

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The use of central venous catheters (CVCs) is essential for critically ill patients, for those undergoing hemodialysis, and for those with malignancies.1 CVC use has increased in intensive care units (ICUs) over the past decade along with a rise in associated complications.23456 Central line-associated bloodstream infections (CLABSIs) are the most serious complications of CVC use and are a major cause of morbidity and mortality in ICUs in the United States.789
Interventions targeting the insertion and maintenance of CVCs can lead to a decrease in the rate of CLABSI and can have a substantial impact on the overall incidence of ICU-acquired infections.1011 The Korean Nosocomial Infections Surveillance System (KONIS) was established in 2006 by the Korea Center for Disease Control and Prevention and the Korean Society for Nosocomial Infection Control with the aim of improving infection control strategies in ICUs.1213 KONIS reported that the rate of CLABSI in ICUs decreased from 3.40 to 2.33 per 1,000 catheter-days from 2006 through 2013.1214 Previously, surveillance and interventions in Korea related to CLABSIs were mainly targeted to ICUs. However, CVCs are increasingly used outside ICUs as more invasive procedures are performed, especially on immunocompromised and elderly patients. Studies have shown that two-thirds of identified CVCs are in non-ICU patients, which highlights the need for surveillance and infection prevention efforts in that population.910 Therefore, we performed a hospital-wide survey of CLABSIs to evaluate the current situation and develop strategies to reduce CLBASI rates.
METHODS
A single-center prospective study was conducted in a 1,328 bed tertiary hospital in Korea between January 2014 and December 2015. All hospitalized patients with CVCs, including those in ICUs (cardiac, medical, surgical, neurosurgical, neonatal, and emergency) and general wards (non-ICUs), were screened for CLABSIs over the study period. We developed an electronic medical record (EMR)-based surveillance system with which we were able to collect all the information on hospitalized patients with CVCs in 2013, and the system was then applied to CLABSI surveillance in ICUs. Surveillance has been expanded to the entire hospital since 2014. It is carried out by infection control nurses, and all cases were regularly reviewed by infectious disease physicians before case confirmation.
CLABSI was diagnosed using the definitions of the National Health Safety Network (NHSN); excluding infections already present on admission and secondary bloodstream infection (BSI).15 Mucosal barrier injury laboratory-confirmed bloodstream infections (MBI-LCBIs) were excluded from the analyses, because the mechanisms responsible for them, such as translocation of gastrointestinal organisms, are different.1617 CLABSI rates were calculated as cases per 1,000 catheter days, and the device utilization ratio (DUR) was defined as number of catheter-days divided by number of patient-days. The recommendations for prevention of CLABSIs by the Society for Healthcare Epidemiology of America and the US Centers for Disease Control7 were implemented. In addition, periodic feedback regarding CLABSI rates was provided to individual team members and senior administrators.
All the clinical information on CLABSI cases was collected retrospectively from EMRs. Among the data collected were demographic findings, underlying illnesses including Charlson comorbidity index, microbiologic data, and CVC-related data (types, duration of catheterization, and insertion sites).18
Statistical analyses were performed with Student's t-tests and χ2tests or Fisher's exact tests depending on the variable, using IBM SPSS Statistics (version 22.0.0.1; IBM Corp., Armonk, NY, USA). In all analyses, a 2-tailed P value of 0.05 was considered significant.
RESULTS
CLABSI rates
A total of 199 CLABSIs occurred in 168 patients in our hospital over the study period. We identified 45 events of MBI-LCBIs in 36 patients, and 7 of these had both CLABSIs and MBI-LCBIs. After excluding the 45 MBI-LCBIs, 154 CLABSIs in 139 patients were included in the study. Among these, 82 (53.2%) occurred in ICUs and 72 (46.8%) in general wards, with rates of 0.81 and 2.71 CLABSIs per 1,000 catheter days, respectively. The overall DUR was 0.16 (0.45 in ICUs, and 0.14 in general wards).
Characteristics of patients with CLABSIs
Among the 139 patients with CLABSIs, 85 (61.2%) were male, and the mean age was 55.5 ± 23.3 years old. Cardiovascular and cerebrovascular diseases were the most common underlying diseases among the ICU patients, whereas malignancies were the most common among the general ward patients. Of the patients in general wards, 23.9% had underlying haematological malignancies, even though MBI-LCBIs were not included in the study (Table 1).
Table 1
Characteristics of 139 patients with CLABSIs, 2014–2015

Data are presented as means ± standard deviation (range).
CLABSI = central line-associated bloodstream infection, ICU = intensive care unit, LOS = length of stay, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease, AACCI = age-adjusted Charlson comorbidity index.
![]()
Characteristics of the CVCs in CLABSIs
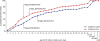
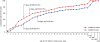
A total of 184 CVCs were placed in the 154 CLABSI events. Most patients (81.8%; 126/154) had only one CVC when the CLABSI occurred, and multiple indwelling CVCs were more frequent in ICUs (29.3%; 24/82) than in wards (5.6%; 4/72). Seventy CLABSI events occurred within one week of CVC maintenance, and non-tunneled catheters were most often associated with these events (68.6%): 48 non-tunneled catheters, 7 tunneled catheters, and 15 peripherally inserted central catheters (PICCs). Tunneled catheters and PICCs were more common (60.5%) among the 114 CLABSIs that occurred more than a week after placement: 44 non-tunneled catheters, 34 tunneled catheters, and 36 PICCs. While the majority (72.2%; n = 78) of CLABSIs in ICUs were associated with non-tunneled catheters, tunneled catheters (44.7%; n = 34) and PICCs (36.8%; n = 28) were more common in wards (Table 2). These findings indicate that CLABSIs tended to occur earlier in ICUs than in wards (Fig. 1); in addition non-tunneled catheters were responsible for most early CLABSIs while the proportion of tunneled catheters increased among late CLABSIs (Fig. 2).
Table 2
Characteristics of 184 CVCs in 154 CLABSIs, 2014–2015

CVC = central venous catheter, CLABSI = central line-associated bloodstream infection, ICU = intensive care unit, PICC = peripherally inserted central catheter, IQR = interquartile range.
![]()

Microbiological data
The microorganisms isolated by blood culture are listed in Table 3. Gram-positive bacteria were the most prevalent both in ICUs and general wards. Coagulase negative staphylococci (CoNS) and Staphylococcus aureus were the most common, representing 52 (31.7%) of the total, and 88.5% and 69.2% of them were oxacillin-resistant, respectively. S. aureus was the most common microorganism isolated, representing 20.7% of the total CLABSIs in general wards, while CoNS was the most frequently isolated microorganism (18.3%), in ICUs. Enterococcus species were the second most frequently isolated microorganisms in both ICUs and general wards. However, there were no statistically significant differences in microorganisms isolated between ICUs and general wards (Table 3).
Table 3
Details of the 164 microorganisms identified in 154 CLABSIs, 2014–2015

Data are presented as number (%).
CLABSI = central line-associated bloodstream infection, ESBL = extended-spectrum beta-lactamases.
![]()
DISCUSSION
Most surveillance and intervention has tended to be focused on CLABSIs in ICUs; and workers have only recently begun to recognize the importance of CLABSI in non-ICUs.12 We found that almost half of all CLABSI events occurred in general wards (non-ICUs) in the two-year surveillance described above. In the United States reported CLABSI rates in non-ICUs have varied, ranging from 0.35 infections per 1,000 central-line days to 5.2 infections per 1,000 catheter-days in major teaching hospitals.1920 The CLABSI rate in our general wards was 0.81 infections per 1,000 catheter day, which is comparable to the rate in the 2013 device-associated module report of the NHSN.21 We found 2.71 infections per 1,000 catheter-days in ICUs, and this rate and that reported by KONIS (2.33 infections per 1,000 catheter-days in 2013) are 2-fold higher than the rate reported by the NHSN; the difference may be related to the fact that the interventions for preventing CLABSIs in Korea are less comprehensive than in the United States.18 Moreover, many of the hospitals that participated in KONIS were large, with over 200 beds, and this may have contributed to an increased severity of illness among the hospitalized patients.
In this study, the median time from placement to CLABSI onset was 9 days in ICUs and 12 days in general wards, which is similar to the 7.5 days in ICUs and 13 days in non-ICUs reported by Klintworth et al.22 It is plausible that the majority of CVCs used in ICUs were non-tunneled, and that this contributed to the early infections (Fig. 2). It is noteworthy that substantial numbers of the CLABSIs associated with non-tunneled catheters or PICCs occurred between 31 and 90 days after CVC maintenance despite the fact these catheters are intended for short-term use for vascular access.23 It will be important to educate healthcare workers to use CVCs appropriate for their expected duration.
Tedja et al.24 conducted surveillance for CLABSIs in a non-ICU and examined morbidity and mortality. They reported that Enterococcus spp. (47 isolates; 26%) were the predominant organisms identified, and that 39 (83%) were vancomycin resistant. Klebsiella species were the second most-commonly isolated organisms, along with almost the same proportion of Candida species (11% and 10%, respectively). The high proportion of patients with hematological malignancy may have influenced those results. In our study, the most commonly identified organisms were CoNS in ICUs and S. aureus in general wards. Enterococcus spp. were the second most commonly identified organisms in both ICUs and general wards, but only one isolate (4%) was vancomycin resistant. Even though there was no statistically significant difference in microorganisms isolated between ICUs and general wards, gram-negative organisms were more common in ICUs and fungi predominated in general wards (Table 3). Patients' comorbidities and the types of CVC employed may have been responsible for these results. Therefore, further studies are required to investigate the relationship between microorganism, type of ward and type of CVC.
Current guidelines regarding CLABSIs are largely based on studies performed on ICU patients with non-tunneled catheters. Recently, Climo et al.9 conducted a large-scale prospective study to identify the prevalence of CVC use among patients both within and outside ICUs. They found differences in the epidemiology of CVC between patients in and outside ICUs: non-tunneled CVCs were more frequent in ICUs, and PICCs in general wards. These results are not directly comparable with ours because our data were collected from CLABSI patients only. Nevertheless, our results are similar in terms of the types of CVC commonly used in ICUs and general wards.
Our study has strength in that we compared the times of onset of CLABSIs and types of causative microorganisms as a function of type of CVC between ICUs and general wards. However, further study is needed of the effect of the site of catheter insertion on CLABSIs.
We are aware of a few limitations of this study. As it was a single-center study, the results should be interpreted with caution and should not be generalized to other hospitals. In addition, they may be biased by the large proportion of patients with severe illnesses, because the study was performed in a tertiary care hospital. In spite of these limitations we believe that the results have important clinical implications. By carrying out hospital-wide surveillance, we found that substantial numbers of CLABSIs occurred in non-ICUs, showing that surveillance is needed in non-ICUs as well as ICUs. In addition, we revealed possible differences between the clinical characteristics, CVCs and causative microorganisms of the CLABSIs in ICUs and in general wards.
In conclusion, CLABSIs are less common in general wards than in ICUs, but they are more often associated with long-term indwelling catheters. Our findings underline the importance of hospital-wide surveillance for CLABSIs, and suggest that approaches to reducing the risk of CLABSIs should be tailored to the type of ward and catheter, and to the associated risk factors.
 XML Download
XML Download