

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mycoplasma pneumoniae (MP) is one of the most common pathogens of community-acquired pneumonia in children and adolescents. It can cause a variety of clinical manifestations, from mild respiratory symptoms to severe fatal pneumonia with extrapulmonary complications.123 Epidemics commonly occur every 3–4 years45; the most recent epidemic was in 2015–2016 in Korea.
Macrolides have long been regarded as the first-line treatment for MP pneumonia in children,6 which has shown excellent effectiveness for many years. However, the incidence of macrolide-resistant M. pneumoniae (MRMP) has recently increased worldwide, especially in Japan and China.789101112 In Korea, the prevalence of MRMP genetically determined by the 23S rRNA gene mutation has gradually increased from 14.7% in 2006 to 56.1% in 2010–2011 and 87.2% in 2015.1314 Patients with MRMP have a longer duration of fever and antibiotic treatment,15 and severe cases of life-threatening pneumonia have been reported in patients with MR strains.16
Given the increase of MRMP, some secondary treatment agents, such as corticosteroids, tetracyclines, and fluoroquinolones, have been considered for the treatment of MRMP pneumonia, although several studies have suggested that macrolides have clinical efficacy for the treatment of MRMP.171819 Tetracyclines, including minocycline and doxycycline, have been reported as alternative agents for children with MRMP.2021 However, they are not recommended for use in patients younger than 8 years of age, because tetracyclines can cause tooth discoloration in children during the periods of osteogenesis and odontogenesis.22 In addition, fluoroquinolones have been associated with a risk of musculoskeletal toxicities, including tendinitis, arthritis, and growth impairment in children.23 Although there is still lack of information on their safety in children, it was reported that there were no clinically detectable adverse events for up to 5 years after treatment with levofloxacin (LFX).24 Some studies have reported the clinical effectiveness of systemic corticosteroids (CST) in the treatment of refractory MP pneumonia, because hyper-reaction of the host immune system may contribute to its pathogenesis.2526 However, CST can also cause several side effects, such as growth disorder, glucose intolerance, and the suppression of the immune system.27
We aimed to compare the therapeutic efficacy of prolonged macrolides (PMCs), CST, doxycycline (DXC), and LFX against macrolide-unresponsive MP pneumonia in children, and to evaluate the safety of CST, DXC, and LFX.
METHODS
Subjects and study design
We retrospectively analyzed the medical records of patients with MP pneumonia aged ≤ 18 years old who were hospitalized at Gil Medical Center between January 2015 and April 2017.
The diagnosis of MP pneumonia was confirmed if all the following conditions were satisfied: 1) signs and symptoms (fever, cough, dyspnea, productive sputum, chest pain, or abnormal breath sounds) of pneumonia; 2) abnormal chest X-ray findings compatible with pneumonia; and 3) identification of MP IgM antibody performed during the illness via enzyme-linked immunosorbent assay.
Among these patients, macrolide-unresponsive MP pneumonia cases were clinically defined as persistent fever ≥ 38.0°C at ≥ 72 hours after macrolide treatment in this study. The macrolide-unresponsive MP pneumonia cases were divided into four groups, PMC, CST, DXC, and LFX. The PMC group was defined as cases treated with PMC without a change of antibiotics. The CST, DXC, and LFX groups were defined as cases with treatment added on (CST) or changed to secondary treatment (DXC, LFX) because of persistent symptoms despite macrolide treatment.
Patients with any of the following were excluded: 1) patients for whom clinical symptoms and radiologic findings were not compatible with pneumonia, despite positive MP IgM; 2) patients with a history of MP infection within the past year; 3) patients whose fever had subsided within 72 hours after macrolide treatment; 4) patients who were prescribed oseltamivir because of proven influenza during hospitalization period; or 5) patients for which a secondary treatment was started ≥ 12 hours after the last time with a fever of ≥ 38.0°C.
The mean duration of administration in the CST, DXC, and LFX groups was 5.9 ± 3.1 days (oral prednisolone dosage of 1 mg/kg/day or intravenous methylprednisolone dosage of 1–2 mg/kg/day), 9.4 ± 3.4 days (at a dosage of 4 mg/kg/day), and 8.2 ± 2.4 days (at a dosage of 10 mg/kg/day).
Data collection and analysis
The collected data included age, sex, hospitalization period, duration of fever (febrile days before macrolide treatment, febrile days during macrolide single treatment, time to defervescence [TTD] after initial macrolide treatment, and TTD after secondary treatment), chest X-ray findings, prescribed antibiotics, extrapulmonary symptoms (hepatitis, skin rash, arthritis, hematologic, and neurological symptoms), oxygen use, intensive care unit (ICU) hospitalization, percutaneous catheter drainage (PCD) insertion, re-hospitalization, and side effects associated with secondary treatments (CST, DXC, and LFX). The chest X-ray findings were from the records read by two radiologists and classified according to the presence of consolidation (lobar or patchy), reticular opacities, pneumonic infiltration, and parapneumonic effusion. In addition, information about mixed infections with other respiratory pathogens identified through multiplexed reverse transcription-polymerase chain reaction (RT-PCR) for respiratory viruses from a nasopharyngeal swab was included.
We compared the TTD after secondary treatment, the use of combined antibiotics, other required treatments and outcomes among the CST, DXC and LFX groups. In addition, we compared the TTD after initial macrolide treatment and the length of hospital stay between PMC group vs. each CST, DXC, and LFX group. To adjust some variables which could affect the fever duration, we performed propensity score (PS) matching analysis.
Side effects such as Cushing appearance and peptic ulcer for CST, tooth discoloration for DXC, and tendinopathy, arthritis for LFX were evaluated for one month after medication.
Statistical analysis
All analyses except PS matching were performed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). The Kruskal-Wallis test or Mann-Whitney test was used for continuous variables such as age, hospitalization period, and duration of fever. The χ2 or Fisher's exact tests were used for categorical variables such as sex, chest X-ray findings, antibiotics, extrapulmonary symptoms, oxygen use, ICU hospitalization, PCD insertion, and re-hospitalization. If the variables were statistically significant when compared among more than two groups, they were further analyzed by Mann-Whitney test, χ2 test or Fisher's exact test for comparing two groups.
We compared the TTD after initial macrolide treatment between PMC group and each secondary treatment group through PS matching to reduce selection bias and to control potential confounding factors. The estimated PS for being assigned to each group was calculated for each patient using multiple logistic regression models with the following covariates: age, sex, radiographic findings, mixed infection with other pathogens. Patients were matched at a ratio of PMC:CST = 2:1, PMC:DXC = 1:1, and PMC:LFX = 2:1, based on a greedy 8-1 digits matching algorithm. This algorithm attempted to match the PMC subjects and the secondary treatment subjects on the first 8 digits of the PS. The PMC subjects that did not match were then matched to secondary treatment subjects on 7 digits of the PS. We processed through the algorithm sequentially to the 1-digit match on the PS. The patients with no corresponding match were excluded. PS matching was performed using SAS 9.1.3 (SAS Institute Inc., Cary, NC, USA). P values of < 0.05 were considered to be statistically significant.
RESULTS
Characteristics of subjects
The total number of subjects who met the inclusion criteria for MP diagnosis within the study period was 1,165. After exclusion by our study criteria, 190 cases (16.3%) of macrolide-unresponsive MP pneumonia were enrolled. Among those, 138 cases were continuously treated with macrolide approximately for 7–14 days, and 32 cases were treated with add-on CST and continuous macrolide. Fourteen and 6 cases were treated with secondary antimicrobial therapy with DXC and LFX, respectively. Two patients were excluded: one patient had improved when administered a combination therapy of corticosteroid and LFX after treatment failure of the add-on of corticosteroid alone; the other patient was treated with corticosteroid and LFX simultaneously.
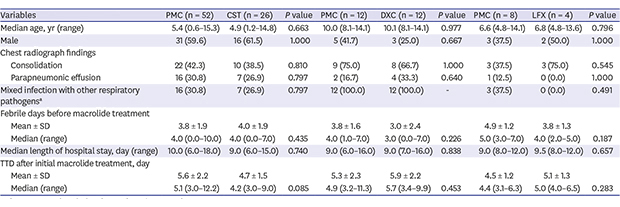
The median age of patients in the PMC, CST, DXC, and LFX groups was 5.2 years old (range: 0.6–16.0), 4.9 years old (range: 1.2–14.8), 10.1 years old (range: 8.1–14.6), and 9.7 years old (range: 4.8–17.0), respectively (P < 0.001). Patients in the DXC group were significantly older than in the PMC and CST groups (P < 0.001 for both). The number of boys in each group was 59 (42.8%), 19 (59.4%), 4 (28.6%), and 3 (50.0%), respectively (P = 0.850). The median duration of hospitalization was 9.5 days (range: 5.0–22.0), 9.5 days (range: 6.0–17.0), 9.0 days (range: 4.0–16.0), and 9.5 days (range: 8.0–23.0), respectively (P = 0.726) (Table 1). The number of febrile days before macrolide treatment in the PMC, CST, DXC, and LFX groups was 4.0 days (range: 0.0–11.0), 4.0 days (range: 0.0–7.0), 3.0 days (range: 0.0–7.0), and 4.0 days (range: 0.0–5.0), respectively (P = 0.326). The number of febrile days during macrolide single treatment in the CST, DXC, and LFX groups was 4.0 days (range: 3.0–14.5), 4.8 days (range: 3.0–7.4), and 4.5 days (range: 3.9–18.0), respectively (P = 0.669) (Table 2).
Table 1
Characteristics of patients with macrolide-unresponsive MP pneumonia in each treatment group

Values are number (%) unless otherwise stated.
MP = Mycoplasma pneumoniae, PMC = prolonged macrolide, CST = corticosteroid, DXC = doxycycline, LFX = levofloxacin.
When additional statistical analysis was preformed, difference only between aPMC vs. LFX (P = 0.007) and bPMC vs. DXC (P = 0.002) was significant. cParainfluenza virus, adenovirus, human bocavirus, corona virus, human metapneumovirus, and respiratory syncytial virus. dSkin rash, hepatitis, myalgia or arthralgia, anemia or thrombocytopenia, and neurologic symptoms. Hepatitis was defined as when alanine aminotransferase exceeded 40 U/L.
![]()
Table 2
The TTD after secondary treatment in patients with macrolide-unresponsive MP pneumonia in each treatment group

TTD = time to defervescence, MP = Mycoplasma pneumoniae, PMC = prolonged macrolide, CST = corticosteroid, DXC = doxycycline, LFX = levofloxacin, SD = standard deviation.
![]()
Defervescence after the change of treatment among the CST, DXC, and LFX groups
After the change to the secondary treatment, the TTD was the shortest in the CST group (8.4 ± 26.8 hours), followed by the LFX (16.8 ± 18.0 hours) and DXC (27.4 ± 33.2 hours) groups (Fig. 1). The numbers of patients who achieved defervescence within 48 hours in CST, DXC, and LFX groups were 31 (96.9%), 12 (85.7%), and 5 (83.3%), respectively (Table 2).
 | Fig. 1The comparison of TTD after secondary treatment between the CST, DXC, and LFX groups.The box displays range from the first quartile to the third quartile and midline of box represents median of TTD after secondary treatment. Error bars represent minimum and maximum of TTD after secondary treatment.
TTD = time to defervescence, CST = corticosteroid, DXC = doxycycline, LFX = levofloxacin.
|
Defervescence after initial macrolide treatment among the PMC, CST, DXC, and LFX groups
The TTDs after initial macrolide treatment were compared in the matched analysis between the PMC group and each secondary treatment group. The TTDs after initial macrolide treatment were not significantly different between PMC and CST groups (5.1 days [range, 3.0–12.2] vs. 4.2 days [range, 3.0–9.0], P = 0.085), PMC and DXC groups (4.9 days [range, 3.2–11.3] vs. 5.7 days [range, 3.4–9.9], P = 0.453), PMC and LFX groups (4.4 days [range, 3.1–6.3] vs. 5.0 days [range, 4.0–6.5], P = 0.283), respectively (Table 3). There was no difference in the length of hospital stay between the PMC group and each secondary treatment group.
Table 3
Comparison of therapeutic efficacy between PMC group and the secondary treatment groups using PS matched analysis

Values are number (%) unless otherwise stated.
PMC = prolonged macrolide, PS = propensity score, CST = corticosteroid, DXC = doxycycline, LFX = levofloxacin, SD = standard deviation, TTD = time to defervescence.
aParainfluenza virus, adenovirus, human bocavirus, corona virus, human metapneumovirus, and respiratory syncytial virus.
![]()
Combined antibiotics, other required treatments, and outcomes
The number of patients who received combined treatment with third-generation cephalosporin was higher in the PMC than other groups. Patients who received combined treatment with vancomycin or needed PCD insertion were identified only in the PMC group. There was no patient who required ICU care and no difference in re-hospitalization rates was found among the groups (Table 4). There was no patient whose clinical symptoms were aggravated after secondary treatment.
Table 4
Combined antibiotics, other required treatments, and outcomes according to the secondary treatment group

Values are number (%) unless otherwise stated.
PMC = prolonged macrolide, CST = corticosteroid, DXC = doxycycline, LFX = levofloxacin, ICU = intensive care unit, PCD = percutaneous catheter drainage.
aCombined use of 3rd generation cephalosporin was significantly different between PMC with corticosteroid or DXC groups (P < 0.001 for both).
![]()
DISCUSSION
The incidence of macrolide resistance of MP has recently increased and has been related to life-threatening or refractory MP pneumonia in children.16 Several studies on macrolide and alternative treatments for MRMP have been reported. However, data on their therapeutic efficacy and safety in children are still limited. We compared the therapeutic efficacy of PMC, CST, DXC, and LFX against macrolide-unresponsive MP pneumonia and collected data about their safety in children. Most of the patient achieved defervescence within 48 hours after the secondary treatment and any side effect was not observed in the CST, DXC, and LFX groups. However, TTD after initial macrolide treatment did not differ significantly between the PMC, CST, DXC, and LFX groups.
Macrolide resistance of MP is genetically determined by the 23S rRNA gene mutation. As there was no difference in the clinical manifestation between macrolide-susceptible M. pneumoniae (MSMP) and MRMP, it is difficult to clinically distinguish MRMP from MSMP. However, it has been reported that the duration of fever after the administration of macrolide was longer in MRMP than MSMP in childhood pneumonia and that persistent fever might suggest the possibility of infection with MRMP. The patients with MSMP achieved defervescence within 48–72 hours in more than 80% of cases after treatment with macrolide.141528 As mycoplasma takes a long time to isolate, antibiotic susceptibility testing is difficult to apply in practical clinical situations. Molecular tests to confirm macrolide resistance are not currently available in Korean hospitals, except in some cases for research purposes. Japanese societies have recommended a change of antibiotics to second-line agents when fever does not subside in 48–72 hours from macrolides administration.28 In this study, macrolide-unresponsive MP pneumonia was defined as persistent fever of ≥ 38.0°C at ≥ 72 hours after macrolide treatment.
In this study, the prevalence of macrolide-unresponsive MP pneumonia was 16.3%, which was much lower than the prevalence of MRMP reported in Korea (87.2% in 2015).14 This discrepancy between macrolide-resistance and macrolide-unresponsiveness indicated that most patients with MRMP pneumonia achieved defervescence within 72 hours after macrolide administration. Matsubara et al.19 demonstrated that 22.7% of MRMP cases showed clinical improvement within 3 days after macrolide treatment. In addition, Suzuki et al.17 reported that fever resolved with the initially prescribed macrolide, without changing antibiotics, for the treatment of MRMP infection, and there was no apparent treatment failure or cases of serious illness. It was suggested that macrolides have anti-inflammatory effects, as well as antimicrobial effects, through the inhibition of the production of cytokines such as IL-6 and IL-8 in human bronchial epithelial cells.2930 In our data, there were no cases of treatment failure in the PMC group, except for two cases of re-hospitalization. In these two cases, defervescence occurred within 24 hours without a change in antibiotics after re-hospitalization.
In some previous reports, systemic CST induced clinical and radiological improvement in severe refractory MP pneumonia.252631 Immune regulatory and anti-inflammatory effects of CST could result in the clinical improvement of severe refractory MP pneumonia.3233 In this study, CST improved fever in the shortest time (8.4 ± 26.8 hours) compared with other medications, which was similar to those reported in other studies. Lee et al.34 reported that 93% of patients with severe MP pneumonia achieved defervescence within 24 hours. In another study, the TTD was approximately 8–48 hours in prednisolone-treated patients.25
Recently, several studies suggested that tetracycline and fluoroquinolone had a therapeutic effect on MRMP in children. Most patients administered DXC or minocycline achieved defervescence within 24 hours, with a significantly shorter TTD than macrolide in the MRMP group (13.5 ± 4.1 vs. 123.3 ± 59.0 hours).2135 Miyashita et al.36 reported that 77% of patients with MRMP in the quinolone group achieved defervescence within 48 hours after the initiation of antibiotics and quinolone was more effective than macrolide for MRMP treatment (P = 0.036). In this study, TTD after DXC and LFX treatment was 27.4 ± 33.2 hours and 16.8 ± 18.0 hours, respectively. In addition, 85.7% and 83.3% of patients achieved defervescence within 48 hours in the DXC and LFX groups, respectively (Table 2). Direct comparison of TTD between the PMC group and the secondary treatment groups was not possible, because all patients were initially treated with macrolide and added on or switched to CST, DXC, and LFX. Therefore, we performed PS matching to adjust differences in baseline characteristics among the groups and compared TTD after initial macrolide treatment between groups. However, the TTDs after initial macrolide treatment of the CST, DXC, LFX groups did not differ from that of each matched PMC group (P = 0.085, P = 0.453, and P = 0.283, respectively). There was no difference in length of hospital stay between the PMC group and the secondary treatment groups (Table 3).
We investigated the frequency of the use of broad-spectrum antibiotics in the treatment of community-acquired pneumonia in children. The number of patients treated with 3rd generation cephalosporin was higher in the PMC group than other groups. In addition, the use of vancomycin was observed only in the PMC group (Table 4). These results suggested that the choice of appropriate second-line agents in the treatment of macrolide-unresponsive MP pneumonia reduced the use of unnecessary broad-spectrum antibiotics.
In the DXC and LFX groups, no side effects such as tooth discoloration or tendinopathy and arthritis were observed. It was reported that tooth staining or color change were not observed in children aged between 2 and 8 years old treated with DXC.37 However, because DXC, approved by the U.S. Food and Drug Administration for children aged ≥ 8 years old, is still contraindicated for children younger than 12 years of age in Korea, the age indications for tetracycline-bound drugs, including DXC, should be reconsidered. In addition, the risk of cartilage injury with LFX was clinically undetectable in children over 5 years old, or was easily reversible.24 Of the 1,340 subjects treated with LFX, only one case (0.07%) was ‘possibly related’ to drug therapy assessed at 5 years, and this was not different from the comparator group (1/893, 0.1%). However, because concerns about the safety of tetracycline and fluoroquinolone in children still exist, it should be cautiously used with the consideration of both the risk and benefit in children with macrolide-unresponsive MP pneumonia.
This study has some limitations. Firstly, as this study was performed retrospectively, the clinical information might be uncertain, especially with regard to the use and duration of macrolide prescribed in other clinics. Secondly, the numbers of patients in DXC and LFX groups were small. In the future, it is necessary to carry out prospective randomized studies or to conduct studies involving more subjects through multicenter studies. Lastly, the IgM antibody test was used to diagnose MP infection. Although the patients with a history of MP infection within past year were excluded, some subjects with false positive could be included due to prolonged existence of IgM for several months after past infection. In addition, false negatives could also exist due to a lack of IgM antibodies in early stages. However, other alternative methods, such as isolation or the molecular detection of MP, cannot differentiate asymptomatic carriage of MP in the nasopharynx from infection or MP pneumonia.
In this study, the macrolide resistance of MP determined by molecular analysis or susceptibility test was not identified. But, this study was based on an actual treatment course for MP pneumonia in a clinical setting. If fever persists despite the use of macrolide, it is necessary to consider a secondary treatment without the results of antimicrobial susceptibility. We compared the therapeutic efficacy of the secondary treatments on clinically assessed macrolide-unresponsive MP pneumonia.
Most of macrolide-unresponsive MP pneumonia patients achieved defervescence within 48 hours with CST add-on or treatment changes to DXC, and LFX, and any side effects were not observed in the secondary treatment groups. However, the secondary treatments did not shorten the duration of fever or hospitalization compared to PMC treatment. A large-scale prospective study is needed to guide appropriate treatment in children with mycoplasma pneumonia.
 XML Download
XML Download