

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Utilization of hospice palliative care (HPC) for patients with terminal illness is increasing globally.123 Nonetheless, there remains a significant unmet need for HPC.4 Moreover, the demand for HPC is expected to increase among aging populations.1
Previous studies have revealed that most patients are referred to HPC late in the course of their illness. The median survival from initial HPC enrollment to patient death ranges from 17 days to 1.9 months, and 9%–25% of the patients die within a week after their initial referrals.5678910 According to the literature, the reason for the delay in the use of HPC among terminal cancer patients is related to the patients themselves, their family caregivers and physicians, and health care systems. Patients who are unaware of their terminal status and whose family caregivers have negative impressions toward HPC are likely to end up with a late referral to HPC.1112 Barriers related with physicians include a lack of knowledge, negative perceptions of HPC, difficulties with communicating poor prognosis to patients or caregivers, and late discussions about HPC.13 Finally, a lack of accessibility to HPC and complicated admissions criteria delay and deter the use of HPC among terminal cancer patients.1314
Although the first hospice clinic in Korea opened in 1965, HPC developed very slowly up until 2000. Government policies for HPC developed in 20051516 have resulted in a significant increase in the number of designated hospice palliative care units (HPCUs) throughout Korea, which as of 2016 totaled 76.5 However, the utilization of HPC among Korean cancer decedents has been reported as low as 15.0% in 2015.5 Moreover, almost half of patients who were admitted to an HPCU died within 15 days.5 In other words, a considerable number of terminal cancer patients use HPCU at a time only when their life expectancy is short.
Various factors are thought to influence decisions on place of care for terminal cancer patients. According to a survey of 108 bereaved family members in 1998, terminal cancer patients received medical care through hospitalization (45.4%), outpatient clinics (22.2%), and the emergency department (16.7%).17 Meanwhile, although there has been a change in efforts to improve awareness of HPC and the number of HPCUs, recent data on the patterns of utilization for places of care among terminal cancer patients are lacking. In addition, even though palliative care consultations have been found to promote discussion of plans and preferences for future care among patients and their families,18 there has been no study on health care utilization of terminal cancer patients after consultation with a palliative care team (PCT) in Korea.
Therefore, this study aimed to investigate; 1) factors related with utilizing HPCU and 2) how these changed between 2010 and 2014 among terminal cancer patients in Korea.
Go to : 
METHODS
Study design and participants
We performed a retrospective analysis of medical records for terminal cancer patients who were referred to the PCT of the National Cancer Center in Gyeonggi, Korea in 2010 and 2014. Patients who selected medical facilities as their place of care after PCT consultation were included in this analysis. Patients who opted for staying home and who did not decide on a place of care were excluded.
Oncology physicians with the National Cancer Center referred terminal cancer patients to the PCT, which consisted of a physician specializing in HPC and an advanced practice nurse. Patients were diagnosed with terminal cancer if they had advanced cancer without response to chemotherapy or if they were not able to receive radical treatment due to deteriorating condition or refusal of chemotherapy. The PCT assessed the patients and discussed with the patients and/or their caregivers to establish care plans, including place of care. In addition, the PCT controlled the patients' physical and psychological symptoms, provided psychosocial support for the patients and their family, and explained HPC. After the PCT recommended an appropriate place of care in accordance with the patients' medical condition and patient/caregiver demands, the patients and their caregivers decided on the place of care.
Data acquisition and analysis
From electronic medical records, we collected each patient's age, sex, primary site of cancer, level of education, residential area, marital status, and religion. Using medical records and consultation records, we obtained information on who received consultation, the patient/caregiver's awareness of terminal status and preferred place of care.
Awareness of terminal status of patient and family was evaluated on first interview for consultation. Preferred place of care was evaluated on first interview and before discharge. Choices for place of care comprised HPCU, current hospital, other general hospital, long-term hospital and home. For comparison with HPCU, current hospital, other general hospital, long-term hospital were categorized as non-HPCU. Home was excluded from analysis because the frequency of preferring home was too small to analyze related factors. When a non-HPCU was a preferred place of care, we asked the interviewed patient and family why HPCU was not chosen as a place of care and documented the reason. If the preferred place of care or reason for not preferring HPCU had been changed before discharge, the final decision for place and reason for not choosing HPCU was recorded.
The recorded reasons for not choosing HPCU included 13 items. Based on grounded theory, authors analyzed the themes in these 13 reasons and developed 4 categories as following; “refusing hospice facility”, “near death”, “poor accessibility to HPCU,” and “caregiving problems”.
“Refusing hospice facility” comprised reasons that patients or their caregivers refused to utilize hospice facility as they wished to have further anti-cancer treatment, or they had negative impression toward hospice care, or they only preferred current hospital and declined transfer. “Near death” was defined as a case in which death was predicted within a few days on evaluation. “Poor accessibility to HPCU” referred to the lack of an available HPCU near the patient's residence or available beds at the HPCU. “Caregiving problems” signified that the patient did not have any family caregiver or could not afford to hire a paid caregiver. Two authors reviewed the medical records independently, determining and assigning data to their appropriate reasons and categories. If there were more than one reason for preferring a non-HPCU, two authors reviewed the medical records and consultation record to allocate the dominant reason. We reviewed discharge records to verify which medical facilities the patients actually used after consultation.
Statistical analysis
Descriptive statistics were used to summarize the characteristics of the patients, place of care, and reasons for selecting non-HPCUs. The patients/caregivers' characteristics of the HPCU and non-HPCU groups were compared using the χ2 test for categorical data and Student's t-test for continuous data. We performed binomial logistic regression analysis with a backward selection algorithm to investigate factors related to the participants' decision to utilize HPCU. Multinomial logistic regression analysis with a backward selection algorithm was used to identify factors related to the patients' decisions to utilize individual subcategories of non-HPCU facilities and their reasons for choosing a non-HPCU, compared with HPCUs. All statistical analyses were conducted using STATA, version 12.0 (STATA Corp., College Station, TX, USA), and a P < 0.05 was considered statistically significant.
Ethics statement
This study was reviewed and approved by the Institutional Review Board (IRB) of the National Cancer Center (IRB No. NCC2016-0251).
Go to :
RESULTS
A total of 1,070 terminal cancer patients were referred to the PCT in 2010 and 2014. Among these, 15 patients were excluded because they selected their home for the place of care, and 27 patients who were reluctant to decide on a place of care were also excluded. Finally, 1,028 terminal cancer patients were included in this study.
General characteristics of the participants
Table 1 summarizes the characteristics of patients according to their decisions on HPC. The number of referred patients increased from 388 in 2010 to 640 in 2014. The mean age of the patients was 61.0 ± 12.2, with 55.1% of the patients being male. The most common diagnosis was lung cancer (24.3%), followed by stomach cancer (13.8%). While 44.6% (n = 173) of referred patients used HPCUs after consultation in 2010, this increased to 53.9% (n = 345) in 2014. Univariable analyses showed that the year, patient's age, and patients/caregivers' awareness of terminal illness influenced HPCU use.
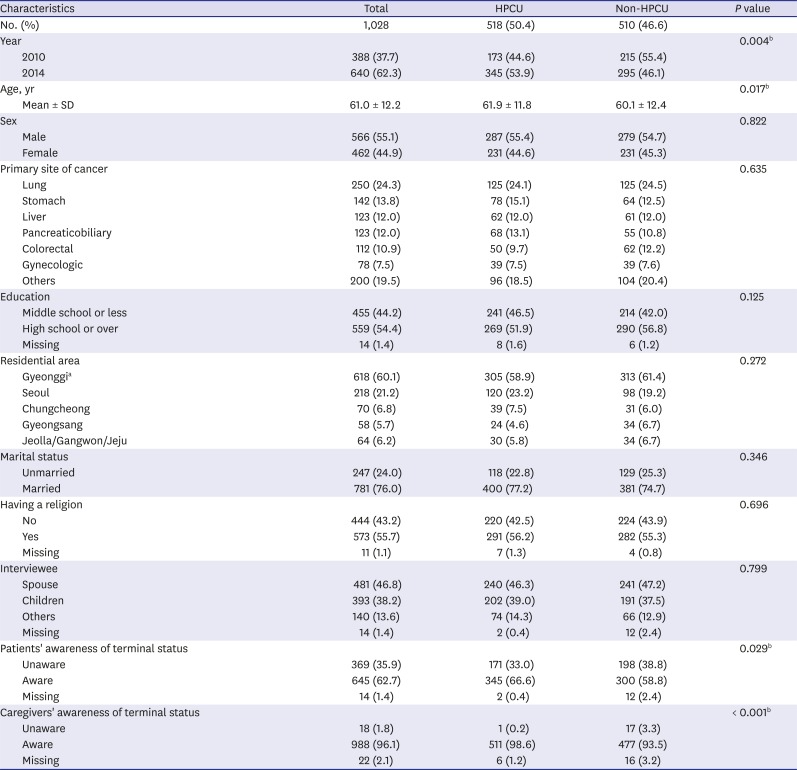
Table 1
General characteristics of the patients
HPCU = hospice-palliative care unit, SD = standard deviation.
aWhere the National Cancer Center is located; bP < 0.05.
![]()
Factors related to choosing an HPCU
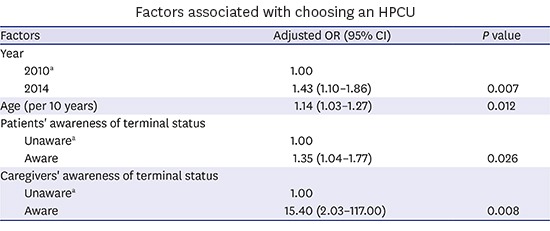
Table 2 presents the factors significantly related to deciding to use HPCUs according to binomial logistic regression analysis. Compared with 2010, patients who were referred in 2014 were more likely to use HPCUs (odds ratio [OR], 1.43; 95% confidential interval [CI], 1.10–1.86). Older age (OR, 1.14; 95% CI, 1.03–1.27) and awareness of the patients' terminal condition by the patients (OR, 1.35; 95% CI, 1.04–1.77) and their caregivers (OR, 15.40; 95% CI, 2.03–117.00) were positively associated with choosing HPCU.
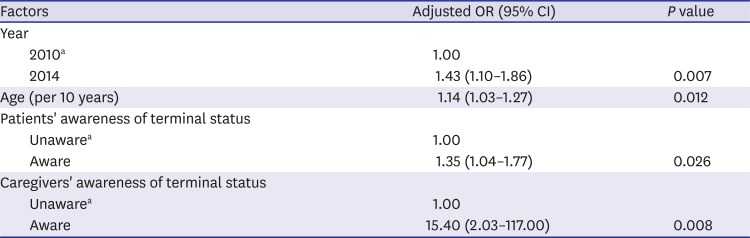
Table 2
Factors associated with choosing an HPCU
Binomial logistic regression analysis with backward selection.
HPCU = hospice-palliative care unit, OR = odds ratio, CI = confidence interval.
aReferences.
![]()
Factors affecting decisions on place of care among non-HPCU group patients
Table 3 shows the results of the multinomial logistic regression for places of care. Among participants who did not choose an HPCU, 290 (56.9%) patients decided to receive care in the current hospital, while 132 (25.9%) and 88 (17.2%) patients selected other general hospitals and long-term hospitals, respectively. Patients who received palliative care consultations in 2014 were less likely to use other general hospitals (OR, 0.40; 95% CI, 0.26–0.59) and a long-term hospital (OR, 0.38; 95% CI, 0.24–0.62), compared to those who did in 2010. Older patients were related with less utilization of the current hospital and increased utilization of long-term hospitals. Patients who lived in Jeolla, Gangwon, and Jeju provinces were negatively associated with choosing current hospitals and positively associated with choosing other general hospitals. Patients aware of terminal illness were less likely to choose other general hospital. Caregivers aware of terminal condition were less likely to utilize current hospital and long-term hospital.
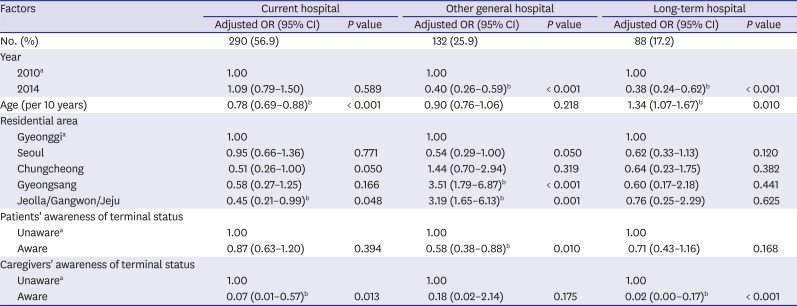
Table 3
Factors associated with choosing a non-HPCU according to eventual place of care
Multinomial logistic regression analysis with backward selection (reference group: patients who selected an HPCU).
HPCU = hospice-palliative care units, OR = odds ratio, CI = confidence interval.
aReference; bP < 0.05.
![]()
Factors related to reasons for selecting non-HPCUs
The most common reason for not selecting an HPCU was “refusing hospice facility” (34.9%), followed by “near death” (34.7%), “poor accessibility to HPCU” (17.7%), and “caregiving problems” (12.7%) (Table 4). Among the patients of “refusing hospice facility,” 46.6% (n = 83) did not want to move to other hospitals and preferred staying at current hospital, 29.2% (n = 52) rejected hospice care itself, and 24.2% (n = 43) opted for further treatment for cancer. There was no significant change of proportion of cases for these reasons under “refusing hospice facility” between 2010 and 2014 (data not shown). Compared to 2010, poor accessibility and caregiving problems were less likely to be reasons why patients did not choose an HPCU in 2014 (OR, 0.32 and 0.47, respectively; 95% CI, 0.19–0.52 and 0.27–0.81, respectively). Older patients were more likely to use a non-HPCU for caregiving problems. Patients in most residential areas were associated with poor accessibility to an HPCU, with the exception of Seoul (OR, 0.28; 95% CI, 0.11–0.74). Awareness of terminal status by caregiver showed negative associations with “refusing hospice facility” and “caregiving problems.”
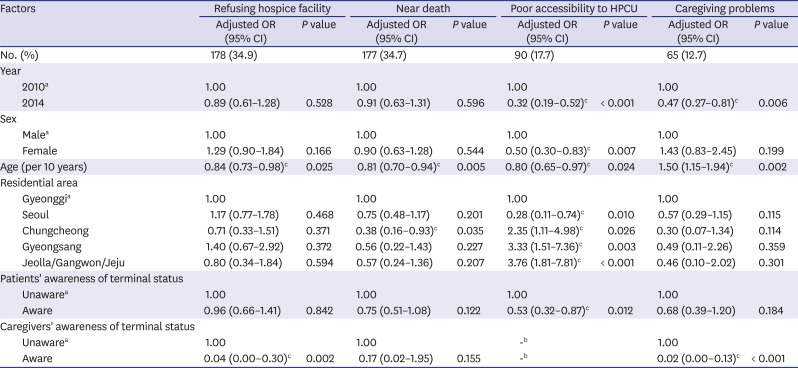
Table 4
Factors associated with reasons for deciding on a non-HPCU
Multinomial logistic regression analysis with backward selection (reference group: patients who selected HPCU).
HPCU = hospice-palliative care units, OR = odds ratio, CI = confidence interval.
aReference; bIn the “Poor accessibility to HPCU” group, all caregivers were aware of terminal status; cP < 0.05.
![]()
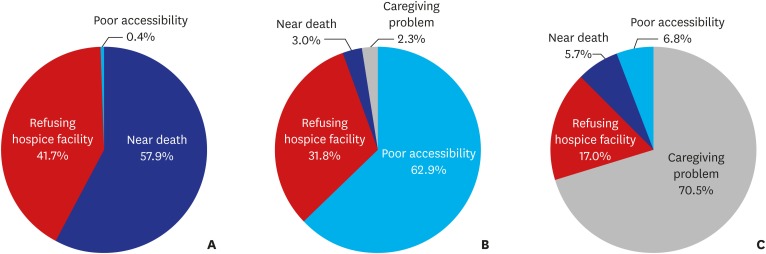
Reasons for selecting non-HPCUs according to chosen places of care
Among non-HPCU patients, there was a significant difference in the reasons for selecting their chosen place of care (P < 0.001, Fig. 1). The most common reason for choosing their current hospital was “near death” (57.9%), and the second was “refusing hospice facility” (41.7%). 62.9% of the reasons for choosing other general hospitals was “poor accessibility to HPCU.” The majority (70.5%) of patients who chose long-term hospitals were unable to choose an HPCU due to “caregiving problems.”
Go to :
DISCUSSION
To the best of our knowledge, this is the first study to explore decisions on utilizing HPCU and factors related therewith among terminal cancer patients after consultation with a PCT in Korea. The largest number (50.4%) of referred patients decided to use a HPCU, followed by their current hospital, other general hospitals, and long-term hospitals. The rate of HPCU utilization was much higher than that of all cancer decedents during the same time period in Korea (10.6% in 2010 and 13.8% in 2014).5 The first reason for the high rate of HPCU utilization in our study could be that the patients and their caregivers were provided accurate information on HPC during consultation with the PCT. This result was consistent with those from previous studies suggesting that palliative care consultation is associated with increased hospice utilization.1819 The second reason was that the accessibility to HPCU was relatively fair among participants, since 81.3% of participants lived in Seoul and Gyeonggi, where HPCUs are concentrated.5 Finally, the oncologist's knowledge of HPC might have affected their referral to PCT: oncologists without information about HPC might not refer their patients to PCT, while those knowledgeable in HPC would likely refer more patients to PCT.
The selection of HPCUs for terminal cancer patients after consultation increased in 2014, compared to 2010, while the selection of other general hospitals and long-term hospitals decreased. We speculate that the main reason for the increased use of HPCUs is that the number of HPCUs in Korea increased from 42 in 2010 to 57 in 2014.5 This is supported by our findings that the percentage of patients who decided to use a non-HPCU due to “poor accessibility to HPCUs” decreased in 2014, compared to 2010.
In our study, the utilization of HPCU increased and “Refusing hospice facility” decreased as the patients' age increased. This is in line with findings from earlier Asian studies, which reported that elderly patients were more likely to receive hospice care and preferred palliative care.2021 This may be due to the fact that many Asians view aging and death in the elderly as natural processes and are more likely to receive non-invasive treatments.20 By contrast, older patients tend to use HPC less in Western countries.22 This is because fairness and justice for the utilization of medical resources are also emphasized for elderly patients. Thus, they are not excluded from aggressive cancer treatment.23 In addition, our study demonstrated that the use of long-term hospitals and “caregiving problems” increased with advancing age. Caregivers are in high demand for end-of-life care,24 especially among elderly patients with comorbidities.25 If there are “caregiving problems,” such as a lack of family members to provide care or financial support for hiring caregivers, it is inevitable to use long-term hospitals where the cost of caregiving is lower than that for an HPCU. The Korean government has begun providing health insurance for hiring paid caregivers in HPCUs since July 2015. Therefore, it is expected that the burden from caregiving for patients and their families in HPCUs will be reduced in the future.
In this study, 63.6% of patients and 98.2% of family caregivers were aware of the terminal illness when they were referred to the PCT. Patients aware of their terminal status among all terminal cancer patients who pass away at HPCUs has increased as years have passed in Korea, from 67.3% in 2010 to 77.6% in 2015.5 The present study showed that patients and caregivers aware of their terminal illness were positively associated with utilization of HPCUs and less use of other general hospitals. All of the reasons for selecting non-HPCUs, except for “near death,” were related to unawareness of terminal status. These findings are in accordance with previous studies that reported patients aware of their terminal illness were more likely to use palliative care.26 The results support the importance of adequate disclosure of terminal illness and communication about end-of-life care, including transition to palliative care.27
“Near death” remained as a major reason for not selecting an HPCU in 2014 in comparison to 2010. This indicates that the timing of referral to the PCT is still too late in Korea, and this late referral pattern has not improved during study period. Late referrals to palliative care have a negative impact on patients, such as inadequate pain and symptom control, failure to discuss advance care planning, and increased in-hospital mortality.2829 A previous study suggested that inadequate communication about preferred end-of-life care with physicians was a reason for late referrals to the palliative care unit.12 We suggest that bringing forward the timing of discussing end-of-life care and introducing HPC is necessary. Additionally, we expect that improving perceptions and knowledge of HPC through public relations and education will help reduce refusal of hospice care and promote early referral.
Although “poor accessibility to HPCUs” decreased in 2014, compared to 2010, it was higher in Chungcheong, Gyeongsang, Jeolla, Gangwon, and Jeju provinces than in metropolitan areas (Seoul, Gyeonggi). The regional disparity in HPCUs was similar to that reported in other countries.130 The number of HPCUs increased by 15 in 2014, compared to 2010; however, 10 of them were newly established in metropolitan areas.5 Even though the number of HPCUs has increased in Korea, this uneven distribution has not yet been resolved. Active intervention from the government may be necessary in order to solve the regional imbalance in HPCUs. Possible interventions include inducing appropriate supply to meet demands and developing a comprehensive HPC program within the community.
This study has a few limitations. First, the study was undertaken at a single institution, and thus, the findings may not be applicable to all terminal cancer patients. Second, we were not able to collect information on certain variables that could influence health care utilization, such as socioeconomic status. Third, data on place of final care or death were not available; a few of the participants could have changed their place of care after discharge. Lastly, the patients' awareness of their terminal illness was ascertained from family caregivers, and thus, there might have been some inconsistency in their actual awareness.
In conclusion, the use of HPCUs in Korea increased between 2010 and 2014. When patients and family members were aware of the terminal condition, they were likely to choose HPCU. Therefore, improving awareness of disease status among patients and family members through communication would be necessary to promote HPCU utilization. Considering many patients couldn't utilize HPCU for “near death,” the discussion for end-of-life care needs to be initiated earlier.
Go to :
 XML Download
XML Download