadequate drinking water is influenced by the number of people drinking water at a lower water quality than provided by waterworks, and an inadequate sanitation level is reflected in the number of inhabitants in areas where sewage treatment facilities are not available. Inadequate hand hygiene reflects the percentage of people who do not wash their hands with soap after contact with human excreta.
In the developed countries, the water supply rate is close to 100% in urban areas, but in rural areas, groundwater is often used as drinking water and there are a few people who use well water as drinking water according to individual preferences. The use of inadequate drinking water increases the likelihood of exposure to waterborne pathogens causing diarrhea and abdominal pain. In rural areas, water quality inspection is carried out periodically on groundwater and well water for the management of drinking water, but a certain level of inadequate water quality has been reported continuously. Inadequate water quality testing results have been reported in which the total colony counts and total coliform, used as indicators of human or animal fecal contamination, exceed the threshold.17 In Korea, approximately 700,000 people use groundwater or well water that has been judged as inadequate drinking water in water quality tests. In particular, when contaminated drinking water was used for cooking in a restaurant or a group reception facility, several patients with water-borne diseases were diagnosed and epidemiological studies were conducted. The contamination of drinking water is closely related to the installation of sewage treatment facilities that provide an inadequate sanitation level. In areas where sewer is unconnected, septic tanks or private sewage treatment facilities can be inadequately treated due to technological inexperience and wrong usage of detention centers. In addition, livestock manure from livestock farming is recognized as a major source of water contamination.1819
In 2013, the average sewage treatment rate in Korea was 99.0%. One percent of the total population is living in areas where individual improved sanitation facilities instead of sewer connections. However, the sewerage penetration rate in urban areas was almost 100%, but 98.3% in rural areas, which is different from urban areas. As a result, approximately 515,000 people live in rural areas where public sewage treatment facilities are not connected.20 In Korea, there is a possibility of gastroenteritis due to contaminated groundwater intake, especially due to the low sewage treatment rate in rural areas and inadequately managed groundwater used as drinking water.21 Studies suggesting that norovirus was detected in approximately 8.7% of the collected domestic groundwater supports this possibility.21 Another study using geographic information systems showed that outbreaks due to norovirus infection occurred in areas with small, low-tech, self-operated sewage treatment plants and poorly treated sewage discharge.22 The detection of hepatitis A RNA in approximately 13% of the pediatric and adolescent patients hospitalized for acute gastroenteritis in Seoul indicates that it has spread through contaminated water or food, resulting in illness in urban areas due to inadequate WASH.23 In addition to acute gastroenteritis, some studies have suggested that contaminated water is a potential risk associated with the spread of aseptic meningitis and hand, foot, and mouth disease.242526
In 2006, the frequency of handwashing with soap after using a public restroom was approximately 17% in the handwashing observational survey conducted in Korea.16 In the survey conducted in 2013, it was 23.5%, which is still low compared with the North American high-income countries (49%) and the European high-income countries (44%).616 A low percentage of handwashing with soap in Korea has contributed to more than 90% of the total burden of diarrheal and intestinal infectious.
The risk of diarrheal and intestinal infectious disease due to inadequate drinking water provided by the WHO and IHME is mainly calculated from data for low- or middle-income countries. Therefore, in developed countries where the water supply rate is approaching 100%, there are limited categories that can be applied to populations using some groundwater or well water as drinking water. In this study, the RR of 1.56 (1.43–1.70), which is just above the TMREL, was applied to Korean population using inadequate drinking water (Supplementary Table 1). Although this RR may be overestimated in Korean context, the applied RR was considered acceptable when considering the result that 12.5% of the mean risk of acute gastroenteritis was attributed to drinking groundwater in a developed country environment.27
For the risk of inadequate sanitation related to the inadequate sewage treatment, the improved category in this study has a RR of 2.71 (2.55–2.88). However, in a meta-analysis that effects of sewerage on diarrhea and enteric infection, the risk with respect to diarrheal disease of the use of septic tank or other facility compare to the introduction of a sewage treatment facility was about 1.28–1.45.28 This gap in RR is believed to be due to conceptual differences in defining improved sanitation facilities. It was due to the difference between the improved facility at the global context by WHO and researchers who judged the use of septic tanks as an improved facility at the Korean context. This shows that considering that Korea is a developed country, the RR applied in this study is likely to overestimate the PAF due to inadequate sanitation, and therefore, the burden of disease can be calculated to be larger than the actual impact.
The RR for no handwashing with soap and water in this study was 1.66 (1.46–1.87). Although the effects of handwashing according to national development level were all protective in preventing disease, the protective effects in developed countries (RR, 0.73; 95% CI, 0.58–0.92) were relatively less effective than those in non-developed countries (RR, 0.66; 95% CI, 0.53–0.82).29 Health damage caused by poor WASH is not only a problem in developing countries but also in developed countries.3031 Intervention studies on handwashing with soap in the United States and Australia have shown a 50% reduction in diarrheal disease, consistent with the results of developing countries.323334 Therefore, although some preventive effects of handwashing with soap have been shown to be more effective in developing countries than in developed countries, the RR for no handwashing with soap and water presented by the WHO is considered to be applicable in developed countries.
Regarding the burden of disease due to inadequate WASH, unsafe drinking water and sanitation associated with sewage treatment are mainly due to the poor environment in rural areas. Environmental improvement in rural areas with a low population density will require policy intervention by the authorities, and therefore, policymakers will need to make a preliminary study of cost-effectiveness. In this regard, the cost-benefit ratio was estimated to be approximately 9.95 (3.36–20.65) for improving the drinking water supply environment in the rural areas in the developed countries of the western Pacific, including Korea. This means that even in developed countries, the health benefits are much greater than the cost of improving the drinking water supply environment.35
Based on the results of the present study, the magnitude of the burden of disease caused by inadequate WASH in Korea was found to be in the order of hand hygiene, sanitation, and safe drinking water. Therefore, to reduce the burden of disease caused by the lack of these, it is necessary to raise awareness related to handwashing with soap and to form good habits through handwashing campaigns and various programs. Next, policy intervention by the authorities is required to improve the environment related to sewage treatment rates in rural areas. Finally, with regard to safe drinking water, it is advisable to use drinking water that is equivalent to the quality of water supplied by waterworks, and it is required to continuously monitor water quality and provide information for the population using groundwater and well water as drinking water.
 XML Download
XML Download