

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intraductal papillary neoplasm of the bile duct (IPNB) is a rare disease entity with a previously reported prevalence of 4% to 15% among bile duct tumors.123 In 2010, the World Health Organization (WHO) (fourth edition, 2010) classified IPNB as dilated intrahepatic bile ducts (IHDs) filled with a noninvasive papillary or villous biliary neoplasm covering delicate fibrovascular stalks.4 As IPNB is a recently defined disease category, and few papers on this condition have been published to date, little is known about the morphologic characteristics or clinicopathologic features of IPNB.
Many previous reports have discussed IPNB as a counterpart of intraductal papillary mucinous neoplasm (IPMN) of the pancreas; both arise in the ductal structures and have a mass with a predominantly papillary pattern.567 However, IPNB has many clinical features that differ from those of IPMN, and whether the same diagnostic and classification criteria can be applied to both conditions is uncertain. Symptoms and elevation of tumor markers are more common in IPNB, and the proportion of malignancy or invasive carcinoma is higher in IPNB than in IPMN. Based on the differential involvement of the pancreatic ductal system, IPMN is classified into main duct, branch duct, and mixed types that are correlated with the histologic subtype and prognosis.8 In IPNB, however, there are considerable differences in the findings among individual researchers owing to the particular characteristics of the biliary tract. Moreover, the clinicopathologic features, prognosis, and surgical methods between lesions of the intrahepatic versus extrahepatic bile ducts (EHDs) are quite different.
Some morphologic features of IPNB have been identified, including diffuse or segmental ductal dilatation and the appearance of an intraductal growing mass. However, little is known about the association between morphological subtypes and the clinicopathologic features of IPNB.910 Although several morphological classifications have been proposed in previous reports, most were based on experiences using a small sample size in a single institution and have never been externally validated. In cases of cholangiocarcinoma, which account for the largest proportion of biliary tumors, traditional anatomical classification (extrahepatic/intrahepatic/hilar cholangiocarcinoma) has been used, and both the treatment strategy and clinical staging vary according to this classification. Although IPNB shows some radiologic features similar to those of cholangiocarcinoma, this simple anatomical classification cannot be applied to the previously suggested morphological classifications of IPNB.
Consequently, the aims of the present study were to clarify the clinicopathologic and morphological characteristics of IPNB, validate the existing classifications using our patient cohort, and establish optimal classification criteria for effective diagnosis and treatment.
METHODS
Patient selection
From January 2003 to October 2016, the data of 112 patients who underwent surgical resection of IPNB were collected in this study. Patients without available preoperative images or postoperative pathologic slides were excluded.
Interpretation of pathologic diagnosis and histologic subtypes of IPNB
A specialized biliary-pancreas pathologist retrospectively reviewed all pathologic slides and reconfirmed the diagnosis of IPNB according to the WHO 2010 criteria. During this process, patients with biliary mucinous cystic neoplasms or other cystic tumors were excluded. The pathologic tumor grades were classified as low- to high-grade dysplasia and invasive carcinoma according to the WHO classification.4 The histologic subtypes of IPNB were divided into four groups: the gastric type (GT), consisting of columnar cells with abundant mucin and clear cytoplasm; the intestinal type (IT), consisting of stratified columnar cells with goblet cells; the pancreatobiliary type (PT), consisting of columnar cells with eosinophilic cytoplasm and a round nucleus; and the oncocytic type (OT), which has been reported as a variant of PT, consisting of abundant eosinophilic cytoplasm and a round nucleus.
Radiologic characteristics of IPNB and anatomical and morphological classifications
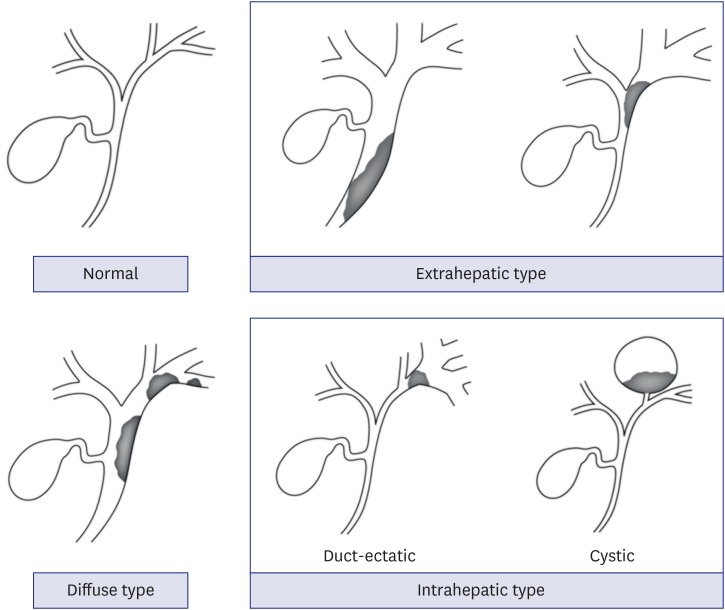
Every patient underwent a quadruple-phase computed tomography (CT) scan including unenhanced, early arterial, late arterial, and venous phases or a triple-phase CT without an early arterial phase. For precise clinical interpretation, these CT images were reconstructed with a 3 mm slice thickness. For some patients with poor CT images, magnetic resonance imaging with magnetic resonance cholangiopancreatography was additionally performed. Based on these CT and magnetic resonance images, radiologists with several years of experience in our pancreatobiliary division determined the location and extent of the mass, wall thickening and stricture formation in the bile duct, and ductal dilatation. Using these radiologic findings, we validated the classification according to the Japan Biliary Association (JBA) definition,10 which is based on dilatation of the bile duct and the presence of cystic formation. Localized duct-ectatic type (I) is including patients with focal dilatation of bile duct and generalized duct-ectatic type (II) with diffuse dilatation of bile duct. Cystic type (III) includes patients with cystic formation of bile duct and mixed type (IV) is combined form of duct-ectatic and cystic types. We also attempted to validate the morphological classification described by Kim et al.9 that is based on dilatation of the bile duct and the presence of an intraductal mass or stricture. Type I is diffuse duct ectasia with a grossly visible papillary mass and type II is diffuse duct ectasia without a visible mass. Type III is an intraductal polypoid mass within localized duct dilatation and type IV is intraductal cast-like lesion. Type V is focal stricture-like lesion and type UC is unclassified cases we added.
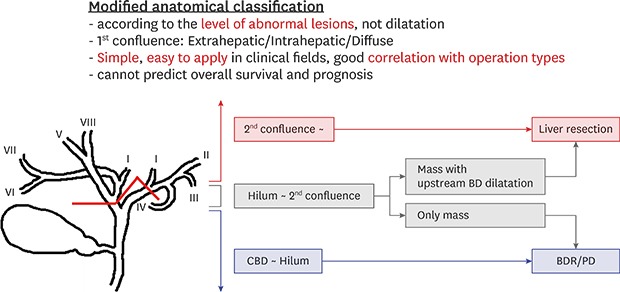
Moreover, to compare the usefulness of these two existing classification systems, we evaluated the patients using “modified anatomical classification” similar to that used for cholangiocarcinoma and based on the level of the main lesions, including intraductal masses, strictures, and wall thickening. For this classification method, we divided the patients into three groups as follows (Fig. 1):
Extrahepatic type: the main lesions were confined to the common bile duct and common hepatic duct
Intrahepatic type: the main lesions were located at the periphery beyond the first confluence of the IHD
Diffuse type: the main lesions were located over a wide range of the IHD and EHD
Furthermore, we divided the intrahepatic type into two subgroups, namely the cystic form and the duct-ectatic form, to clarify the differences according to the shape of the lesions. By comparing these three classifications, we aimed to determine if the “modified anatomical classification” differs from the existing classification systems.
Correlation between the clinicopathologic characteristics of IPNB and anatomical and morphological classifications
To investigate the general characteristics of IPNB, we analyzed its clinicopathologic and radiologic features using preoperative CT as well as the effects of these factors on prognosis and survival. Lesion size was measured radiologically and pathologically, and multiplicity and communication with the adjacent bile duct were also identified. Histologic subtypes were divided into four groups similar to those of IPMN, and histologic grades were defined according to dysplasia and invasive cancer. R1 resection was defined as the presence of cancer in the resection margin, and the depth of invasion was classified according to whether the lesion was confined to the bile duct. We compared the correlation of histologic subtypes with survival and prognosis according to the conventional morphologic classification methods and our “modified anatomical classification.”
Statistical analysis
All statistical analyses were performed using IBM SPSS version 19.0 software (IBM Corp., Somers, NY, USA). Nominal variables were compared using the χ2 test or Fisher's exact test, and continuous variables were compared using Student's t-test or analysis of variance. For binary variables, a logistic regression model was used to identify significant predictors and estimate their odds ratios. Two-sided P values of < 0.05 were considered statistically significant. Survival was analyzed using the Kaplan-Meier method and compared using the log-rank test.
RESULTS
Demographic findings
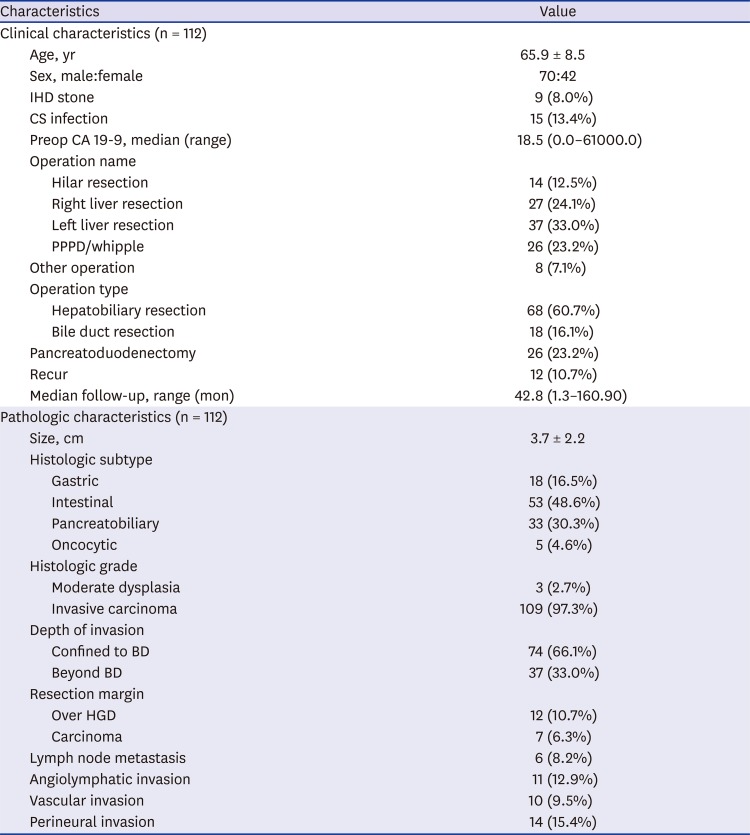
Table 1 shows the patients' demographic findings. Mean patient age was 65.9 years, and the median follow-up period was 42.8 months. On preoperative CT scans, almost all patients showed bile duct dilatation (n = 110; 98.2%) and an intraductal mass (n = 104; 92.9%). Although many of the patients with ductal dilatation were found to have a very wide range of dilatation, we could clearly distinguish the locations of the lesions in the patients with intraductal masses or wall thickening. Among the patients who underwent hepatobiliary resection, a greater proportion underwent left liver resection (n = 37; 33.0%) than underwent right liver resection (n = 27; 24.1%).
Table 1
Patients' characteristics
Pathologic findings
As shown in Table 1, most patients had carcinoma (n = 109; 97.3%), and three patients had moderate dysplasia (2.7%). Given that the T stage according to the WHO classification is applied differently depending on the location of IPNB, we reclassified the tumor according to if it was confined to the bile duct. Among the histologic subtypes, the IT was the most common (n = 53; 48.6%), and the PT was the next most common (n = 33; 30.3%). Seven patients (6.3%) showed a positive resection margin on the final pathologic reports, and only six (8.2%) had lymph node metastasis.
Survival outcome and prognostic factors
The five-year survival rate of all patients was 72.3% (100.0% in the dysplasia group and 71.1% in the carcinoma group) (Fig. 2). The survival curves showed no differences among the four histologic subtypes and morphological classification systems (JBA10, Kim et al.9, and “modified anatomical classification”) (Fig. 3A-D). Patients with a positive resection margin had a five-year survival rate of 25.0%, while those with a negative resection margin had a five-year survival rate of 75.9% (P = 0.003) (Fig. 3E). Moreover, patients with lymph node metastasis showed a lower survival rate than those with no lymph node metastasis, with marginal statistical significance (P = 0.091) (Fig. 3F).
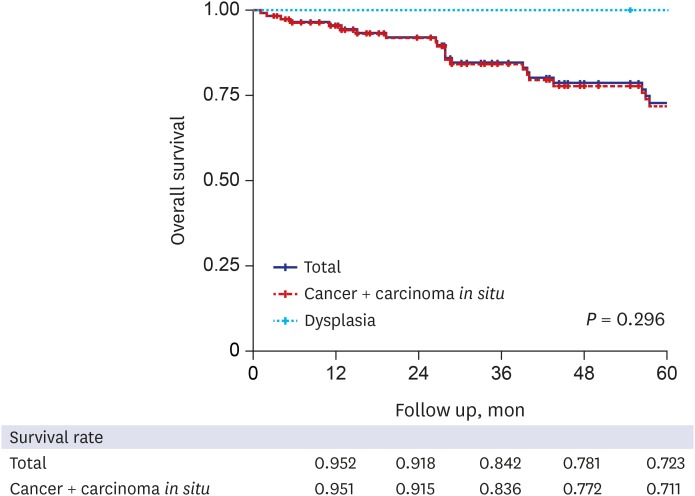
Fig. 3
Overall survival according to the various prognostic factors. (A) Overall survival according to the histologic subtypes. (B) Overall survival according to the JBA classification.10 (C) Overall survival according to the classification by Kim et al.9 (D) Overall survival according to the modified anatomical classification. (E) Overall survival according to the resection margin status. (F) Overall survival according to the lymph node metastasis.
JBA = Japan Biliary Association.
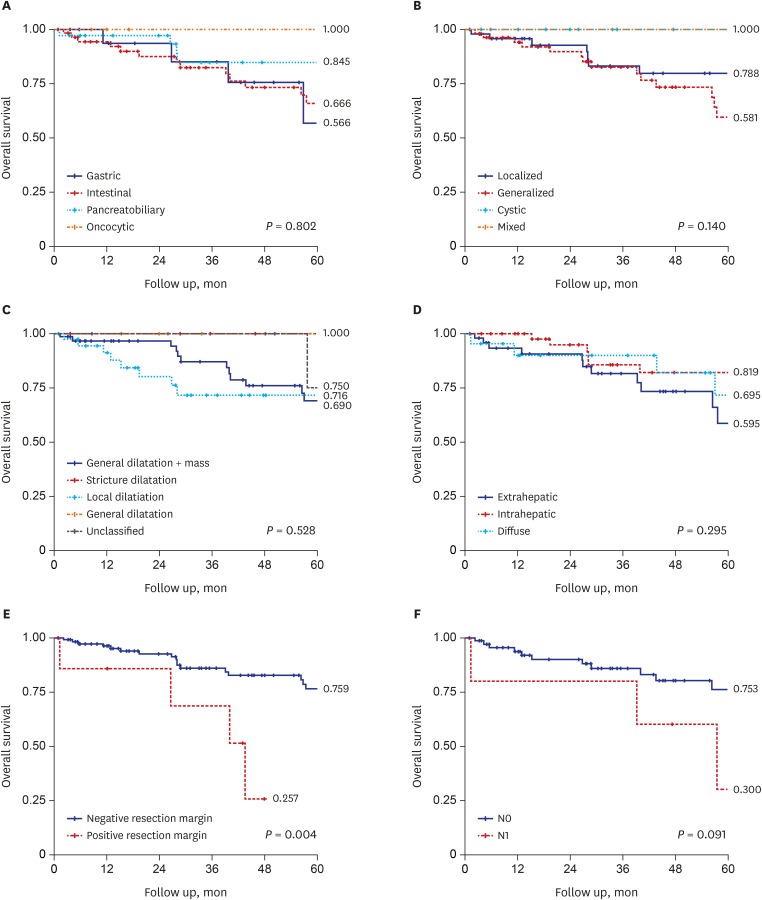
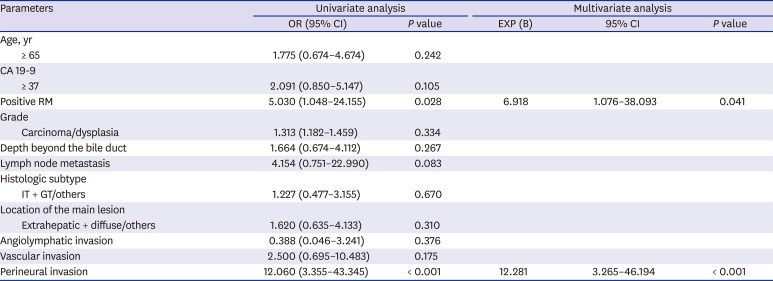
Table 2 shows the univariate and multivariate analysis results. A positive resection margin and perineural invasion were found to be important risk factors in both the univariate and multivariate analyses.
Table 2
Prognostic factors for survival
Radiologic characteristics according to various morphological and anatomical classifications based on preoperative CT
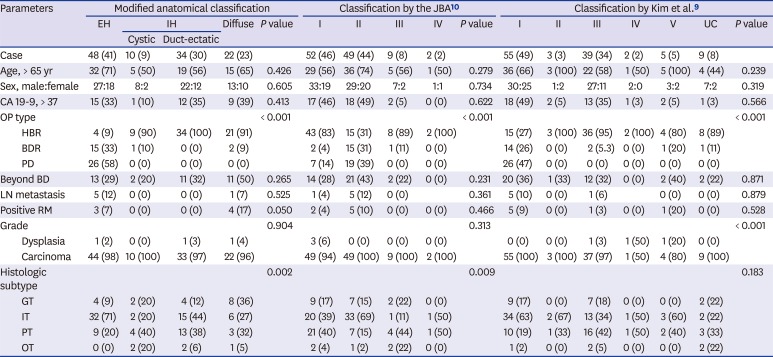
Table 3 shows the clinicopathologic features of IPNB according to the “modified anatomical classification,” which focuses on the level of the main lesions. The extrahepatic type tended to be removed by pancreaticoduodenectomy (PD) or bile duct resection and the intrahepatic type by liver resection. Moreover, patients with diffuse type IPNB had higher rates of positive resection margins (extrahepatic and intrahepatic type vs. diffuse type: 6.7% and 0.0%, respectively, vs. 17.4%; P = 0.020). Among the histologic subtypes, the extrahepatic type had a higher rate of IT, the intrahepatic type had an equally high proportion of IT and PT, and the diffuse type had a higher proportion of GT. In accordance with the JBA classification,10 we further categorized the cystic and duct-ectatic forms. Only intrahepatic type IPNB was allocated to these two subgroups, as this additional classification pertains to lesions surrounded by the hepatic parenchyma. Among those histologic subtypes, we identified a relatively higher proportion of IT in the duct-ectatic form and PT in the cystic form.
Table 3
Clinicopathologic characteristics according to morphological and anatomical classifications
| Parameters | Modified anatomical classification | Classification by the JBA10 | Classification by Kim et al.9 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EH | IH | Diffuse | P value | I | II | III | IV | P value | I | II | III | IV | V | UC | P value | |||
| Cystic | Duct-ectatic | |||||||||||||||||
| Case | 48 (41) | 10 (9) | 34 (30) | 22 (23) | 52 (46) | 49 (44) | 9 (8) | 2 (2) | 55 (49) | 3 (3) | 39 (34) | 2 (2) | 5 (5) | 9 (8) | ||||
| Age, > 65 yr | 32 (71) | 5 (50) | 19 (56) | 15 (65) | 0.426 | 29 (56) | 36 (74) | 5 (56) | 1 (50) | 0.279 | 36 (66) | 3 (100) | 22 (58) | 1 (50) | 5 (100) | 4 (44) | 0.239 | |
| Sex, male:female | 27:18 | 8:2 | 22:12 | 13:10 | 0.605 | 33:19 | 29:20 | 7:2 | 1:1 | 0.734 | 30:25 | 1:2 | 27:11 | 2:0 | 3:2 | 7:2 | 0.319 | |
| CA 19-9, > 37 | 15 (33) | 1 (10) | 12 (35) | 9 (39) | 0.413 | 17 (46) | 18 (49) | 2 (5) | 0 (0) | 0.622 | 18 (49) | 2 (5) | 13 (35) | 1 (3) | 2 (5) | 1 (3) | 0.566 | |
| OP type | < 0.001 | < 0.001 | < 0.001 | |||||||||||||||
| HBR | 4 (9) | 9 (90) | 34 (100) | 21 (91) | 43 (83) | 15 (31) | 8 (89) | 2 (100) | 15 (27) | 3 (100) | 36 (95) | 2 (100) | 4 (80) | 8 (89) | ||||
| BDR | 15 (33) | 1 (10) | 0 (0) | 2 (9) | 2 (4) | 15 (31) | 1 (11) | 0 (0) | 14 (26) | 0 (0) | 2 (5.3) | 0 (0) | 1 (20) | 1 (11) | ||||
| PD | 26 (58) | 0 (0) | 0 (0) | 0 (0) | 7 (14) | 19 (39) | 0 (0) | 0 (0) | 26 (47) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||||
| Beyond BD | 13 (29) | 2 (20) | 11 (32) | 11 (50) | 0.265 | 14 (28) | 21 (43) | 2 (22) | 0 (0) | 0.231 | 20 (36) | 1 (33) | 12 (32) | 0 (0) | 2 (40) | 2 (22) | 0.871 | |
| LN metastasis | 5 (12) | 0 (0) | 0 (0) | 1 (7) | 0.525 | 1 (4) | 5 (12) | 0 (0) | 0.361 | 5 (10) | 0 (0) | 1 (6) | 0 (0) | 0 (0) | 0.879 | |||
| Positive RM | 3 (7) | 0 (0) | 0 (0) | 4 (17) | 0.050 | 2 (4) | 5 (10) | 0 (0) | 0 (0) | 0.466 | 5 (9) | 0 (0) | 1 (3) | 0 (0) | 1 (20) | 0 (0) | 0.528 | |
| Grade | 0.904 | 0.313 | < 0.001 | |||||||||||||||
| Dysplasia | 1 (2) | 0 (0) | 1 (3) | 1 (4) | 3 (6) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (3) | 1 (50) | 1 (20) | 0 (0) | ||||
| Carcinoma | 44 (98) | 10 (100) | 33 (97) | 22 (96) | 49 (94) | 49 (100) | 9 (100) | 2 (100) | 55 (100) | 3 (100) | 37 (97) | 1 (50) | 4 (80) | 9 (100) | ||||
| Histologic subtype | 0.002 | 0.009 | 0.183 | |||||||||||||||
| GT | 4 (9) | 2 (20) | 4 (12) | 8 (36) | 9 (17) | 7 (15) | 2 (22) | 0 (0) | 9 (17) | 0 (0) | 7 (18) | 0 (0) | 0 (0) | 2 (22) | ||||
| IT | 32 (71) | 2 (20) | 15 (44) | 6 (27) | 20 (39) | 33 (69) | 1 (11) | 1 (50) | 34 (63) | 2 (67) | 13 (34) | 1 (50) | 3 (60) | 2 (22) | ||||
| PT | 9 (20) | 4 (40) | 13 (38) | 3 (32) | 21 (40) | 7 (15) | 4 (44) | 1 (50) | 10 (19) | 1 (33) | 16 (42) | 1 (50) | 2 (40) | 3 (33) | ||||
| OT | 0 (0) | 2 (20) | 2 (6) | 1 (5) | 2 (4) | 1 (2) | 2 (22) | 0 (0) | 1 (2) | 0 (0) | 2 (5) | 0 (0) | 0 (0) | 2 (22) | ||||
Data are presented as number (%).
UC = unclassified, EH = extrahepatic, IH = intrahepatic, CA 19-9 = cancer antigen 19-9, HBR = hepatobiliary resection, BDR = bile duct resection, PD = pancreaticoduodenectomy, BD = bile duct, LN = lymph node, RM = resection margin, GT = gastric type, IT = intestinal type, PT = pancreatobiliary type, OT = oncocytic type.
We validated the other two morphological classifications using the preoperative CT images of our patients (Table 3), and a similar tendency was observed in these two categories, although it was more complex than that of the “modified anatomical classification.” The types of surgeries performed were well separated by all three classifications. Using the JBA classification,10 patients with the generalized duct-ectatic type tended to undergo PD, while patients with the other types tended to undergo hepatic resection. Using the classification by Kim et al.,9 to which we added an “unclassified type” because it did not include cystic tumors, only the generalized duct dilatation with mass type (type I) was associated with a high proportion of PD. Among the histologic subtypes in the JBA classification,10 a relatively high proportion of IT in the duct-ectatic form and PT in the cystic form was observed. This finding was similar to that observed using the “modified anatomical classification.”
DISCUSSION
Since 2001, reports of IPNB have been steadily increasing.711 Until it was established as IPNB by the WHO in 2010, this biliary tumor, which is characterized by a large amount of mucin production, a papillary growth pattern, and dilated extrahepatic and IHDs, was referred to by various names, including “mucin-hypersecreting bile duct tumor,” “mucin-producing cholangiocarcinoma,” “biliary papillomatosis,” and “biliary papilloma.”
Several similarities and differences between IPNB and IPMN have been proposed to clarify the clinicopathologic characteristics and establish a new disease category that includes both tumor types.1213 Similar to IPMN, IPNB is a papillary tumor originating from the ductal system with mucin production. However, only one-third of IPNBs present as macroscopic mucin-hypersecreting masses, which distinguishes them from the typical mucin hypersecretion of IPMN.6 Many patients with IPNB have preoperative jaundice and elevated tumor markers (carcinoembryonic antigen and cancer antigen 19-9); in contrast, symptom development and tumor marker elevation are less common in patients with IPMN.14 These two diseases are often divided into four histologic subtypes: the GT, IT, PT, and the OT.15 The predominant forms of IPNB are IT and PT, whereas the predominant forms of IPMN are IT (main duct type) and GT (branch duct type).1516
In terms of pancreatic carcinogenesis, the progression of early lesions, including IPMN or pancreatic intraepithelial neoplasm, to ductal adenocarcinoma or colloid cancer is relatively well understood. In the bile duct, although biliary intraepithelial neoplasm and IPNB are presumed to be precursor lesions, little is known about their exact courses of progression. In 2014, Aishima17 suggested putative models of tumor origin, risk factors, and precancerous lesions of biliary tract carcinoma. However, the pathologic differentiation between biliary intraepithelial neoplasm and IPNB remains ambiguous because these two conditions have similar histology but different clinical or biological manifestations.
We published a report on the clinicopathologic characteristics of IPNB in 2013,18 in which we analyzed macroscopic morphology, multiplicity, and mucin production in 84 patients who underwent surgical resection. From the viewpoint of morphology, microscopic IPNB had the best prognosis followed by pedunculated or sessile IPNB, and diffuse IPNB had the worst prognosis. A positive resection margin and multiplicity were significant independent prognostic factors in the multivariate analysis. Since a better long-term prognosis can be achieved in patients with IPNB by ensuring sufficient surgical resection,3 it is important to accurately localize the main lesions and establish a proper extent of resection based on the preoperative radiologic images. The main principle of surgery for conventional cholangiocarcinoma is very similar.1920
Previously suggested classifications have commonly focused on the ductal dilatation of IPNB. Kubota et al.10 from the JBA suggested a new classification system based on the extent and shape of ductal dilatation. However, this system is limited in its evaluation of the stricture site and wall thickening. Kim et al.9 proposed another morphological classification that focused on the extent of ductal dilatation and the presence of an intraductal mass, which also has some pitfalls, most importantly, tumors with the cystic form are not considered. Although these two classification systems are the most representative of the various previously established classifications, the clinicopathologic characteristics of each subgroup were not significantly different, and the systems are very complex to apply in clinical practice.21
Most patients in our study cohort had a specific point lesion regardless of the presence of ductal dilatation (intraductal mass, 92.9%; wall thickening or stricture, 14.3%). With recent improvements in the resolution of radiologic images, the likelihood of discovering tiny lesions (intraductal mass, stenosis, or bile duct wall thickening) is increasing. As IPNB is a surgical disease, the surgeons' major concern during the operation is determining the location of these main lesions, not the degree of expansion of the bile duct caused by mucin hypersecretion. If focus is on the dilatation of bile duct only, it is difficult to determine the precise location of the lesion and obtain information linked to treatment and prognosis, such as the tumor burden.
We generally categorize cholangiocarcinoma, a malignant tumor arising from the biliary epithelium, as either intrahepatic or extrahepatic based on the anatomical location of the tumor. Even according to the American Joint Committee on Cancer staging system, which is the most commonly used system in clinical practice, the extrahepatic and intrahepatic classification is applied for the staging of cholangiocarcinoma. The reason for using this anatomical classification is that the stage, prognosis, surgical extent, and the clinical and biological characteristics differ markedly between extrahepatic and intrahepatic cholangiocarcinoma. Although the location, morphology, and surgical extent of IPNB closely resemble those of cholangiocarcinoma, this anatomical classification has not been considered for IPNB. By applying this simple anatomical classification of cholangiocarcinoma to IPNB based on the main lesions, patients could receive a clearer diagnosis and undergo the optimal operation with a better prognosis.
In the “modified anatomical classification” system, the boundary of the extrahepatic and intrahepatic types is the first confluence. This system is very simple and intuitive, which makes it easy to determine which type of surgery to perform. In the present study, when the lesion was classified as the extrahepatic type, the operation tended to be bile duct resection or PD, whereas the operation tended to be liver resection when the lesion was the intrahepatic type. Moreover, because diffuse type IPNB was characterized by a significantly higher proportion of multiple masses on preoperative CT images, the proportion of hepatobiliary resections was higher than that of other types of surgery; expanding the extent of the operation should be considered in order to obtain a negative resection margin. The “modified anatomical classification” yielded a simpler and clearer correlation between the clinicopathologic characteristics and the types of surgical resection as in contrast to the classifications by the JBA10 and Kim et al.9
When comparing the histologic subtypes, all classifications had some common tendencies: tumors associated with extrahepatic duct dilatation had a higher rate of IT, while tumors with cystic formation had a higher rate of PT. Using the “modified anatomical classification,” the extrahepatic type had a greater proportion of IT, and intrahepatic type tumors had double peak rates of IT and PT. Furthermore, the proportion of IT in the duct-ectatic form and PT in the cystic form were relatively high. This correlation could represent a new finding of IPNB, since the rate of patients with IT is higher for the main duct type in IPMN, and the rate of patients with GT and PT is higher for the branch duct type.8
None of these three morphological and anatomical classifications showed any significant differences in the survival analysis; in addition, the four histologic subtypes did not affect the overall survival of the patients. This trend was also reported in a previous study on IPMN, in which lymphatic spread, an increased T stage, and positive surgical margins were more strongly associated with a poor prognosis than the histologic subtypes.162223 Only patients with a positive resection margin had significantly lower overall survival than those with a negative margin in this study. Several reports have suggested that the presence of invasive components in the surgical margin is associated with poor survival in IPNB.242526 We previously compared the distance to the resection margin between papillary pattern cholangiocarcinoma and other types of cholangiocarcinoma. Our findings suggested that a longer resection margin is needed for cholangiocarcinoma with a papillary pattern than with a nodular pattern (16 vs. 10 mm, respectively).27 Under the guidance of this “modified anatomical classification” system, surgeons can more easily define the optimal extent of resection with a sufficient resection margin.
We gathered a homogenous cohort of patients with IPNB from a single center over a long period of time in Korea, where the incidence of bile duct tumors is very high, and the data were confirmed upon strict review by a specialized pathologist with extensive experience. Since our study was retrospective in design and had a relatively small sample size, a validation study involving a larger population and prospectively collected data will be necessary to validate our findings.
In conclusion, owing to improvements in the resolution of radiologic images, the “modified anatomical classification,” which focuses on the location of the main lesions (intraductal mass, stricture, and wall thickening), was found to adequately predict the clinicopathologic features of IPNB and may help to optimize the strategy and extent of operation.
 XML Download
XML Download